1
L2 Gynecology D. Huda Adnan
Chronic Pelvic Pain
Definition
Chronic Pelvic Pain (CPP) is pain of apparent pelvic origin that has been present most of the time
for the past six months
Incidence
Affects 15-20% of women of reproductive age
Accounts for 20% of all laparoscopies
Accounts for 12-16% of all hysterectomies
Associated medical costs of $3 billion annually
25-50% of women had more than one diagnosis
Severity and consistency of pain increased with multisystem symptoms
Most common diagnoses:
o endometriosis
o adhesive disease
o irritable bowel syndrome
o interstitial cystitis
2
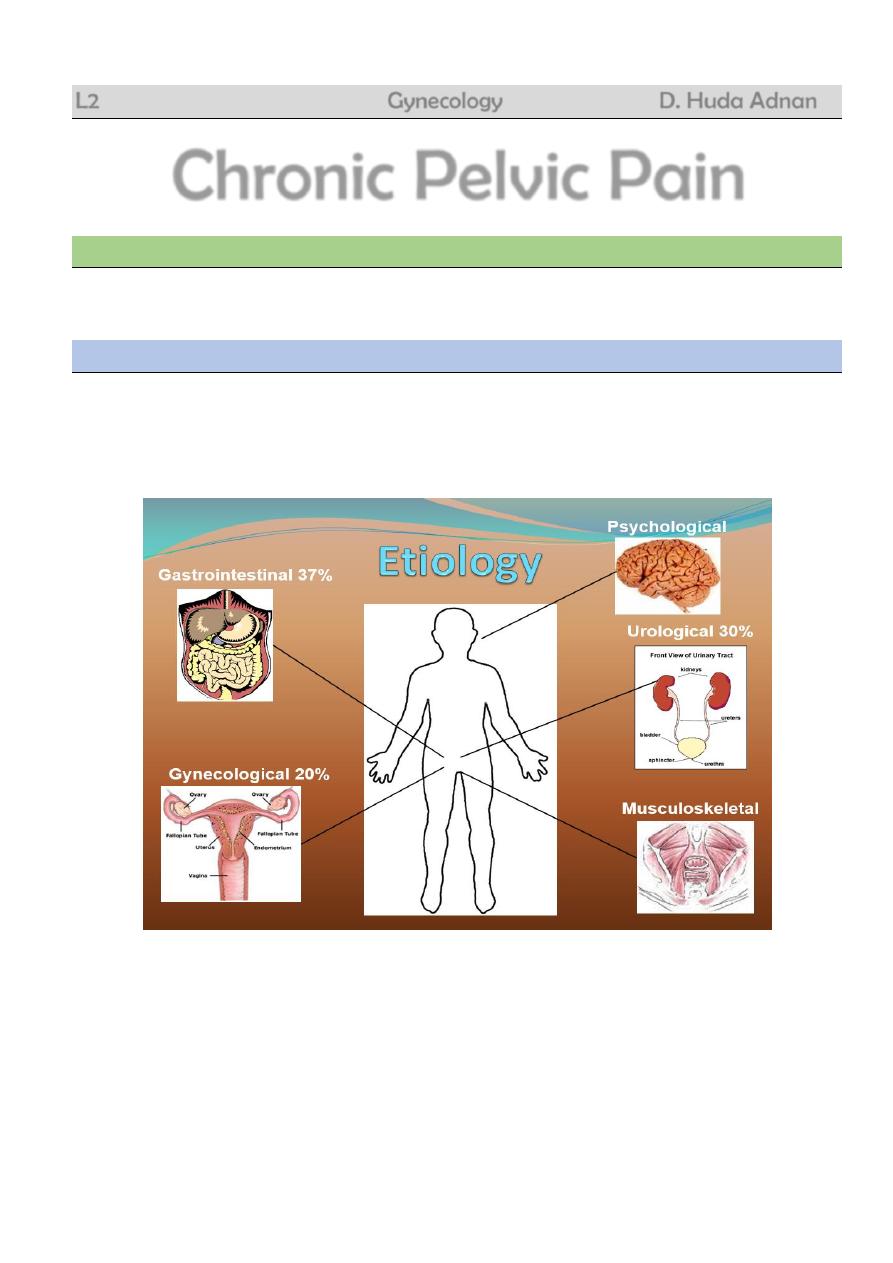
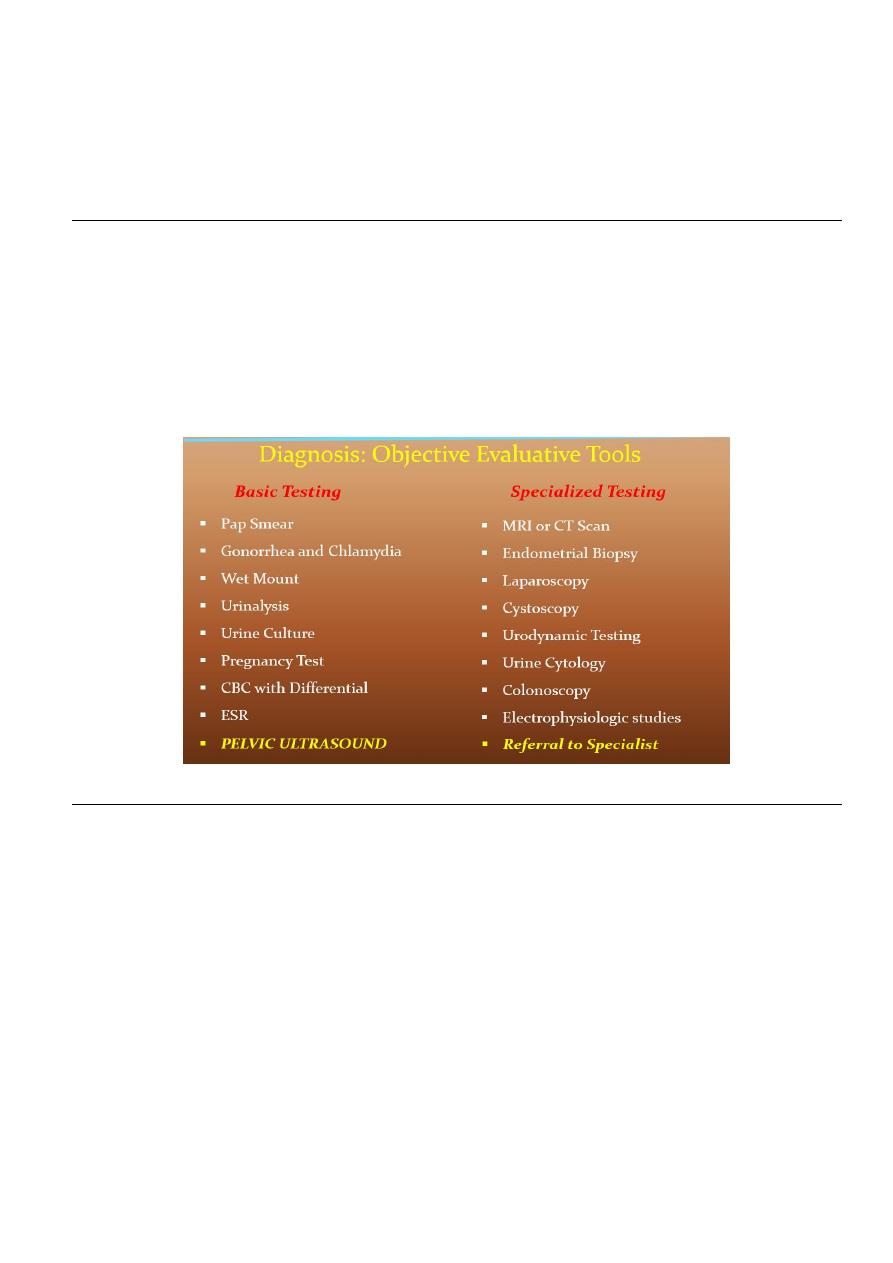
Diagnosis
Obtaining a COMPLETE and DETAILED HISTORY is the most important key to formulating a
diagnosis
Diagnosis: Obtaining the History
Gynecological Review of Systems
Associated with menses?
