Lec 3
Tonsillectomy
This is one of the most commonly performed operations.
Patients usually stay in hospital for one night, so that bleeding
may be recognized and treated appropriately. Tonsils are
removed by dissection under general anaesthetic. Haemostasis
is achieved with diathermy or ties.
Tonsillectomy is very painful and regular simple analgesia is
always required afterwards. Patients should be advised that
referred pain to the ear is common. Until the tonsillar fossae are
completely healed, eating is very uncomfortable. The traditional
jelly and ice cream has now been replaced with crisps, biscuits,
and toast, since chewing and swallowing after tonsillectomy is
very important for recovery and in helping to prevent infection.
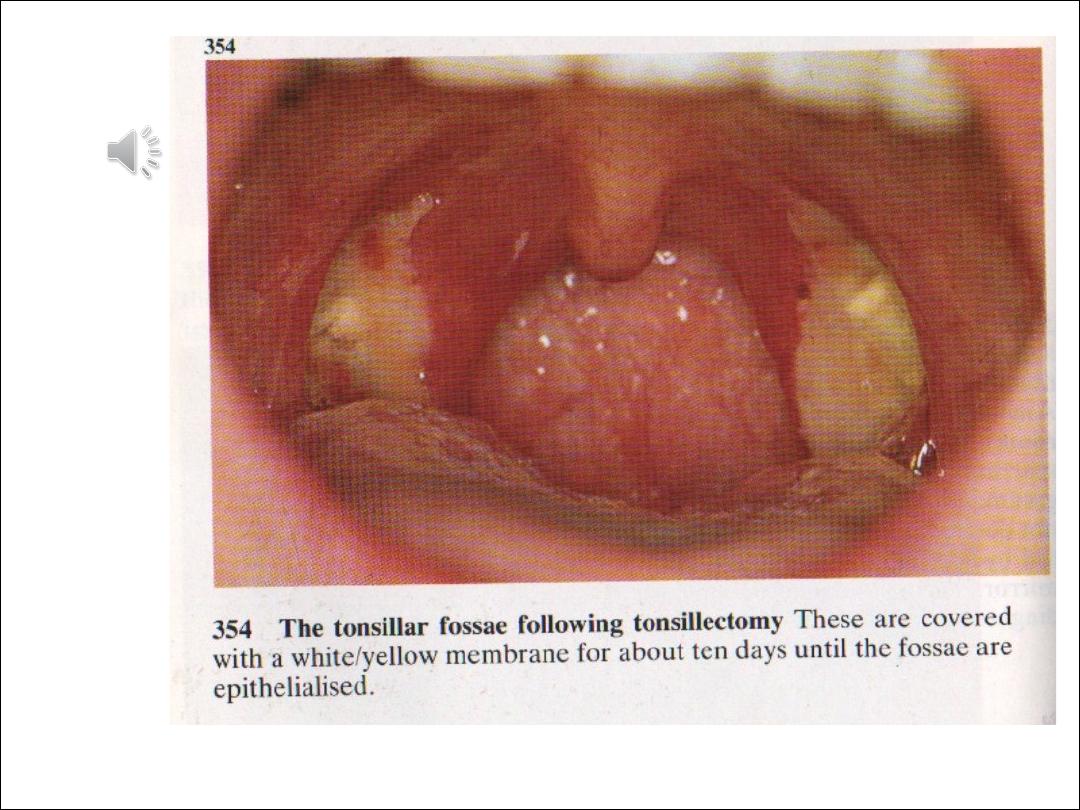
In the immediate postoperative period the tonsillar fossae
become coated with a white exudate, which can be mistaken as
a sign of infection.
Indications for tonsillectomy
1- Absolute indications for surgery
•
Suspected malignancy
•
Children with OSA (obstructive sleep apnoea)
•
As part of another procedure such as UPP for
snoring.(UPP=uvulopalatopharyngoplasty)
2-Relative indications for surgery
•
Recurrent acute tonsillitis
•
3 attacks per year for 3 years or
•
5 attacks in any one year
•
More than one quinsy.
