Abnormal Uterine
Bleeding

normal
abnormal
Duration
4-6 days
<2d, >7d
Volume
30-35cc
>80cc
Cycle length
21-35d
<21d, >35
Average Iron loss: 16mg
Menstrual Period Characteristics

•Menorrhagia
:
Heavy or prolonged uterine bleeding
that occurs
at regular intervals. Some sources define further as the loss of ≥ 80
mL blood per cycle or bleeding > 7 days.
•Hypomenorrhea
:
Periods
with
unusually
light
flow,
often
associated
with
hypogonadotropic
hypogonadism
(athletes,
anorexia). Also may be associated with Asherman’s syndrome
•Metrorrhagia
:
Irregular menstrual bleeding or bleeding between
periods
•Menometrorrhagia
:
Metrorrhagia associated with > 80 mL
•Polymenorrhea
:
Frequent menstrual bleeding. Strictly, menses
occur q 21 d or less
•Oligomenorrhea
:
Menses are > 35 d apart. Most commonly caused
by PCOS, pregnancy, and anovulation

• Bleeding is either irregular, heavy or
prolonged
• History should be helpful in determining
whether patient is ovulating
– If patient is ovulatory, she will have
monthly bleeding episodes
– If patient is not ovulatory, bleeding
will occur at irregular and unpredictable
intervals
• Have patient keep a menstrual calendar or
diary

• Anovulatory bleeding
– Caused by lack of progesterone production
by the ovary
– Patient will not have normal withdrawal
bleeding monthly
– Menses may be delayed for several months
and then be very heavy
– Hypothyroidism is a commonly associated
with
heavy
menses
and
intermenstrual
bleeding
• Examine thyroid, check thyroid function

• Anovulatory bleeding
– Patients who have long intervals
between
menses are at risk for developing
hyperplasia of the endometrium
–Treat
these
patients
with
progesterone monthly so they will
have withdrawal bleeding

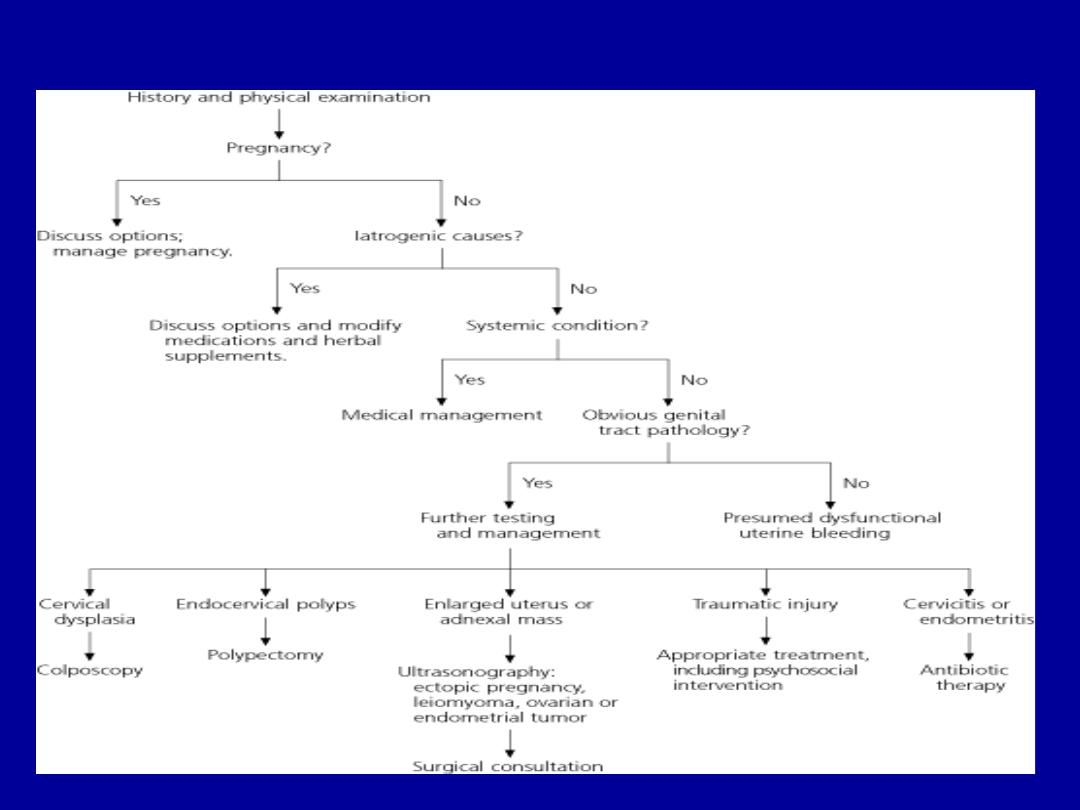
Abnormal Uterine Bleeding: Differential Diagnosis
•Structural
Cervical or vaginal laceration
Uterine or cervical polyp
Uterine leiomyoma
Adenomyosis
Cervical stenosis/Asherman’s (hypomenorrhea)
•Hormonal
Anovulatory bleeding
Hypogonadotropic hypogonadism
Pregnancy
Hormonal Contraception (i.e. OCPs, Depo-Provera)
Thyroid disorders
Hyperprolactinemia
•Malignancy
Uterine or Cervical cancer
Endometrial hyperplasia (potentially pre-malignant)
•Bleeding disorders
von Willebrand’s Disease, Hemophilia/Factor deficiencies,
platelet disorders
Abnormal Uterine Bleeding in Women of Childbearing Age

