1
Community Medicine / Fourth Stage / Dr. Ali / Lecture 18
Epidemiology of Diabetes Mellitus
Definition
• Diabetes mellitus is a metabolic disorder of multiple etiology characterized by
chronic hyperglycemia with disturbances of carbohydrates, fat and protein
metabolism resulting from a defect in insulin secretion, insulin action or both.
Why diabetes is important?
• Diabetes is a common disease.
• There is evidence that the overall worldwide prevalence of diabetes is gradually
increasing.
• Diabetes causes great morbidity and early mortality in a large number of people,
since it is associated with many complications.
• The cost of managing the complications of DM is high.
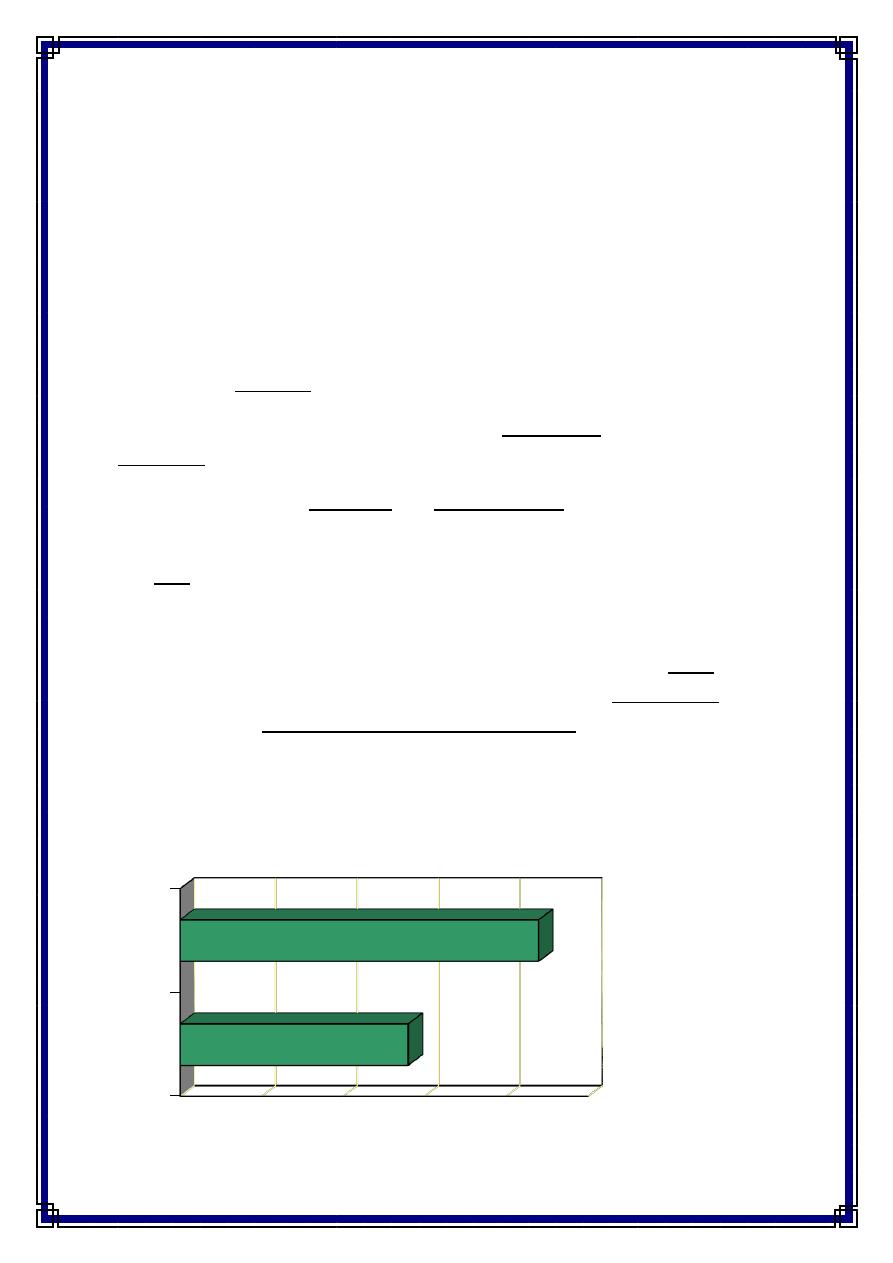
Burden of DM
• Diabetes prevalence is increasing in the developed world due to aging of the
population, and in the developing world due to increased urbanization
accompanied by cultural and socio-economic changes. Experts estimated that the
number of adults with diabetes will reach 300 million in the year 2025, more than
75% of them (i.e. 228 million) will be in the developing countries.
