
1
Dermatology Dr. Hussein A. Al-Sultany
2019-2020
Parasitic Skin Infections
A parasite is an organism that depends on a living host, for one or more of its essential
metabolic requirements.
Cutaneous Leishmaniasis (Baghdad Boil)
Cause:
Leishmaniasis is caused by Leishmania, which is a dimorphic parasite (present as
promastigote form in the gut of Phlebotomous sandfly, and in amastigote form in the
macrophage of human).
Life Cycle:
Phlebotomous sandfly female (vector) ingests amastigotes while taking a blood meal from
the skin of a human or other mammals (reservoir). Amastigotes transform into
promastigotes in the vector’s gut, then the sandfly inject it into skin of a human (host).
Promastigotes become amastigotes inside the host, and then taken by the macrophages
within which they multiply.
Clinical Types of Leishmaniasis:
1. Cutaneous Leishmaniasis (CL), including: old world CL and new world CL.
2. Mucocutanous Leishmaniasis.
3. Visceral Leishmaniasis (Kala-Azar).
Old World Cutaneous Leishmaniasis:
(Baghdad Boil, Delhi Boil, Little Sister).
It is caused by: L. major, L. tropica, L. aethiopica, or L. infantum.
Epidemiology:
Old world include the Mediterranean basin, Southern Europe, Africa, and Asia.
CL is an endemic disease in Iraq. Children are the commonest age group affected; since
immunity is acquired from the initial infection.
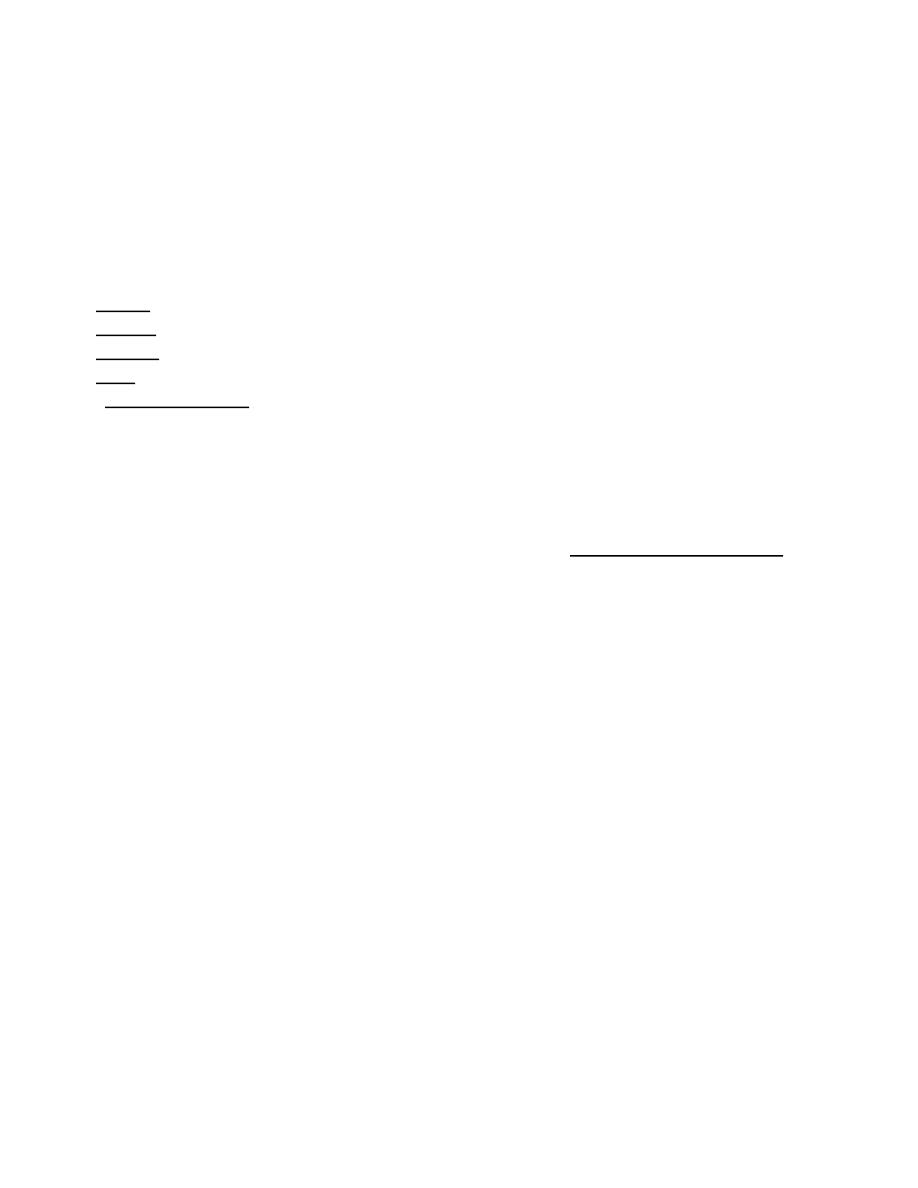
Clinical Features:
Incubation period: is variable (average: 2-3 months).
