
1
Ascaris lumbricoides
Ascaris lumbricoides Linnaeus, 1758, the large intestinal roundworm of man, has
been known to physicians since the dawn of history. Davaine (1863) first
discovered that fully mature Ascaris eggs hatch in the small intestine and Stewart
(1916) showed that the hatched larvae require a migration to the lungs before final
development in the intestine.
With the possible exception of Enterobius, Ascaris lumbricoides is the most widely
prevalent of all human roundworms and occurs endemically in all parts of the
world except in cold, dry climates.
Morphology, Biology and Life Cycle.
Ascaris is the largest roundworm parasitizing the human intestinal tract.
The sexually mature male worm measures 12 to 31 cm in length by 2 to 4 mm in
greatest diameter. The female measures 20 to 35 cm. In length by 3 to 9 mm in
greatest diameter, but specimens up to 45 cm are occasionally observed. The daily
egg production per female averages about 200.000.
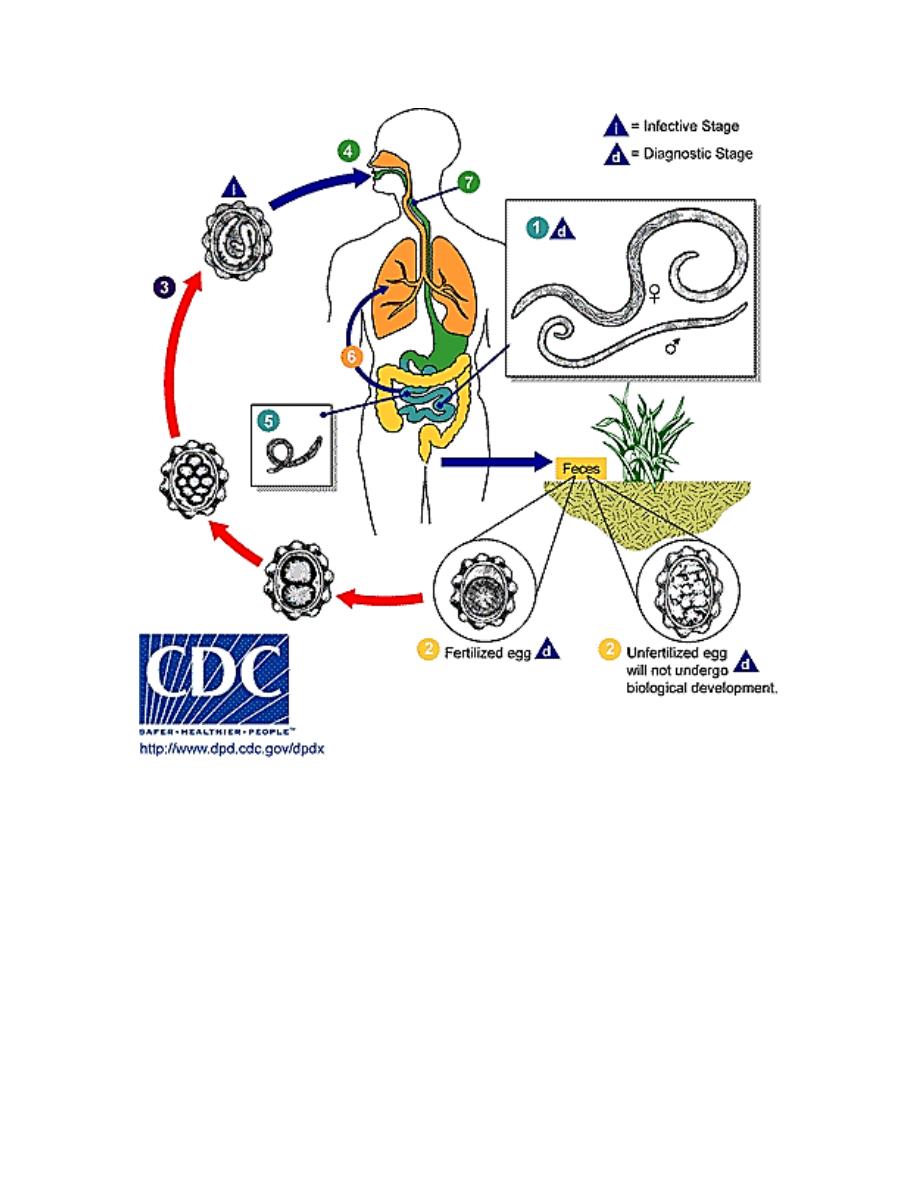
The fertilized egg of A. lumbricoides at the time of oviposition is broadly ovoidal,
measures 65 to 75 microns by 35 to 50 microns.