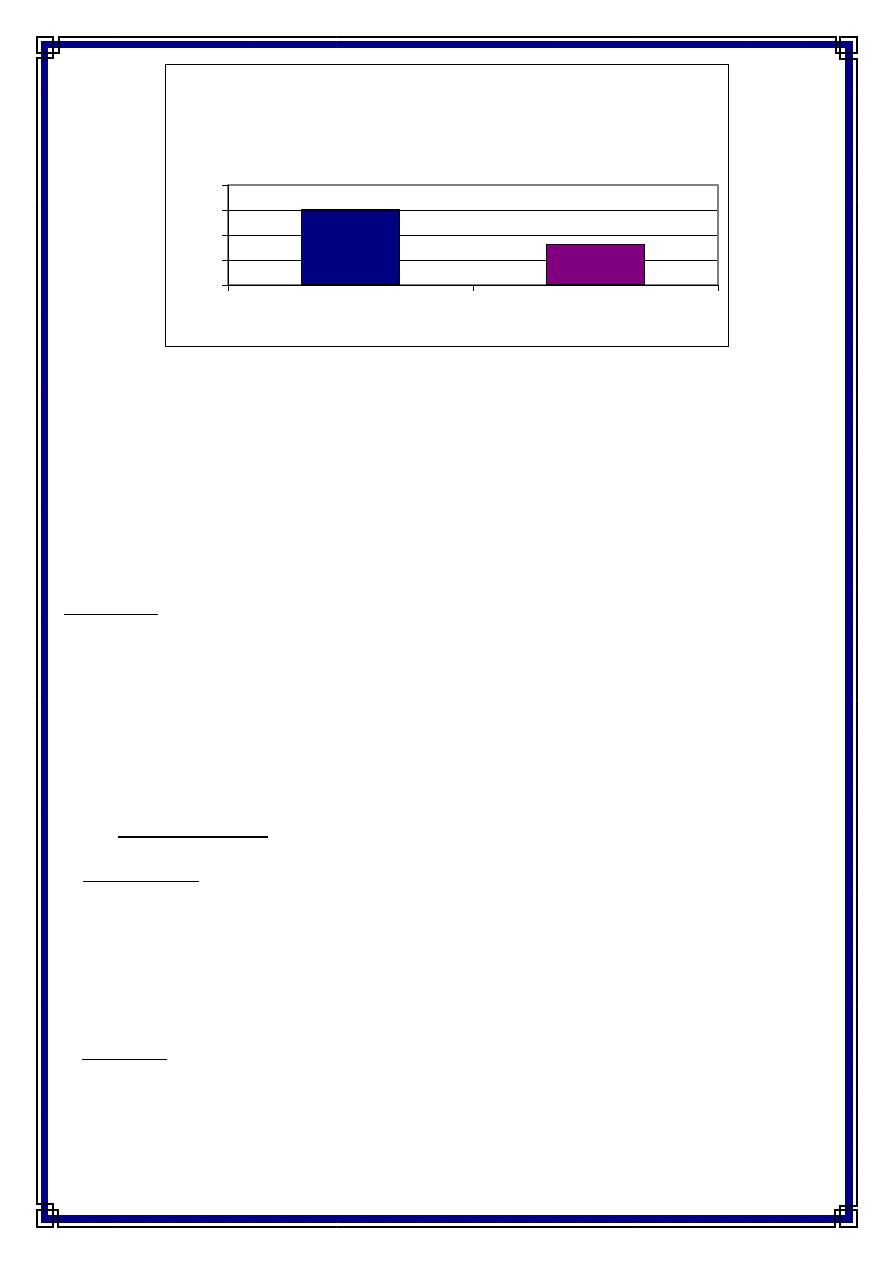
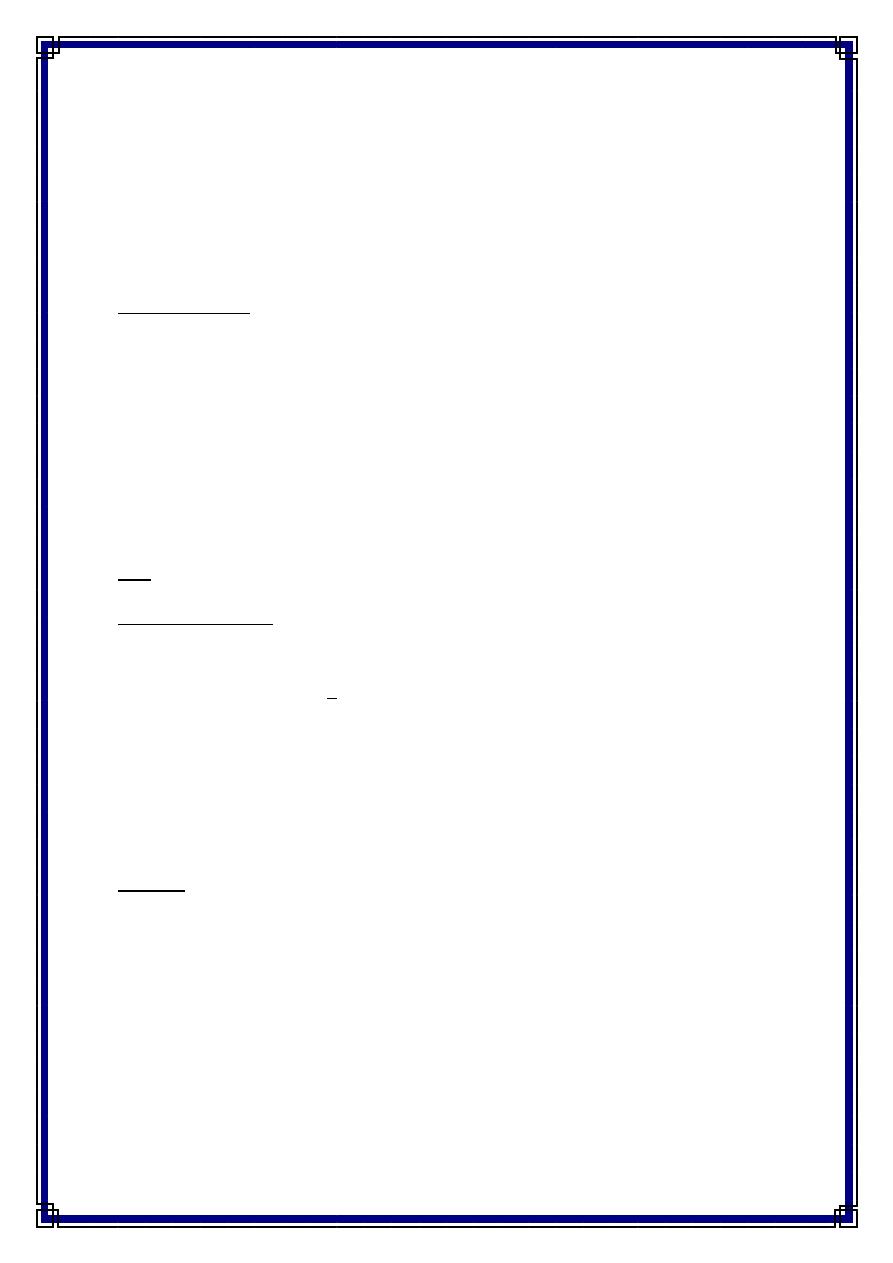
Global Prevalence Estimates, 2000 and 2030
0.0% 1.0% 2.0% 3.0% 4.0% 5.0%
2000
2030
2
Economic Burden
It is estimated that the cost of caring for people with diabetes is 2-4 times the cost of
caring for non-diabetic people in most health care systems. In 1992 a study in the US
concluded that more than US $ 100 billion was spent on overall health care of people
with diabetes.