Onset: is insidious and usually at autumn or winter.
The predilection sites: are the exposed parts especially face, lower limbs, and hands.
The lesions: dusky red, indurated, painless and non-tender nodules, involving the exposed
parts, with slow evolution (more than one month duration).
●Two variants are described:
Wet (Ulcerative, Rural) type: caused by L. major. The IP less than 2 months. Healing
within 2-6 months (rapid course). Residual scar larger and deeper that of dry type.
Dry (Non ulcerative, Urban) type: caused by L. tropica. The IP is more than 2 month.
Healing within 8-12 months (longer course). Residual scar smaller and more superficial.
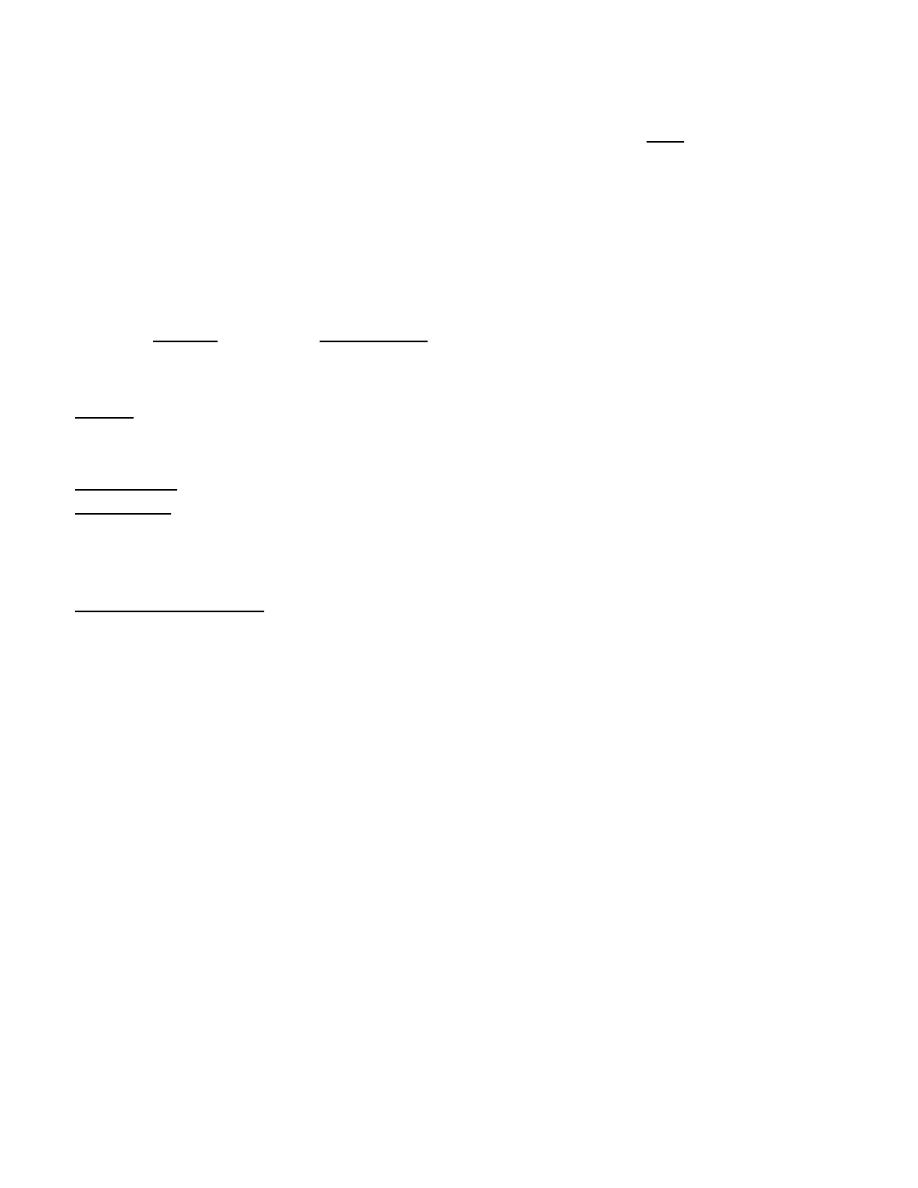
●Leishmaniasis Recidivans (Chronic Leishmaniasis):
Brown-red or brown-yellow papules, usually appear close to a scar of an old (mother)
2
●Post Kala-Azar Dermal Leishmaniasis (PKDL):
Begins during the convalescence of visceral
leishmaniasis, appearing on the face, forearms,
and lower limbs, as discrete papules.