Association with sexual activity? (Be specific)
New sexual partner and/or practices?
Symptoms of vaginal dryness or atrophy?
Other changes with menses?
Use of contraception?
Detailed childbirth history?
History of pelvic infections?
History of gynecological surgeries or other problems?
Gastrointestinal Review of Systems
Regularity of bowel movements?
Diarrhea/ constipation/ flatus?
Relief with defecation?
History of hemorrhoids/ fissures/ polyps?
Blood in stools, melena, mucous?
Nausea, emesis or change in appetite?
Abdominal bloating?
Weight loss?
Urological Review of Systems
Pain with urination?
History of frequent or recurrent urinary tract infxn?
Hematuria?
Symptoms of urgency or urinary incontinence?
Difficulty voiding?
History of nephrolithiasis?
Musculoskeletal Review of Systems
History of trauma?
Association with back pain?
Other chronic pain problems?
Association with position or activity?
Psychological Review of Systems
History of verbal, physical or sexual abuse?
3
Diagnosis of psychiatric disease?
Onset associated with life stressors?
Exacerbation associated with life stressors?
Familial or spousal support?
Diagnosis: The Physical Exam
Abdomen
Anterior abdominal wall
Pelvic Floor Muscles
Vulva
Vagina
Urethra
Cervix
Viscera – uterus, adnexa, bladder
Rectum
Rectovaginal septum
Coccyx
Lower Back/Spine
Posture and gait
A bimanual exam alone is NOT sufficient for evaluation
Differential Diagnosis: Gynecological Conditions
Cyclical
Endometriosis
Adenomyosis
Primary Dysmenorrhea
Ovulation Pain/ Mittleschmertz
Ovarian Remnant Syndrome
Non-cyclical
Pelvic Masses
Adhesive Disease
Pelvic Inflammatory Disease
Pelvic Congestion Syndrome
Symptomatic Pelvic Organ Prolaps
Pelvic Floor Pain Syndrome

4
Pelvic Inflammatory Disease
Description
: Spectrum of inflammation and infection in the upper female genital tract
Endometritis/ endomyometritis
Salpingitis/ salpingoophritis
Tubo-ovarian Abscess
Pelvic Peritonitis
Pathophysiology
: Ascending infection of vaginal and cervical microorganisms
Chlamydia and Gonorrhea (developed countries)
Tuberculosis (developing countries)
Acute PID usually polymicrobial infection
Risk Factors
Adolescent
Multiple sexual partners
Greater than 2 sexual partners in past 4 weeks
New partner in the past 4 weeks
Prior history of PID
Prior history of gonorrhea or chlaymdia
Smoking
None or inconsistent condom use
Instrumentation of the cervix
Minimum Criteria (one required):
Uterine Tenderness
Adnexal Tenderness
Cervical Motion Tenderness
No other identifiable causes
Additional criteria for dx:
Oral temperature greater than 101
Abnormal cervical or vaginal discharge
Presence of increased WBC in vaginal secretions
Elevated ESR or C-reactive protein
Documented of CT
Specific criteria for dx:
Pathologic evidence of endometritis
US or MRI showing hydrosalpinx,
Laparosopic findings consistent with PID
5
Treatment:
Multiple outpatient antibiotic regimens; total therapy for 14 days.
A) CEFTERIAXON 500 mg im single dose and doxycycline 100 mg twice daily plus
metronidazole 400 mg twice daily.
B) ofloxacin 400 mg twice daily plus metronidazole twice daily.
Inpatient regimens in form of i.v. cefteriaxon 2g daily plus i.v. or oral doxycycline 100 mg BD
followed by oral doxycycline 100 mg BD plus metronidazole 400 mg BD.
Surgical intervention
Laparoscopy to confirm the diagnosis
Drainage of abscess
Treatment of concomitant diseases.
