• Epidemiology of Rheumatic fever & Rheumatic heart disease
• *• 1
• Rheumatic fever
• Definition
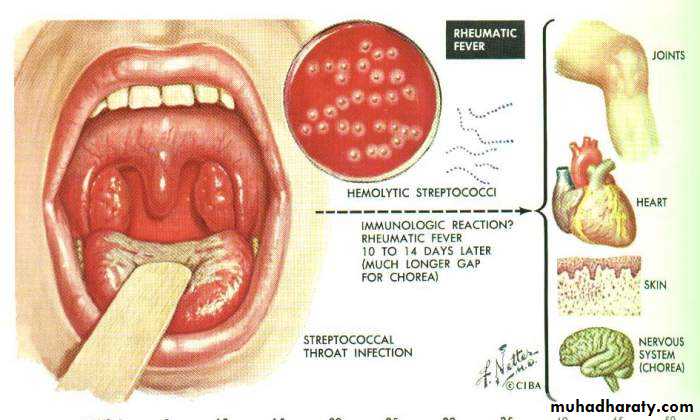
• Rheumatic fever is an immunologically mediated inflammatory disorder, which occurs as a sequel to group A streptococcal pharyngeal infection.• Multisystem disease affecting the heart, joints, brain, cutaneous and subcutaneous tissues
• Major public health problem in heavily populated underdeveloped and developing countries
• Preventable disease
• The most important consequence of rheumatic fever is chronic rheumatic heart disease, characterized by fibrotic valvular disease causing severe cardiac dysfunction decades later
• Only 3% pharyngitis patients develop RHD
• *
• 2
• Rheumatic fever
• Importance of RF
• It is a Human Leukocyte Antigen (HLA) associated disease, with antibodies, thus a classical autoimmune chronic disease, yet most people consider it an infectious disease.• Unlike practically any chronic diseases, it decreases with increasing socioeconomic status.
• It is one of the few autoimmune chronic diseases where both the genetic factors (HLA) and the environmental factors (group A Streptococci) are known.
• The immunologic events leading to the disease through superantigen are beginning to be worked out.
• Many years ago rheumatic fever/heart disease was the major killer of children worldwide. Now in developed countries most physicians will never see a case. If we can do this with rheumatic fever, we can also do it with many other HLA associated diseases.
• *
• 3
• Rheumatic fever
• *
• Rheumatic fever
• 4
• Epidemiology
• Ages 5-15 yrs are most susceptible
• Rare <3 yrs
• Girls>boys
• Common in 3rd world countries
• Environmental factors-- over crowding, poor sanitation, poverty,
• Incidence more during winter & early spring
• *
• Rheumatic fever• 5
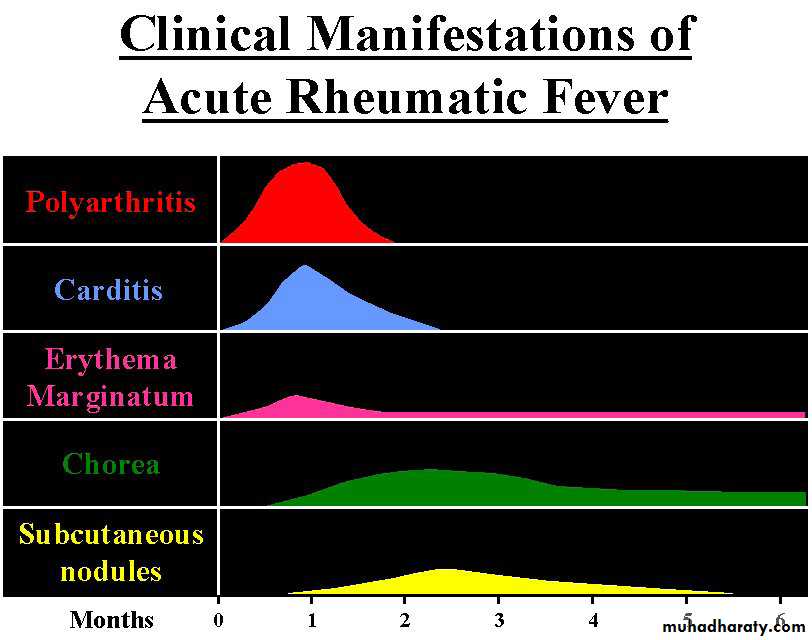
• Clinical Features
• Migratory polyarthritis, involving major joints
• Commonly involved joints-knee,ankle,elbow & wrist
• Occurs in 80%, involved joints are exquisitely tender
• In children below 5 yrs arthritis usually mild but carditis more prominent
• Arthritis do not progress to chronic disease
• 1.Arthritis
• Arthritis
• *
• Rheumatic fever
• 6