●Recurrent Leishmaniasis:
Leishmaniasis usually gives lifelong immunity, but recurrent infection may occur in:
(1) Immunesuppressed. (2) Elderlies. (3) Very early treatment. (4) Infection by a new strain.
Diagnosis:
A- History: more than one month history of painless skin nodules.
B- Examination: dusky red, indurated nodules, on the exposed parts.
C- Investigation:
1. Smear: amastigotes in macrophage by Giemsa-stain (Leishman-Donovan, LD bodies).
2. Biopsy: demonstration of LD bodies, and granuloma.
3. Culture: growth of promastigotes in NNN medium.
4. PCR: demonstration of leishmanial DNA.
5. Leishmanin test (Montenegro test): Injection of 0.1 ml suspension of cultured
promastigotes in the forearm, and read after 48-72 h. It is unreliable in endemic areas.
Treatment:
CL is self-limited infection. The most important indications of treatment are: (1) Cosmetic
concern. (2) Controlling the disease in population. (3) Failure of spontaneous healing.
A- Intralesional infiltration:
1. Sodium stibogluconate solution (Pentostam)
®
: is the treatment of first choice in CL.
It is injected intradermaly in the borders of the lesions at 1-2 weeks intervals until cure.
2. Zinc sulfate solution (2%).
3. Hypertonic sodium chloride solution (7%).
4. Gamma Interferon: effective but expensive.
B- Topical therapy:
Topical paromycin, ketoconazole cream or podophyllin.
C- Physical therapy:
Infrared heat, cryotherapy, surgical excision or laser ablation (CO2 laser).
D- Systemic therapy:
I- Parentral:
1. Sodium stibogluconate (Pentostam)
®
: the 1
st
choice systemic agent in treatment of CL.
Dose: 20 mg/ kg / day for 28 days in two divided daily doses i.v. or i.m.. Although
uncommon, cardiotoxicity is the most serious side effect (it should be given under ECG
monitoring).
2. Meglumine antimoniate.
3. Amphotericin B: may be used in antimonial-resistant cases.
II- Oral:
Zinc sulphate, dapsone, ketaconazole, rifampicin, itraconazole, or allopurinol.
Indications of systemic therapy:
1. Multiple or large lesions.
2. Lesions in an immunocompromized patient.
3. Lesions in a critical area (around eyes), or in disfiguring or painful areas (nose & ears).
4. Leishmaniasis Recidivans.
3
Scabies
Cause:
Human scabies is a highly contagious infestation, caused by a mite (sarcoptes scabiei
var hominus).
Life Cycle:
Adult mites are 0.3 mm long. The mite infestation begins when a fertilized female mite
arrives to skin surface, then burrow through the stratum corneum at a rate of 3 mm per day,
it lays about 3 eggs per day, eggs hatch within 3 days into larvae, which reach maturity in
about 3 weeks. The mite can survive for about 3 days outside the human skin (Role of 3).
Transmission:
Through prolong (5-20 min) close contact, some infections from exposure to fomites.
Presentation:
Scabies affects all races and all social classes. Occurs at any age, with equal sex incidence.
The IP: weeks to months after the initial exposure to the mite. The IP is only few days in
subsequent exposure, due to prior sensitization (the eruption caused by sensitization to the
mites or their products).
The itching: is severe and more at night (nocturnal pruritus is characteristic).