Sequelae
Infertility
Ectopic Pregnancy
Chronic Pelvic Pain
Occurs in 18-35% of women who develop PID
May be due to inflammatory process with development of pelvic adhesions
Pelvic Congestion Syndrome
Description
: Retrograde flow through incompetent valves venous valves can cause tortuous and
congested pelvic and ovarian varicosities; Etiology unknown.
Symptoms
: Pelvic ache or heaviness that may worsen premenstrually, after prolonged sitting or
standing, or following intercourse
Diagnosis
: Pelvic venogrpahy, CT, MRI, ultrasound, laparoscopy
Treatment
: Progestins, GnRH agonists, ovarian vein embolization or ligation, and hysterectomy
with bilateral salpingo-oophorectomy (BSO)
Pelvic Floor Pain Syndrome
Description
: Spasm and strain of pelvic floor muscles
Levator Ani Muscles
Coccygeus Muscle
Piriformis Miscle
Symptoms
: Chronic pelvic pain symptoms; pain in buttocks and down back of leg, dyspareunia
Treatment
: Biofeedback, Pelvic Floor Physical Therapy, TENS (Transcutaneous Electrical Nerve
Stimulation) units, antianxiolytic therapy, cooperation from sexual partner
6
Differential Diagnosis:
Urological Conditions that may Cause or Exacerbate Chronic Pelvic Pain
Chronic Urinary Tract Infection
Recurrent Acute Cystitis
Recurrent Acute Urethritis
Stone/urolithiasis
Urethral Caruncle
Bladder Carcinoma
Interstitial Cystitis
Radiation Cystitis
Urethral Syndrome
Detrussor Dyssynergia
Urethral Diverticulum
Interstitial Cystitis
Description
: Chronic inflammatory condition of the bladder
Etiology: Loss of mucosal surface protection of the bladder and thereby increased bladder
permeability
Symptoms
:
Urinary urgency and frequency
Pain is worse with bladder filling; improved with urination
Pain is worse with certain foods
Pressure in the bladder and/or pelvis
Pelvic Pain in up to 70% of women
Present in 38-85% presenting with chronic pelvic pain
Diagnosis
:
Cystoscopy with bladder distension
Presence of glomerulations (Hunner Ulcers)
Treatment
:
Avoidance of acidic foods and beverages
Antihistamines
Tricyclic antidepressants
Elmiron (pentosan polysulphate)
Intravesical therapy: DMSO (dimethyl sulfoxide)
Differential Diagnosis:
Gastrointestinal Conditions that may Cause or Exacerbate Chronic Pelvic Pain
Irritable Bowel Syndrome
Colon Cancer
Constipation
Inflammatory Bowel Disease
Colitis
Chronic
Intermittent
Bowel
Obstruction
Diverticular Disease
Irritable Bowel Syndrome (IBS)
Description
: Chronic relapsing pattern of abdominopelvic pain and bowel dysfunction with
diarrhea and constipation

7
Prevalence
Affects 12% of the U.S. population
2:1 prevalence in women: men
Peak age of 30-40’s
Rare on women over 50
Associated with elevated stress level
Symptoms
Diarrhea, constipation, bloating, mucousy stools
Symptoms of IBS found in 50-80% women with CPP
Diagnosis
based on Rome II criteria

8
Treatment
Dietary changes
Decrease stress
Cognitive Psychotherapy
Medications
Antidiarrheals
Antispasmodics
Tricyclic Antidepressants
Serotonin receptor (3, 4) antagonists
Psychological Associations
40 – 50% of women with CPP have a history of abuse (physical, verbal , sexual)
o Psychosomatic factors play a prominent role in CPP
o Psychotropic medications and various modes of psychotherapy appear to be helpful
as both primary and adjunct therapy for treatment of CPP
o Approach patient in a gentle, non-judgmental manner
Do not want to imply that “pain is all in her head”
Conclusions
Chronic Pelvic Pain requires patience, understanding and collaboration from both patient
and physician
Obtaining a thorough history is key to accurate diagnosis and effective treatment
Diagnosis is often multifactorial – may affect more than one pelvic organ
Treatment options often multifactorial – medical, surgical, physical therapy, cognitive
Mubark A. Wilkins