• *
• Rheumatic fever• 7
• Clinical Features (Contd)
• Manifest as pancarditis(endocarditis, myocarditis and pericarditis),occurs in 40-50% of cases
• Carditis is the only manifestation of rheumatic fever that leaves a sequelae & permanent damage to the organ
• Valvulitis occurs in acute phase
• Chronic phase- fibrosis, calcification & stenosis of heart valves.
• 2.Carditis
• Heart Disease
• *• Rheumatic fever
• 8
• *
• Rheumatic fever• 9
• Occurs in 5-10% of cases
• Mainly in girls of 1-15 yrs age
• May appear even 6 months after the attack of rheumatic fever
• Clinically manifest as- clumsiness, deterioration of hand-writing, emotional lability or grimacing of face
• 3.Sydenham Chorea
• Clinical Features (Contd)
• Sydenham Chorea
• *• Rheumatic fever
• 10

• *
• Rheumatic fever• 11
• Occur in <5%.
• Unique, transient lesions of 1-2 inches in size
• Pale center with red irregular margin
• More on trunks & limbs & non-itchy
• Worsens with application of heat
• Often associated with chronic carditis
• 4. Erythema Marginatum
• Clinical Features (Contd)
• Erythema Marginatum
•


• *
• 12• Rheumatic fever

• *
• Rheumatic fever• 13
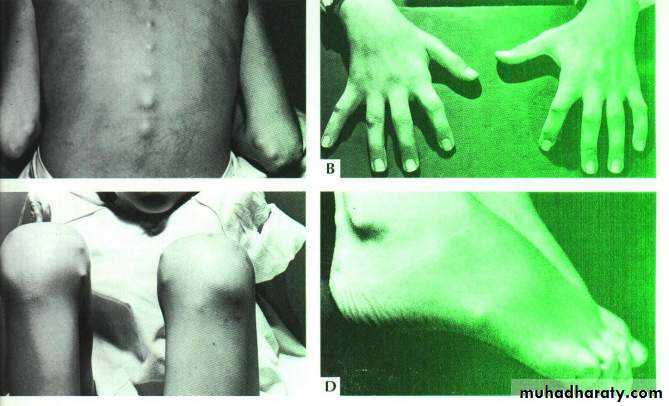
• Occur in 10%
• Painless, pea-sized, palpable nodules
• Mainly over extensor surfaces of joints, spine, & scalp
• Associated with strong seropositivity
• Always associated with severe carditis
• 5.Subcutaneous nodules
• Clinical Features (Contd)
• Subcutaneous nodules
• *
• 14• Rheumatic fever

• *
• Rheumatic fever• 15
• Other features (Minor features)
• Fever – Low grade
• Arthralgia
• Pallor
• Anorexia
• Loss of weight
• Clinical Features (Contd)
• *
• Rheumatic fever• 16
• Laboratory Findings
• High ESR
• Anemia, leucocytosis
• Elevated C-reactive protein
• ASO titer >200. (Peak value attained at 3 weeks, then comes down to normal by 6 weeks)
• Anti-DNAse B test
• Throat culture-GABH streptococci
• *
• Rheumatic fever
• 17
• Laboratory Findings (Contd)
• ECG- prolonged PR interval
• Echo - valve edema, mitral regurgitation, LA & LV dilatation, pericardial effusion, decreased contractility
• Rheumatic fever-diagnosisJones criteria for initial attack of rheumatic fever, For Diagnosis: Two Major or One major and two minor criteria following Group-A strep. pharyngitis. ( increased AS0 titer, positive throat culture GAS)
• Major criteria
• Carditis
• Polyarthritis
• Chorea
• Subcutaneous nodules
• Erythema marginatum
• Minor criteria
• Clinical findings-
• Arthralgia
• Fever
• Laboratory findings-
• Elevated acute phase reactants
• raised ESR
• raised CRP
• Prolonged P-R interval
• *
• 18
• Rheumatic fever
• *
• Rheumatic fever• 19
• The 2 primary features of autoimmunity are HLA and Antibodies. RF is characterized by both. RF has antibodies to the heart, and other tissues.
• *
• 20
• Rheumatic fever
• Superantigens may be what causes epidemiologic similarities across autoimmune diseases. These were first described in the early 1990s. Streptococcal A was the first bacteria identified as a superantigen. RF is a superantigen mediated disease.
• *
• 21
• Rheumatic fever
• Pathogenesis
• Group A streptococcal pharyngeal infection
• Body produce antibodies against streptococci.
• These antibodies cross react with human tissues because of the antigenic similarity between streptococcal components and human connective tissues (molecular mimicry).
• Immunologically mediated damage (autoimmune) to human tissues which have antigenic similarity with streptococcal components- like heart, joint, brain connective tissues
• Fibrinoid degeneration, inflammation mediated by T lymphocytes, macrophages.
• *
• 22
• Rheumatic fever
• Rheumatic fever-pathogenesis
• *
• 23• Rheumatic fever
• Rheumatic fever-epidemiology
• Parallels with epidemiology of streptococcal pharyngitis• Incidence –
• 3% in epidemics of exudative streptococcal pharyngitis in closed community
• 0.3% in civilian population with sporadic streptococcal throat infection
• 50% if there is a past history of rheumatic fever
• first attack between 5-15 years
• M:F equal, except Sydenham’s chorea which is more common in girls
• poor socioeconomic conditions and overcrowding
• *
• 24
• Rheumatic fever
• *
• Rheumatic fever
• 25