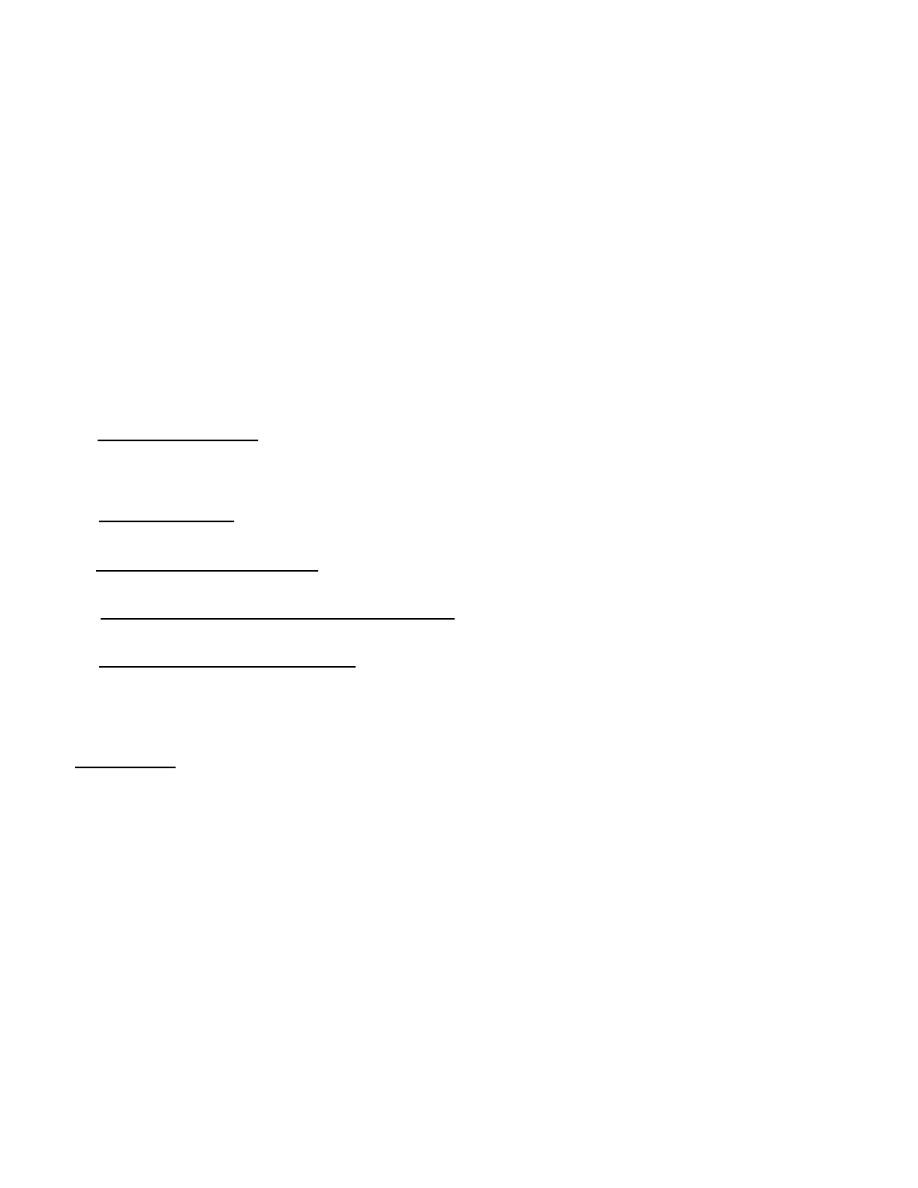
The lesions: the pathognomonic lesion is a burrow, which is a gray white, slightly elevated,
tortuous or zigzag like linear lesion that is 1 to 10 mm in length. Scratching may destroy the
burrows; therefore they don’t appear in some patients.
Other types of lesions are vesicles and papules (red, excoriated, and urticarial).
The predilection sites: interdigital webs, sides of fingers, sides of hand, wrists, elbow
flexure, axillae, areola, umbilicus and genitalia (Circle of Hebra; which is an imaginary
circle intersecting the predilection sites).
In infants, the face and scalp can be infested (very rare in adults), and there is a
characteristic palm and sole involvement.
The average number of adult female mites in an infected patient, is about 12.
Postscabitic allergic nodules: intensely itchy, red nodules that may persist for weeks
or months after successful treatment of scabies, treated by steroid.
Scabies incognito: is a modified scabies due to inappropriate use of topical steroids.
