
Lec 4:
-Tumours of the Nasopharynx :
Benign Tumors
Juvenile Angiofibroma
Epidemiology: Benign tumors of the nasopharynx are rare. The
most common of these is juvenile angiofibroma, which accounts
for less than 0.05% of all ear, nose, and throat (ENT) ``tumors
and occurs exclusively in boys 10–18 years of age
Symptoms: Typical symptoms are obstructed nasal breathing,
recurrent epistaxis, headache, impaired Eustachian tube
ventilation with middle ear effusion, and conductive hearing loss
due to obstruction of the eustachian tube orifice.
Diagnosis: The typical endoscopic appearance is that of a well-
circumscribed, vascularized mass with superficial vascular
markings, situated in the nasopharynx or posterior part of the
nasal cavity. If there is clinical suspicion of an angiofibroma, a
biopsy should not be performed due to the risk of heavy
bleeding. The primary workup should include MRI or CT, which
can accurately define tumor extension into surrounding
structures . Digital subtraction angiography (DSA) is useful for
identifying tumor-feeding vessels
Treatment: The treatment of choice is surgical removal of the
tumor. Preoperative embolization of the feeding vessels
(usually the maxillary artery) should be performed to reduce
the intensity of intraoperative bleeding
Malignant Tumors:
Epidemiology: Carcinomas of squamous-cell origin account for
the great majority of malignant nasopharyngeal tumors. A basic
distinction is drawn between
squamous cell carcinomas and lymphoepithelial carcinomas
(Schmincke tumor).
Much less common tumors of this region are adenocarcinoma,
adenoid cystic carcinoma, malignant melanoma, sarcoma,
lymphoma, and plasmacytoma.
Etiology: The Epstein–Barr virus (EBV) appears to have a key role
in the etiology of undifferentiated lymphoepithelial carcinoma.
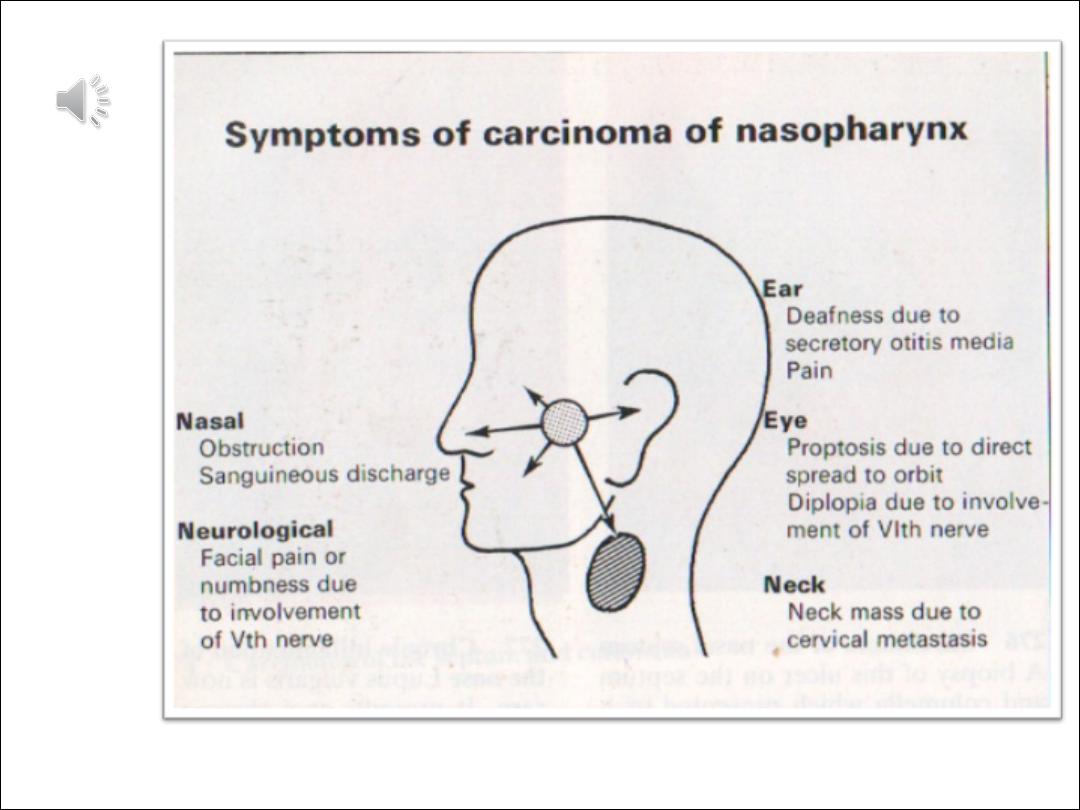
Symptoms: Early symptoms of nasopharyngeal malignancies are
unilateral conductive hearing loss with middle ear effusion. Any
persistent middle ear effusion of long duration in an adult
patient with no prior history of middle ear disease is suspicious
for a tumor and should be investigated accordingly. Cervical
lymph-node metastasis, usually involving the
nodes at the mandibular angle, is another common initial
finding. Features of advanced disease include nasal airway
obstruction, recurrent epistaxis, headaches, and cranial nerve
palsies.