• Rheumatic fever-Epidemiology
• For rheumatic fever to occur-• Pharyngeal infection with group A streptocooci
• Certain rheumatogenic strains of GAS with M proteins
• Throat infection of sufficient duration- persistence of GAS
• Throat infection may or may not be symptomatic
• Throat infection is a must, not with pyoderma
• Infection of sufficient duration to produce antibody
• Brisk and sufficient antibody response to the infection
• Genetic predisposition
• *
• 26
• Rheumatic fever
• Much of our understanding of the etiology of RF has come from the brilliant work in the military. “ Previously, was said that one would catch the death of cold if he went out in cold, wet, nights with many people around”. It is here that the agent of RF is transmitted.
• *
• 27
• Rheumatic fever
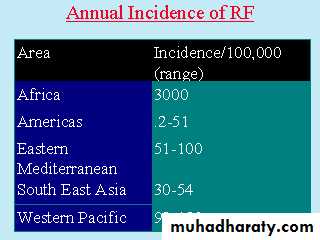
• There is an enormous variation of rheumatic fever around the world. The geographic variation is the greatest seen for almost any chronic disease.
• *
• 28
• Rheumatic fever

• *
• 29• Rheumatic fever
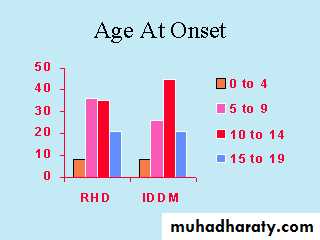
• The pattern of onset starts with few cases in the very earlier years, with a rapid increase in incidence in the pre pubertal and pubertal years, followed by a decline.
• *
• 30
• Rheumatic fever
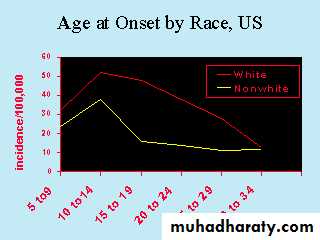
• Non-whites have tended to have a lower incidence in the US. However, this is unlikely to be genetic as when socioeconomic status was adjusted, the differences were eliminated.
• *
• 31
• Rheumatic fever
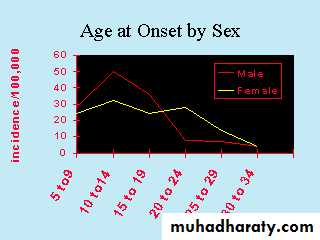
• Males tended to have a greater peak age of onset than females in the US. This could be related to a lower probability of group activities for females. However there are also sex hormone relationships to the disease as well as the autoimmune disease.
• *
• 32
• Rheumatic fever
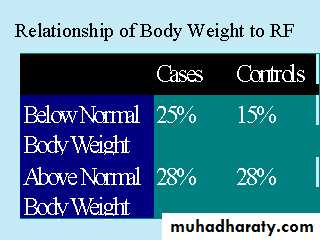
• Underweight children are particularly afflicted by RF. This could be due to them being poorer, thus having a greater risk of exposure, or due to the effect of nutrition or immune status.
• *
• 33
• Rheumatic fever
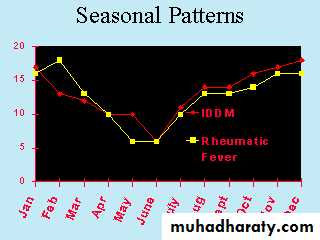
• RF shows a decrease in incidence in the warm summer months. This is consistent with the geographic variation which demonstrates higher incidence in the cooler climates.
• *
• 34
• Rheumatic fever
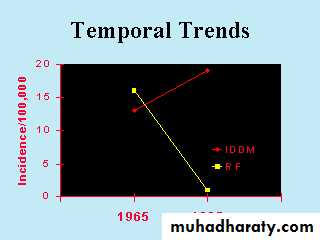
• There is an extremely successfulness in preventing RF with over a 98% reduction in about 25 years. This was not done through screening for antibodies, and immunoprevention. It was accomplished in part by epidemiology and public health.
• *
• 35
• Rheumatic fever
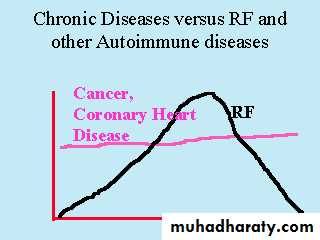
• RF and other autoimmune diseases do not act like typical chronic diseases. They have epidemics and they are frequent. It is in the epidemics that the etiology of autoimmune diseases will be found.
• *
• 36
• Rheumatic fever
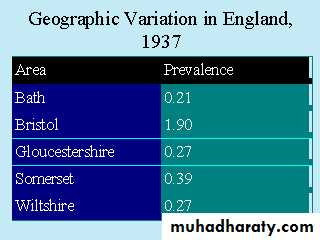
• RF is characterized by enormous geographic and SES differences, within countries as well. There can be a 30 fold variation across SES, and 20 fold across geographic area within the same country.