Crusted (Norwegian) scabies: is a widespread crusted eruption with minimum or
no itching with vast number of mites. It affects people with neurological disorders, senile
dementia, or immunosuppressed, and can be a source of epidemics of ordinary scabies.
Diagnosis:
A- History:
1. Presence of nocturnal pruritus.
2. Involvement of other members of the family.
3. History of prison, travelling or hospital admission for the patients or his close contacts.
B- Examination:
1. Involvement of the predilection sites.
2. Detection of burrows: for better visualization put a drop of mineral oil or use blue or
black ink then removed with alchohol swap.
3. Dermatoscopy: can be used to examine burrow and the mite in vivo.
4
C- Investigation:
1. Microscopical examination: of mites, eggs or its feces (scybala), usually within burrows.
The mite can be picked with a needle from the end of its burrow and identified
microscopically, eggs and mites can be seen in burrow scrapings mounted in KOH or
mineral oil.
2. Wood's light: also can be helpful (fluorescein solution fills the burrows and viewed).
3. Skin biopsy: can be diagnostic, the mite is found in the stratum corneum.
4. PCR: in which the DNA from the mite can be detected from cutaneous scales.
Treatment:
A- General principles:
1. Treat all members of the family and sexual contacts, whether they have itching or not.
2. Clothes and bed linens should be disinfected (with boiled water), and not used for 3 days.
3. The whole body should be covered with the medication, from below the jaw line, to the
soles. Face and scalp should be treated only in infants.
B- Topical medications:
1. Permethrine cream: (5 % for adults and 2.5 % for children), applied for 8-14 h;
repeated after 1 week. It is the treatment of choice, and can be used in pregnant and
lactating women and infants older than 2 months.
2. Sulfur ointment: (10 % for adults and 5% for children) once each day for three days.
Safe in pregnant, lactating, and infants. It is messy, have unpleasant odor, irritant and stain.
3. Crotamiton (Eurax) cream: is an antipruritic and scabicidal drug, once daily for 5 days.
Pregnancy category C (risk cannot be ruled out).
4. Gamma benzene hexachloride (Lindane): applied for 8 h and repeated after 1 week.
Not recommended in children, pregnancy, or lactation
5. Benzyl benzoate lotion 25 %: may be applied safely during pregnancy. The lotion is
usually applied once daily at night on 2 consecutive days, this may be followed by a single
application at night 3 days later.
C- Systemic medications:
Ivermectine: is an antihelminthic drug given in single oral dose (200 Mg / kg), and repeated
after one week. Indicated for: (1) Refractory cases. (2) Scabies in institutions. (3) Crusted