Diagnosis: The primary study is endoscopy of the nasopharynx
.Nasopharyngeal malignancies can have a variety of appearances
ranging from a smooth, well-circumscribed tumor surface to mucosal
ulcerations.
Some of these tumors are initially submucosal and are easily missed at
endoscopy.
Otomicroscopy reveals unilateral tympanic membrane retraction and
a middle ear effusion as a result of impaired eustachian tube
ventilation. Given the EBV association of many nasopharyngeal
cancers, the
EBV antibody titer should be determined (this shows an elevated IgA,
contrasting with the elevated IgM/IgG that is found in infectious
mononucleosis). MRI or CT is useful for defining tumor extent
Treatment: The treatment of choice for most nasopharyngeal
carcinomas is primary high-voltage radiotherapy, because most of
these tumors are very radiosensitive and the unfavorable tumor
location and rapid invasion of the skull base preclude curative surgery
in
many cases.
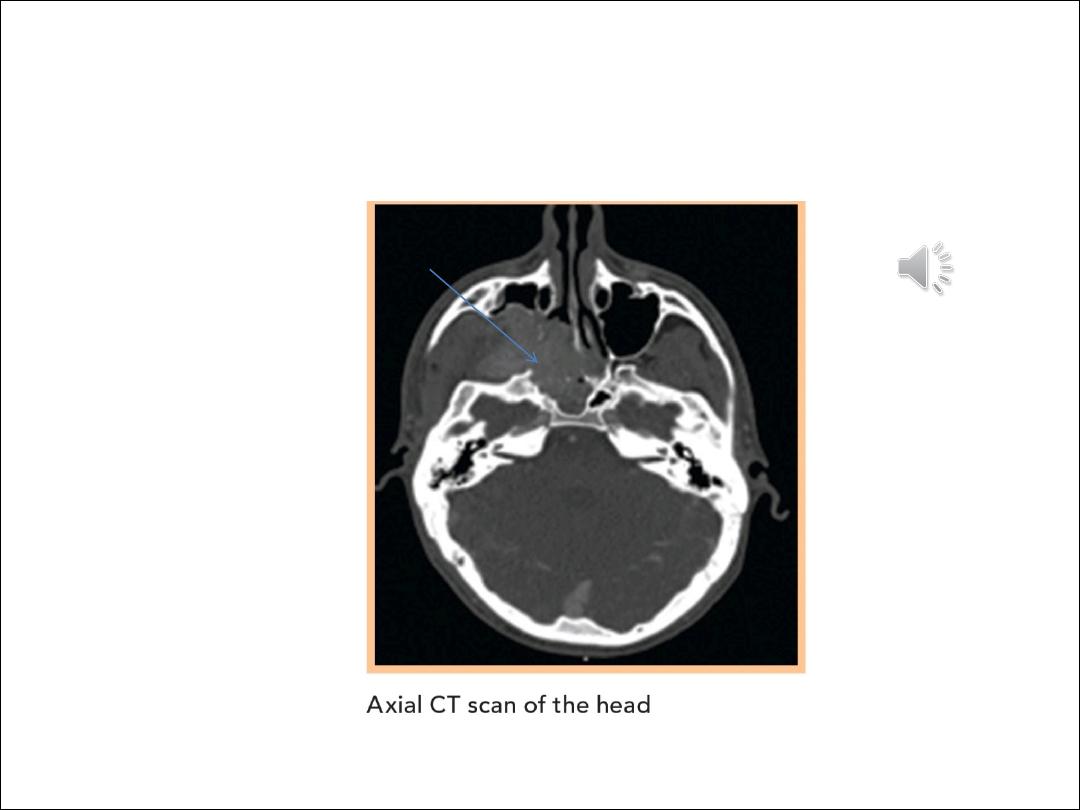
nasopharyngeal tumour CT SCAN