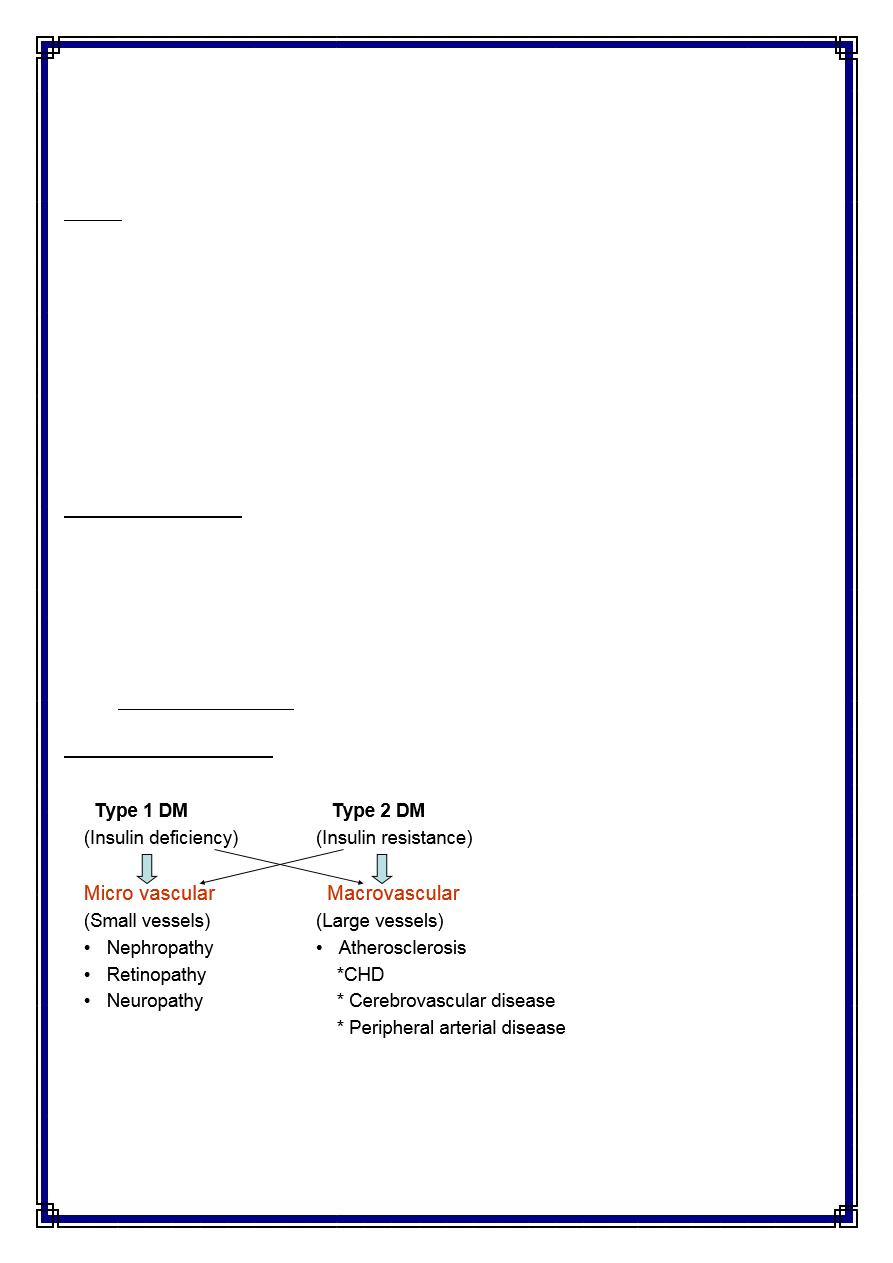
Types of DM
Type 1 DM
-
Accounts for 10% of all patients
-
Destruction of B-cells
-
Absolute insulin deficiency
-
Mostly at ages <30 years (it can occur at any age)
• Forms of Type 1 :
A- Autoimmune:
- Presence of autoimmune markers ( ICAs, IAAs, Autoantibodies to GAD65)
- Strong HLA association
- There is a genetic element
B-Idiopathic: (no known cause)
-
Only minority of patients fall in this group
-
Occurs in individuals of African& Asian origin
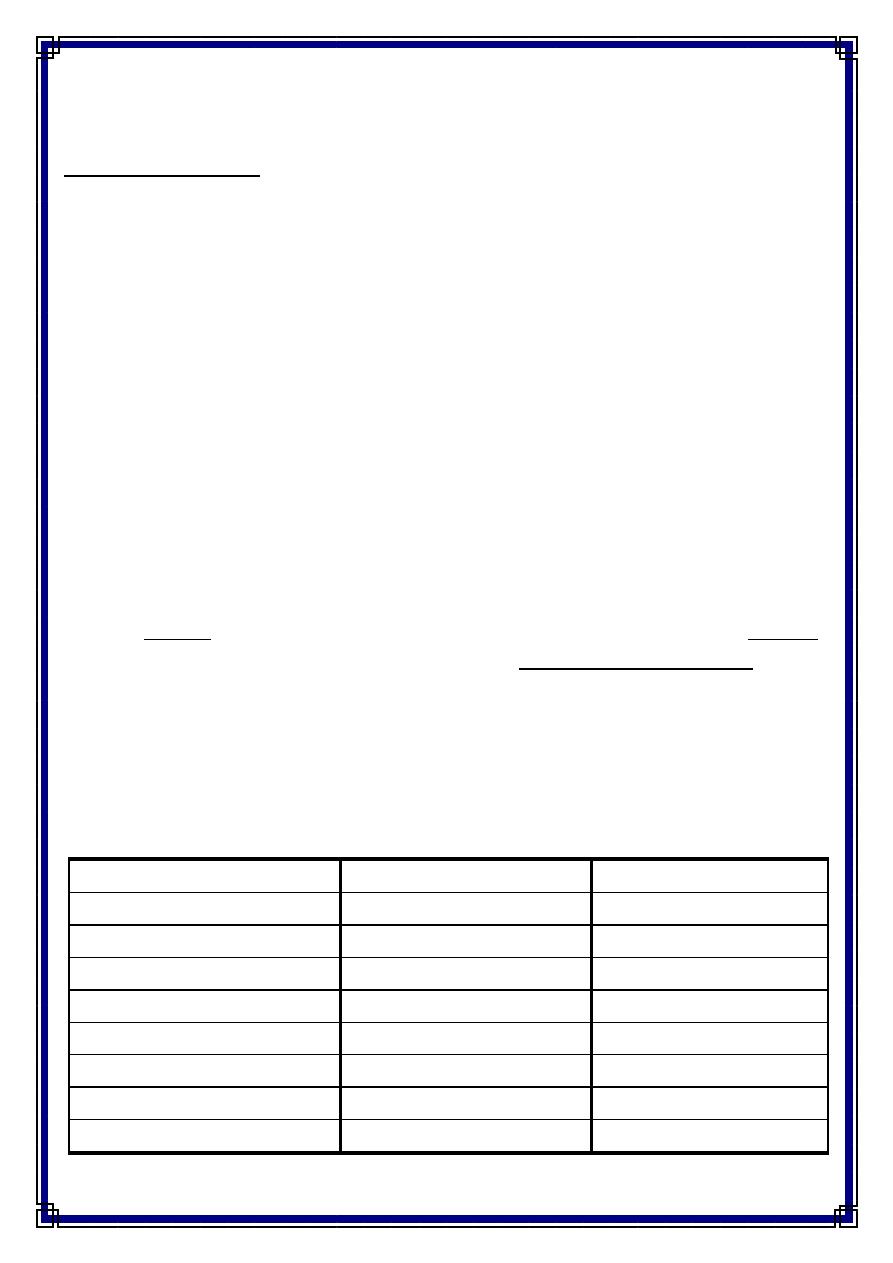
0
50
100
150
200
Developing countries
Developed countries
Number of persons with diabetes in 2007
(millions)
3
-
Strongly inherited
-
Lacks autoimmune markers
-
No HLA associated
Type 2
-
Most common (90%)
-
After age of 40 years
-
Predominant insulin resistance with relative insulin deficiency, ultimately loss of B-
cells mass can lead to insulin dependency
-
Onset is insidious
-
Due to genetic factors, environmental factors or both.
Other specific types:
-
Genetic defects of Beta-cells: onset at early age (<25 years). Inherited as an
autosomal dominant pattern. Previously known as maturity onset diabetes of
young (MODY).
-
Diabetes secondary to diseases of the pancreas or endocrinal diseases & drugs.