Big tonsils which are asymptomatic need not be
removed.

Complications
1-Postoperative haemorrhage is a serious
complication for between 5-15% of
patients after a tonsillectomy.
A reactive haemorrhage can occur in the
first few hours after the operation, this will
frequently necessitate a return trip to the
operating theatre.
A secondary haemorrhage can occur any
time within two weeks of the operation.
2-trauma to teeth, palate, gum.TM joint
trauma or dislocation

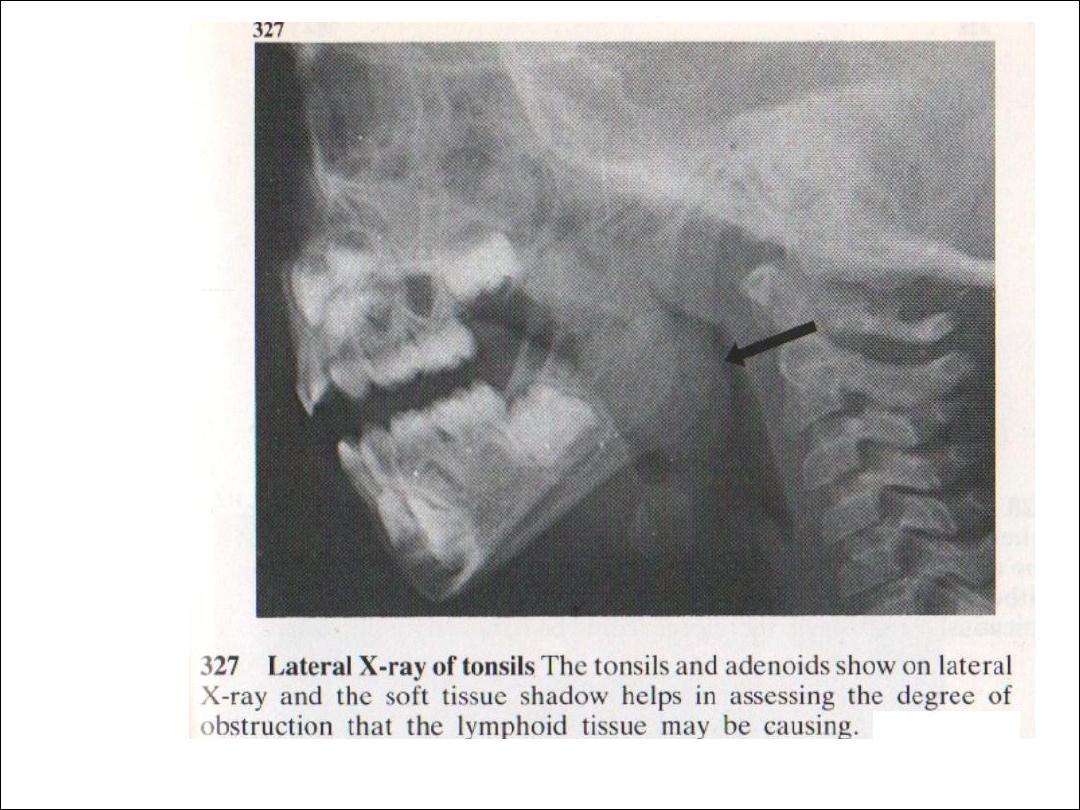
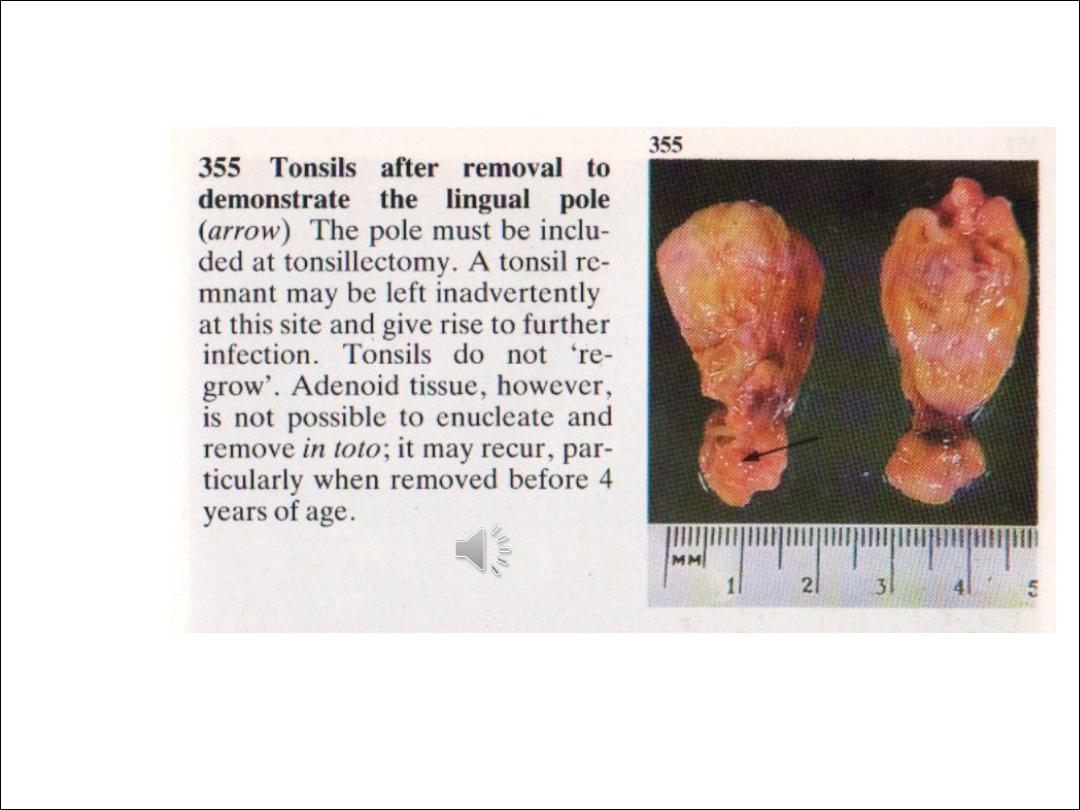
Adenoidal enlargement
The adenoid is a collection of loose lymphoid tissue
found in the space at the back of the nose. The
Eustachian tubes open immediately lateral to the
adenoids. Enlargement of the adenoids is very
common, especially in children. It may happen as a
result of repeated upper respiratory tract infections
which occur in children due to their poorly developed
immune systems.
Signs and symptoms
•
Nasal obstruction
•
Nasal quality to the voice
•
Mouth breathing which may interfere with eating
•
A Runny nose
•
Snoring
•
Obstructive sleep apnoea syndrome (OSAS)
•
Blockage of the eustachian tube.

A diagnosis of adenoidal enlargement is usually suspected from the history.
Using a mirror or an endoscopic nasal examination will confirm the diagnosis.
The glue ear which arises as a result of poor eustachian tube function may
cause hearing impairment. Adenoiditis or infection of the adenoid, may allow
ascending infections to reach the middle ear via the eustachian tube.
Treatment
An adenoidectomy is performed under a general anaesthetic. The adenoids
are usually removed using suction diathermy or curettage.
Complications
Haemorrhage (primary, reactionary, and secondary): These are serious
complications of an adenoidectomy, but this is less common than with a
tonsillectomy. The procedure is frequently carried out safely as a day case.
Nasal regurgitation: The soft palate acts as a flap valve and separates the
nasal and the oral cavity. If the adenoid is removed in patients who have even
a minor palatal abnormality, it can have major effects on speech and
swallowing. Palatal incompetence can occur in these patients resulting in
nasal regurgitation of liquids and nasal escape during speech. Assessment of
the palate should form part of the routine ENT examination before such an
operation, in order to avoid this complication.