Invasive Cancer of the Cervix
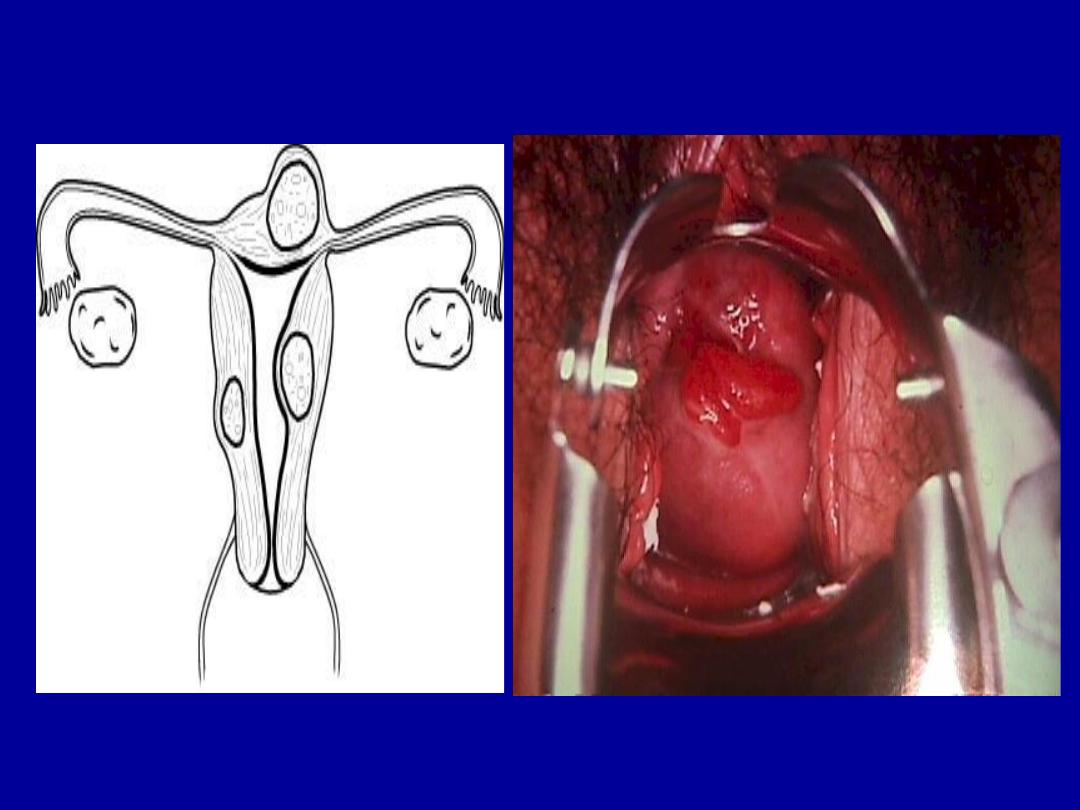
Mechanical factors
Fibroids
cervical polyps

•History
Timing of bleeding, quantity of bleeding, menstrual hx
including menarche and recent periods, associated sxs,
family hx of bleeding disorders
•Physical
R/o vaginal or cervical source of bleeding. Bimanual may
reveal bulky uterus/discrete fibroids
Assess for obesity, hirsutism, stigmata of thyroid disease,
signs
of
hyperprolactinemia
(visual
field
testing,
galactorrhea)
Pap smear
Endometrial biopsy, if appropriate
•Pregnancy Test
•Imaging
Pelvic ultrasound
Sonohystogram or hysterosalpingogram
•Surgical
Hysteroscopy
D & C
Life Phase
Ovulatory Status
Etiology
R/O Pregnancy
Adolescent Likely anovulation
Consider bleeding disorder
Pregnancy
Reproductive age
(Usually DUB)
Ovulatory
(Secretary)
Anovulatory
(Proliferative)
Hormonal
DUB
Anatomic
Coagulopathy
R/O Pregnancy
Perimenopause
Early EMB/TV Sono
Postmenopause R/O Endometrial CA
Dysfunctional uterine bleeding
Definition:
is abnormal uterine bleeding with no
demonstrable
organic
cause,
genital
or
extragenital.
Incidence:
10-20% usually at extremes of reproductive
life.
– 20% of cases are adolescents
– 50% of cases in 40-50 year olds
• Diagnosis of EXCLUSION
• Patients present with “abnormal uterine bleeding”
Diagnosis (by exclusion)
➢
History
➢
General examination
➢
Abdomino-pelvic examination
➢
Investigations (mainly to exclude
organic causes)