• Gestational diabetes
Complications of DM
Cardiovascular disease (i.e. macrovascular complications) is the cause of death in 75-80%
of patients with type 2 DM)
4
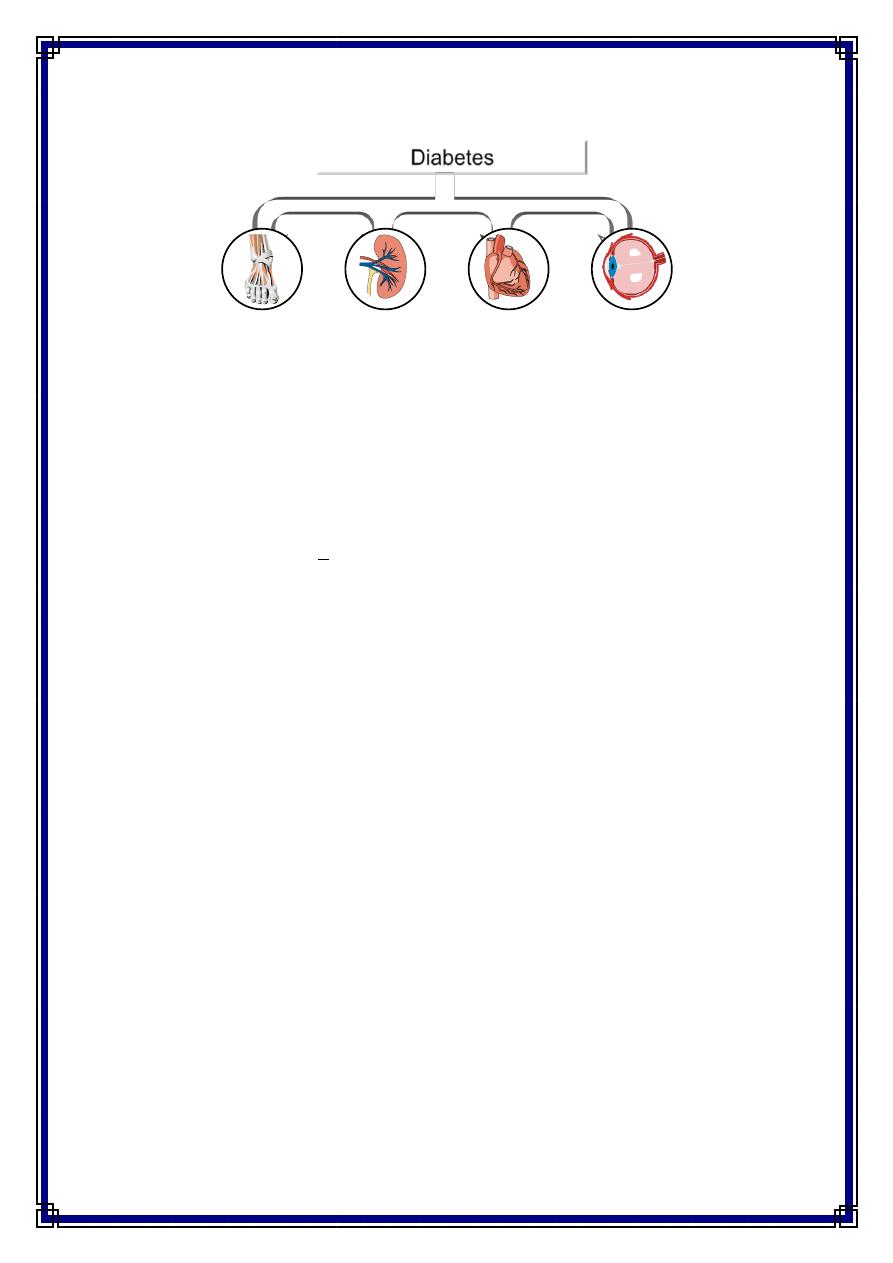
Impact of Diabetes Mellitus
Diabetes
The leading
cause of
new cases
of end
stage renal
disease
A 2- to 4-
fold
increase in
cardio-
vascular
mortality
The leading
cause of
new cases
of blindness
in working-
aged adults
The leading
cause of non-
traumatic lower
extremity
amputations
Diagnosis of DM
• Fasting plasma glucose >126mg/dl (7mmol/l)
• 2 hours postprandial plasma glucose >200mg/dl
• Any random plasma glucose >200mg/dl (11.1 mmol/l), together with polyuria,
polydypsia, weight loss, and visual blurring
• Must confirm diagnosis with two abnormal plasma glucose results on separate
days
• Glycosylated hemoglobin (HbA
1
c)
- reflection of how well the glucose has been controlled.
- hyperglycemia causes an increase in
HbA
1
c
- values expressed in percentages,
* with non-diabetic 5.5 to 7%,
* diabetic with good control 7.5 to 11.4%
* diabetic with moderate control 11.5 to 15%
*diabetic with poor control greater than
15%
5
Diagnosis of Impaired Glucose Tolerance
• Impaired glucose tolerance was defined by the Expert Committee as:
– Fasting Plasma glucose of 110-125mg/dl
– 2-hour post glucose load 140-199mg/dl
Risk factors
• Genetic factors
- Twin studies indicate a very strong genetic component to the etiology of type 1
DM. It is more common in those with certain HLA types.