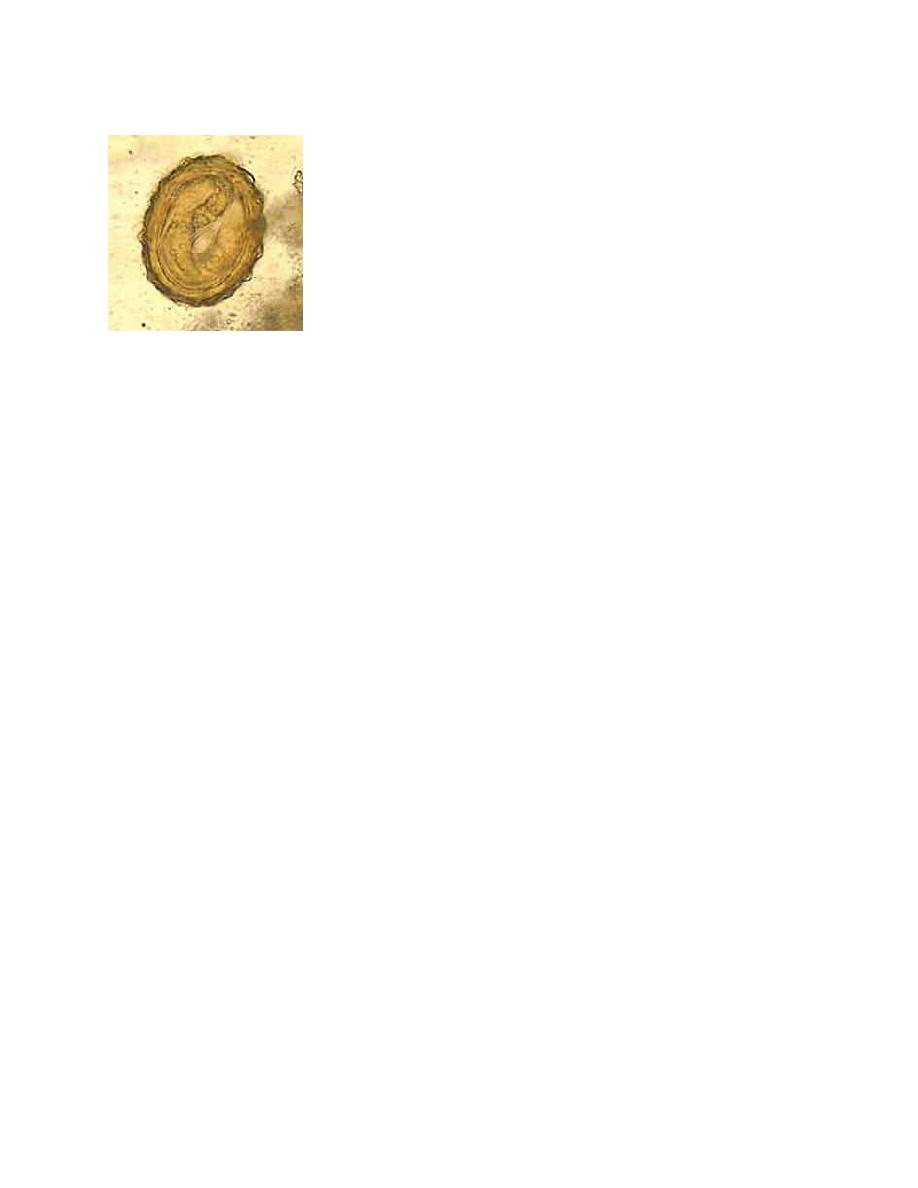
2
Fertilized egg
Female worms without males produce infertile eggs which typically are more
elliptical (88 to 93 microns by 38 to 44 microns) than fertilized eggs.
Both fertile and infertile eggs are usually bile-stained by the time they are
evacuated in the feces. Fertile eggs of A. lumbricoides are passed in the one-cell
stage. They survive putrefaction and can withstand considerable desiccation and
cold. The eggs are infective and contain motile second-stage larvae. Eggs may
remain viable in soil for months and even a year or longer.
When ingested, the infective larvae hatch in the duodenum and penetrate into the
nearby intestinal wall, enter mesenteric venules or lymphatics and via the liver and
inferior vena cava or thoracic duct reach the chambers of the right heart and pass
through the pulmonary vessels to capillaries, where they perforate into the alveoli.
On about the 9
th
day, after doubling their length and molting to the 3
rd
larval stage,
they begin migration via the trachea to the intestine, where they undergo two
further molts and become sexually mature worms 8 to 12 weeks after exposure.
The adult worms may live up to 16 months or possibly 20 months, but usually they
are passed spontaneously in about 12 months.
3
Pathogenesis and Symptomatology.
In light infections there may be no apparent pathologic changes, although even a
single ectopic worm may occasionally produce serious disease. In the average
infection in children there are intermittent colic, loss of appetite, fretfulness, and at
times nervous symptoms. The abdomen is characteristically protuberant. The
nutritional demands and space requirements of massive infections may be great.
Heavy Ascaris infection can lead to significant nutritional impairment.

4
Diagnosis
During the prepatent period, unless immature worms are passed, a specific
diagnosis is not possible.
Once in the intestine, the daily egg output of a single female is about 200000,
sufficient for one to several characteristic eggs to be revealed in an average direct
faecal smear.
Treatment
Ascariasis is treated with albendazole, mebendazole, or ivermectin. Dosage is the
same for children as for adults. Infections are generally treated for 1-3 days. The
drugs are effective and appear to have few side effects (CDC).