Possible Pathophysiology
1)
Shift in the endometrium conversion of
the endoperoxide from vaso-constrictor
PGF
2
a
2)
Increase in the level and activity of the
endometrium fibrinolytic system
3)
Effect
of
other
endometrial
derived
factors as cytokines, growth factors and
endothelins.
Treatment
I.
Medical treatment
A. Non-steroidal
anti-inflammatory
drugs
➢
Mechanism of action: inhibit
cyclo-oxygenase enzyme and the
production of prostaglandins
➢
Phospholipids
phospholipase A
2
arachidonic acid
cyclo-oxygenase
prostaglandins
Effectiveness:
1.
Decrease measured menstrual loss by
40% in 75% of patients
2.
Relief dysmenorrhoea
3.
Little effect on regularity of cycle or
duration of bleeding
Side effects:
➢
Mainly
mild
gastrointestinal
tract
irritation
➢
The treatment should start immediately
with the start of bleeding.
B. Antifibrinolytic agents
Mechanism of action
:
Prevent conversion of plasminogen
into plasmin which dissolve the
fibrin clots occluding the blood
vessels.
Effectiveness
:
➢
Reduce measured loss by 40-50%.
The effect is dose related. It should
be
given
with
the
start
of
menstruation and continue for 3-4
days.

➢
Comparative studies suggested that
tranexemic acid is more effective than
PG synthetase inhibitors (Milsom et
al.1991; Bonnar and Shepard 1996).

Side effects:
1.
Mild gastrointestinal tract irritation
2.
Serious
adverse
effect
has
been
documented (intracranial thrombosis –
central venous stasis retinopathy) but
they are extremely rare.

3.
No such complications occurred in
Scandinavia over 19 years (1
st
line of
treatment there
4.
Should not prescribed for women with
history of thrombo-embolism.
II.
Hormonal treatment:
1.
Oral contraceptive pills
➢
One of the most effective treatments
available for both menorrhagia and
dysmenorrhoea
➢
Can be used safely in women over 40
years if they are of low risk category
➢
Mechanism of action:
Mainly locally
by inducing endometrial
atrophy with reduction in both PG synthesis
and fibrinolysis.
➢
Side effects:
i.
That of oral contraceptive pills in general
ii.
Socially
unaccepted in
single
unmarried
women.
1.
Progestogens
Norethisterone–medroxy-progesterone
acitate.
Are the most commonly prescribed
preparations in UK because it was wrongly
thought that the majority of women with DUB
are anovulatory
➢
Mechanism of action:
1.
In anovulatory cycle it induce secretory
changes but in ovulatory
cycle it
produce minimal changes
2.
Norethisterone is given as 5mg t.d.s. for
21 days while Provera is given as 10 mg
for 10-14 days during luteal phase.

➢
Effectiveness:
1.
If given in high dose for 21 days
especially in anovulatory cycle it reduce
menstrual loss by 80% (Irvin et al.,
1998)
2.
In anovulatory cycle it convert irregular,
unpredictable
bleeding
into
regular
controlled one which is an attractive
feature for many women.

Side effects
:
Usually
minimal
as
abdominal
bloating and weight gain
Progesterone releasing devices
Produce marked reduction in menstrual
blood loss up to 80%
➢
Mechanism of action:
mainly locally
leading to atrophic endometrium with
very minimal systemic effect

➢
Effectiveness:
Scandinavian
study
(milson et al.,1991) showed decreased
menstrual loss by 90%.
➢
Side
effects:
irregular
bleeding
is
common especially in the in the early
months.
Danazol:
Is an extremely effective drug for
treatment of menstrual problems but its
use is limited by its high androgenic
side effects

Gonadotrophin releasing hormone agonist
➢
Mechanism of action:
produce down
regulation
of
pituitary
gland
that
decrease gonadotrophins and ovarian
steroids
➢
Effectiveness:
relief in 90% of cases.
Also relief PMS
Side effects
:
➢
Hypo-estrogenic state and osteoporosis
(add estrogen and progesterone if used
for long period)
➢
Unless used to prepare the patient for
endometrial ablation it is not accepted
by most patients for long term.
Surgical treatment
Suitable for older patients who have no
further wish to conceive.
I.
Endometrial ablation/resection
To remove or destroy the endometrium
producing changes similar to Asherman’s
syndrome (Laser – electrocautary - roller
ball
-
diathermy
– microwave- hot
balloon).

Advantage over hysterectomy
1.
Short hospital stay and return to work
2.
50% of patients were amenorrhoeic,
30-40% experienced marked reduction
in menstrual loss
3.
70% or more were satisfied

Disadvantages
:
1.
Needs experience
2.
Recurrence of about 20%
3.
Operative complications as perforation
4.
Post operative pain
II.
Hysterectomy
Definitive
cure
for
menorrhagia
(Abdominal, vaginal or laparoscopic)
(total or subtotal)
Disadvantages:
1.
Mortality of 6/10000 procedures
2.
Injury of ureter, bladder or bowel.