scabies.
5
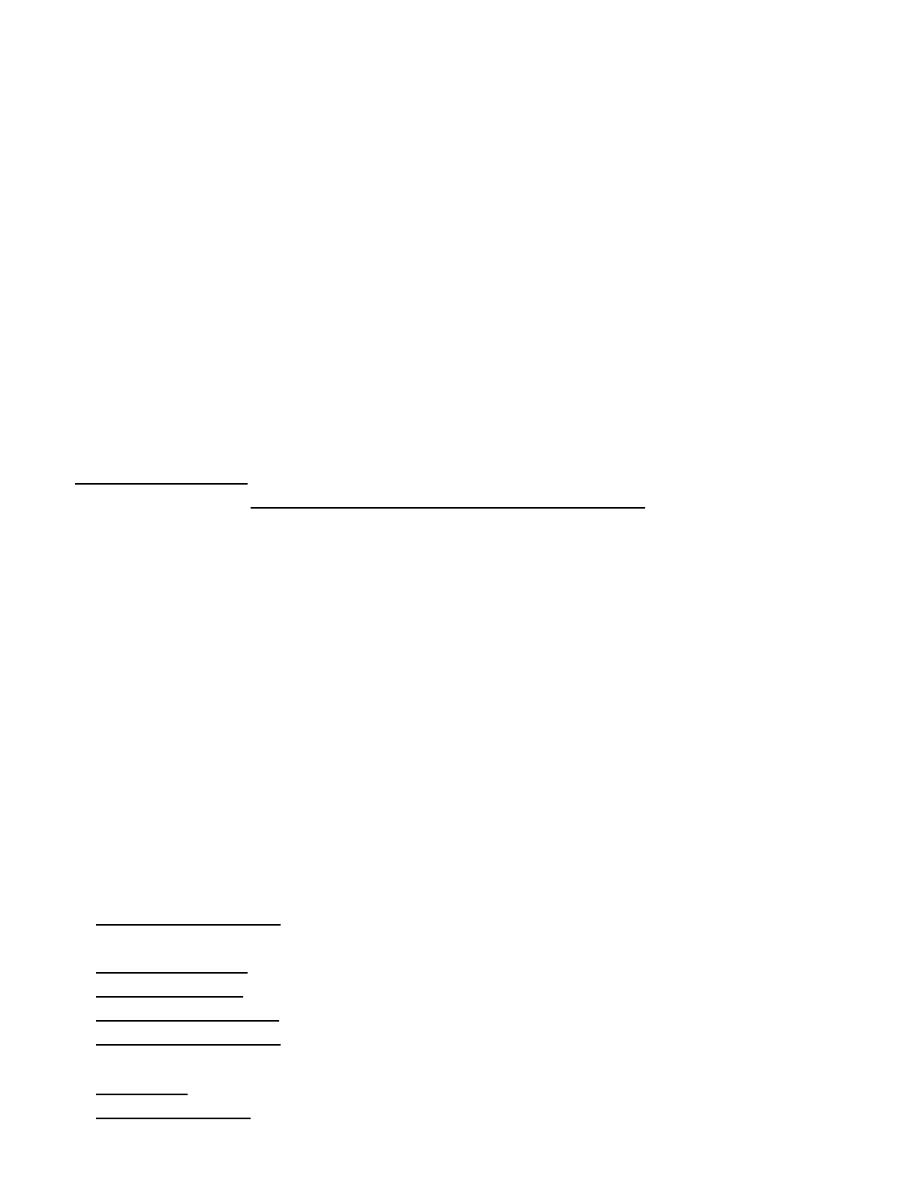
Lice Infestations (Pediculosis)
Cause:
Lice are flattened wingless insects. Two species are obligate parasites in humans: Pediculus
humanus (P.h. capitis, the head louse, and P.h. corporis, the body louse) and Phthirus pubis
(the pubic louse).
Pubic lice (crabs) are broader than scalp and body lice.
Life Cycle:
The female louse (3mm long) lays eggs at a rate of 8 eggs per day. The eggs hatch within 8
days into larvae. The larvae transform into adult lice in 8 days (Role of 8).
Transmission:
It is achieved by direct contact, and by contaminated fomites.
Clinical Types:
Head lice: it is most common in children, and more in girls. The main symptom is itching,
scratching and secondary infection may follow.
Body lice: body louse infestations are now uncommon except in the unhygienic and
socially deprived persons. There is a severe and widespread itching on the trunk.
Body lice can transmit typhus, relapsing fever, and trench fever.
Vagabond’s disease: it is a chronic untreated body lice infection.
Pubic lice: it is the most contagious sexually transmited infection. Most commonly infest
young adults. Severe itching with excoriations in the pubic area may followed by
secondary infection. A blue-grey macules of altered blood at the site of bites may be seen.
Eyelash infestation: Almost exclusively in children, may acquired from other children, or
from infected adult with pubic lice (may be a sign of sexual abuse).
Diagnosis:
A- History.
B- Examination: of the scalp may show few adult lice which are gray and hard to find,
but the nits are many and easily detected. Nits should be differentiated from simple scales
(the nits are oval, shiny, firmly attached to one side of the hair (45°) close to the skin).
C- Investigation: lice and nits seen more easily with wood's light or under microscope.
Treatment:
A-General measures:
1. Household members and those in close contact should be treated.
2. Fomite control is important to prevent reinfestation.
3. Medications should be repeated after 7-10 days (usually 8 days).
B- Topical medications:
1. Permethrin cream 1%: the most effective treatment. It paralyzes the nerves that allow the
lice to breathe. It is applied on the scalp for 10 minutes, after the hair is washed and dried.
2. Pyrethrin solution: applied for 10 minutes.
3. Malathion lotion: has residual activity, one treatment is sufficient for 8-12 hours.
4. Lindane shampoo 1%.
5. Petrolatum (Vaseline): the most practical & effective treatment for eyelashes infestation.
C- Systemic medications:
1. Ivermectin: cause paralysis and death of lice. Single dose of 200Mg/kg .
2. Methoprim tablets: twice daily for 3 days (killing the essential bacteria in gut of louse).