- Twin studies also demonstrate a greater than 30% concordance among
monozygotic twins pairs in the expression of type 2 DM.
- Certain racial groups , as African Americans, Hispanics, and Native Americans, are
at increased risk for type 2 diabetes.
• Age: Incidence of type 2 DM increases with increasing age.
• Physical inactivity: Lack of exercise may alter the interaction between insulin and
its receptors and subsequently leads type 2 DM.
– Vigorous exercise > 1/week, 25% risk reduction (Manson & al, Lancet 1991,
338; 774-8., JAMA, 1992, 268,63-7)
– Looking TV 2-10 hours per week: RR 1.66 of having DM compared with 0-1
hour per week
( HU et al; Arch Intern Med 2001;161: 1542-1548)
• Obesity: Incidence of type 2 DM increases with increasing body mass index.
Obesity can induce resistance to the action of insulin.
– RR risk of DM in females (ref. BMI < 22)
• 22-23 3.0
• 24-25 5.0
• > 31
40
(Colditz & al, Ann Int Med, 1995, 122; 481-6)
6
• Drugs & hormones: Long list of drugs that affect carbohydrate metabolism had
been identified. e.g. Phenytoin, diuretics (thiazide type), corticosteroids. Oral
contraceptives, and beta-adrenergic blocking agents.
• Pancreatic disorders: Inflammatory, neoplastic, and other disorders of the
pancreas e.g. cystic fibrosis, and pancreatectomy.
• History of gestational diabetes or delivery of large babies.
Diabetes Mellitus Treatment
NO CURE!
Relieve symptoms.
Maintain quality of life.
Prevent further complications.
Preventive measures
• Primary prevention: Primary prevention of type 2 DM can be achieved by:
- Promotion of healthy nutrition: Encourage low saturated fat, high fiber diet.
- Smoking cessation
- Correction of obesity: Encourage weight loss to keep BMI<30
There are two approaches for primary prevention:
• The high risk approach:
This is directed to high risk people such as those with family history of type 2 DM,
obese individuals, and those with previous abnormalities of glucose tolerance including
gestational diabetes.
• The population approach:
This is based on altering the environmental risk factors and determinants of type 2 DM
in the whole population through public education
Secondary prevention
This level of prevention aims at early detection of asymptomatic cases
• Early detection and treatment
7
• Screening for gestational diabetes
• Screening for susceptible groups
Screening for diabetes:
-
Screening all adults over 40 years of age with fasting plasma glucose every 2-3
years.
-
Begin screening at earlier age with a positive family history, obesity, or symptoms
of DM.
The community should be involved in diabetes awareness and screening
Tertiary prevention
• This involves treatment of already established cases of diabetes
• What are the objectives of treatment of diabetes?
-
To relieve symptoms
-
To reduce mortality and economic costs of diabetes
-
To prevent as much as possible acute and long term complications and to monitor
the development of such complications and to provide timely intervention
-
To improve the quality of life and productivity of the individual with diabetes
Goals of diabetes management
Goals for chronic diabetes may be somewhat different for good control, not ideal goals
which are normal for a non-diabetic
Acceptable
Ideal (normal)
intervention
<140 mg/dl
<125 mg/dl
FPG
< 7
< 6
HbA1C
< 140/90
< 130/80
Blood pressure
< 240 mg/dl
< 200mg/dl
S. Cholesterol
< 130 mg/dl
< 100 mg/dl
LDL cholesterol
No smoking
No smoking
Stop smoking
BMI <30
BMI <25
Decrease weight
Daily 30 min.
Daily 30-60 min.
Daily exercise
8
Patient and family counseling
Patients and their families should be aware of the following:
• The disease is permanent, life-long treatment is required
• Control of blood sugar to delay appearance of microvascular complications
• Importance of foot care
-
Wash & dry feet daily
-
Soften & gently reduce calluses
-
File (but not cut) nails
-
Wear shoes that are soft and well fitting
-
Never walk barefoot
-
Notice & deal with small injuries or signs of pressure
• Management of hypoglycemic attacks
• Injection technique (when insulin used) and rotation of sites
• Counseling in family planning if possible
• Lifestyle modification:
-
smoking cessation
-
Diet control
-
Weight loss
-
Increase Physical activity
-
Social and psychological factors
,,Thank You,,