• *
• 37
• Rheumatic fever
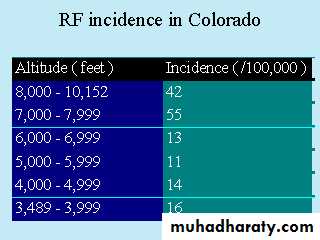
• With increasing altitude in feet, there is an increase in the incidence of rheumatic fever. It is of interest that several other autoimmune diseases exhibit a relationship to altitude.
• *
• 38
• Rheumatic fever
• *
• Rheumatic fever
• 39
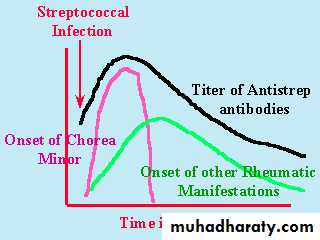
• The relationship between streptococcal A infection, and RF manifestations. The problem is that the infection occurs sometimes months before symptoms, and it is difficult to link the infection to Rheumatic Fever. This may be similar to that of other autoimmune diseases.
• *
• 40
• Rheumatic fever
• Treatment
• Bed rest 2-6 weeks• Supportive therapy- treatment of heart failure
• Anti-streptococcal therapy- Benzathine penicillin 1.2 million units or oral penicillin 10 days, if allergic erythromycin 10 days
• Anti-inflammatory agents-
• Aspirin 100 mg/kg per day for arthritis and in the absence of carditis- for 4-6 weeks to be tapered off
• Corticosteroids in presence of carditis – 1-2 mg/kg per day – for 4-6 weeks to be tapered off
• *
• 41
• Rheumatic fever
• Rheumatic fever- prevention
• Secondary prevention – prevention of recurrent attacks
• Benzathine penicillin G 1.2 million units IM every 4 weeks
• Or Penicillin V 250 mg twice daily orally
• Or Sulfadiazine 1 g daily orally
• If allergic to both – Erythromycin 250 mg twice daily orally
• Duration of secondary rheumatic fever prophylaxis
• Rheumatic fever + carditis + persistent valve disease-
• 10 years since last episode or until 40 years of age,
• sometimes life long
• Rheumatic fever + carditis + no valve disease –
• 10 years or well into adulthood whichever is longer
• Rheumatic fever without carditis-
• 5 years or until 21 years whichever is longer
• *
• 42
• Rheumatic fever
• Rheumatic fever-prognosis
• Prognosis is good if recurrence is prevented by continuous antibiotic prophylaxis- particularly if no carditis in the initial attack• If carditis, half of them can develop chronic rheumatic heart disease. Recurrence following streptococcal sore throat is high in patience with previous carditis
• Takes 10-20 years in western world but earlier in underdeveloped world due to malignant nature of the disease
• Mitral valve is most commonly affected, followed by aortic and tricuspid valves
• So these patients need long term follow up
• *
• 43
• Rheumatic fever
• Rheumatic heart disease
• Definition: A condition resulting from having Rheumatic fever as a child. ( weakening of the heart valve)
• Signs and Symptoms: Damaged heart valve which can progress into serious even a disabling condition.
• Causes: A disease process that begins with the untreated strep. throat infection.
• Treatment: Prevention is the best measure to be taken. Treat strep. throat infections with antibiotics so it does not progress into Rheumatic Fever.
• *
• 44
• Rheumatic fever
• Acute Rheumatic vegetations:

• *
• 45• Rheumatic fever
• Fish mouth Mitral stenosis:

• *
• 46• Rheumatic fever
• *
• Rheumatic fever
• 47

