Chest Trauma
Chest Series
Tikrit University
College of Medicine
Department of Radiology
Chest trauma
• Types of trauma:
1. Blunt
2. Penetrating
3. Explosion Related
Trauma Chest Radiograph
• Usually AP, often
supine, frequently in
poor inspiration.
• So, a challenge to
interpret.
CT Chest
More sensitive and specific
Chest Trauma
May Result In:
1. Fractures & Dislocations of
Spine, Ribs,
Clavicles, Sternum, Shoulders
2. Flail Chest
3. Pneumothorax & Hemopneumothorax
4. Pneumo-mediastinum
5. Pneumo-pericardium &
Hemopericardium- cardiac tamponade
6. Surgical emphysema

Pneumothorax
What is a pneumothorax?
• Air within the pleural cavity (i.e. between
visceral
and
parietal
pleura)
• The air enters via a defect in the:
– visceral pleura (e.g. ruptured bulla) or
– parietal pleura (e.g. puncture following rib
fracture)
CXR
features
of pneumothorax
1. White line of visceral pleura parallel to
chest wall
2. No lung markings lateral to the line
3. There may be associated rib fractures
• Do not confuse the line with skin fold or
with scapula
• Expiration film is better.
• CT is the most sensitive imaging modality
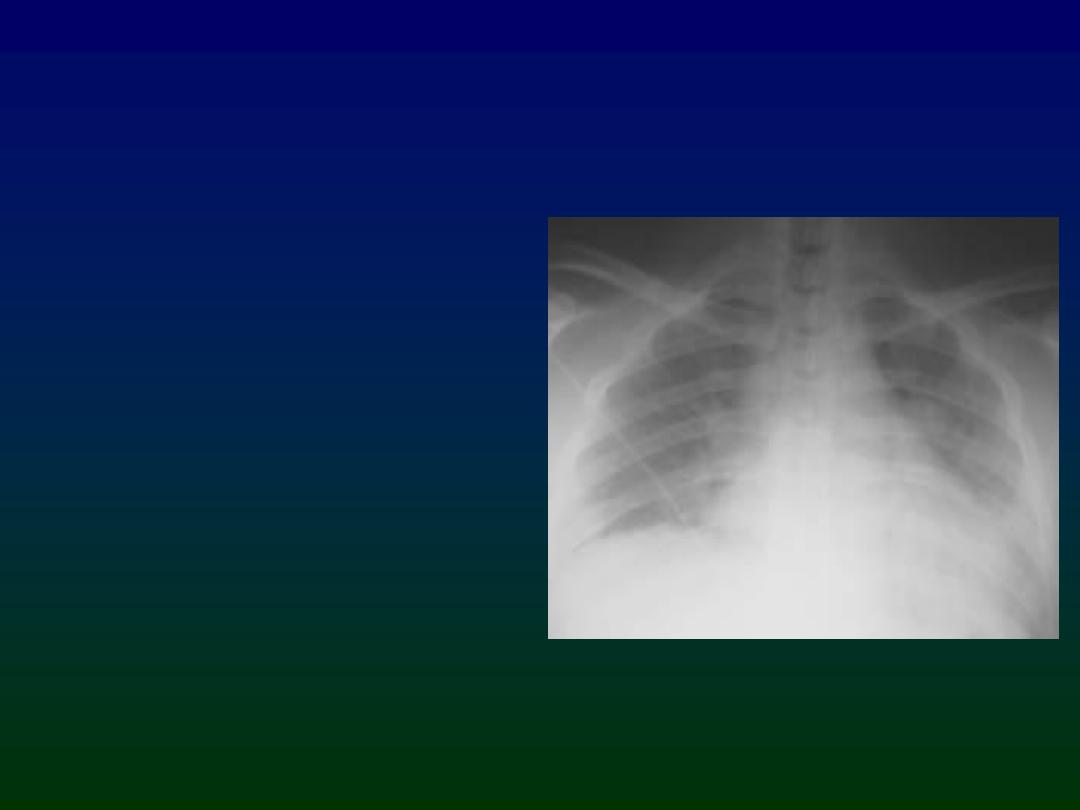
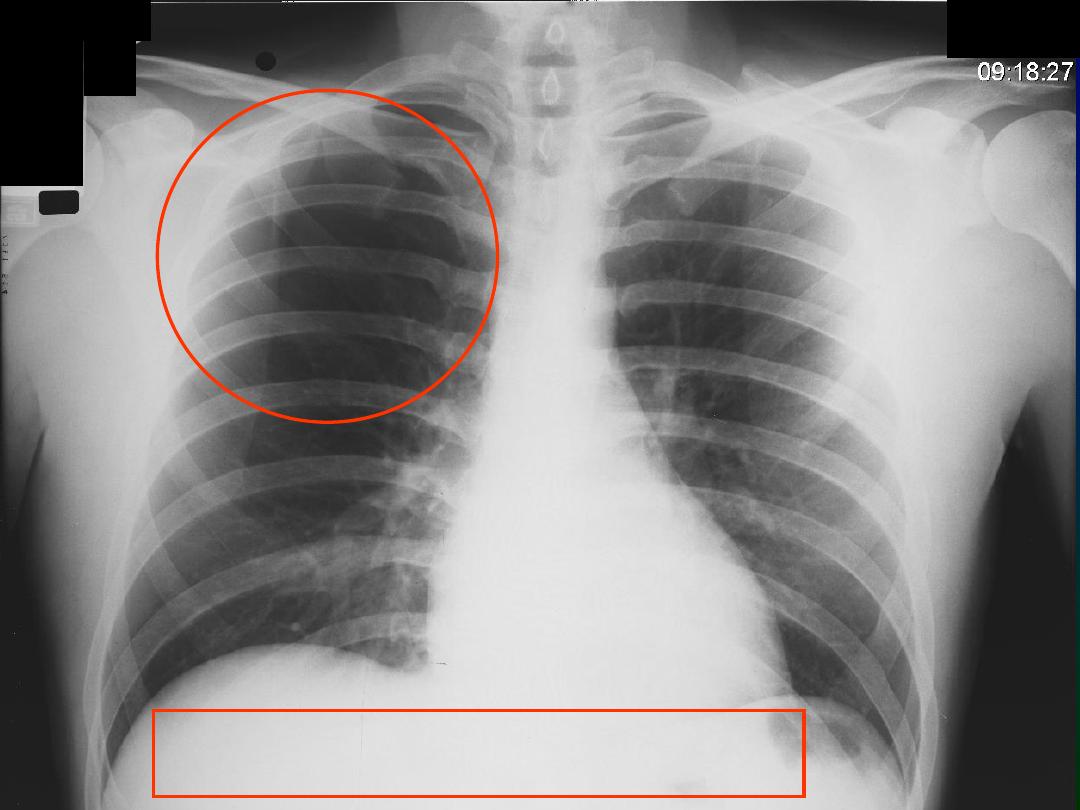
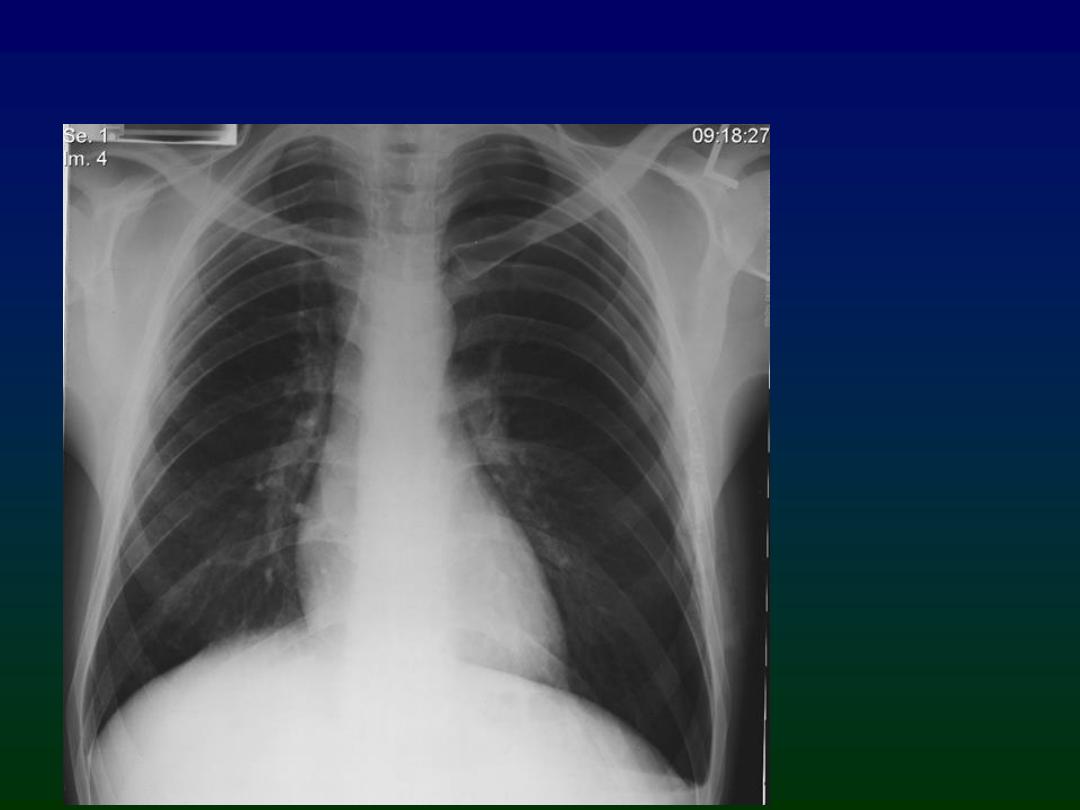
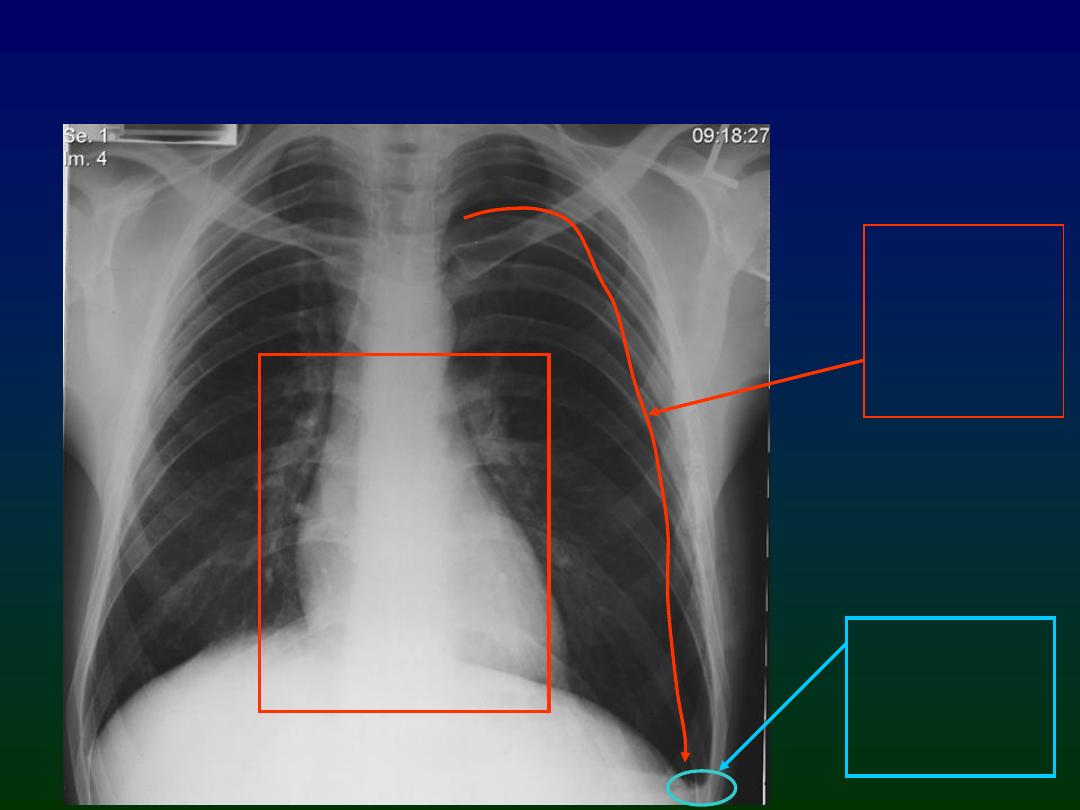
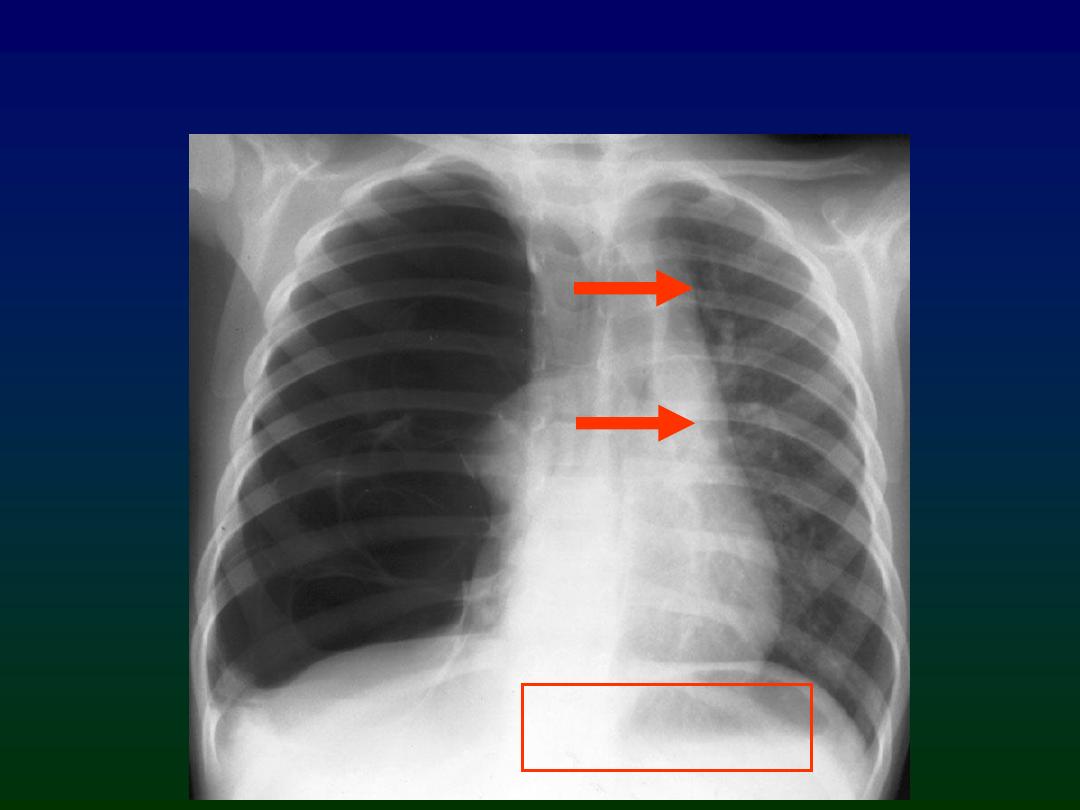
Look at the CXR on the next slide. Where is the pneumothorax?

R
R
•Right lung more translucent than left
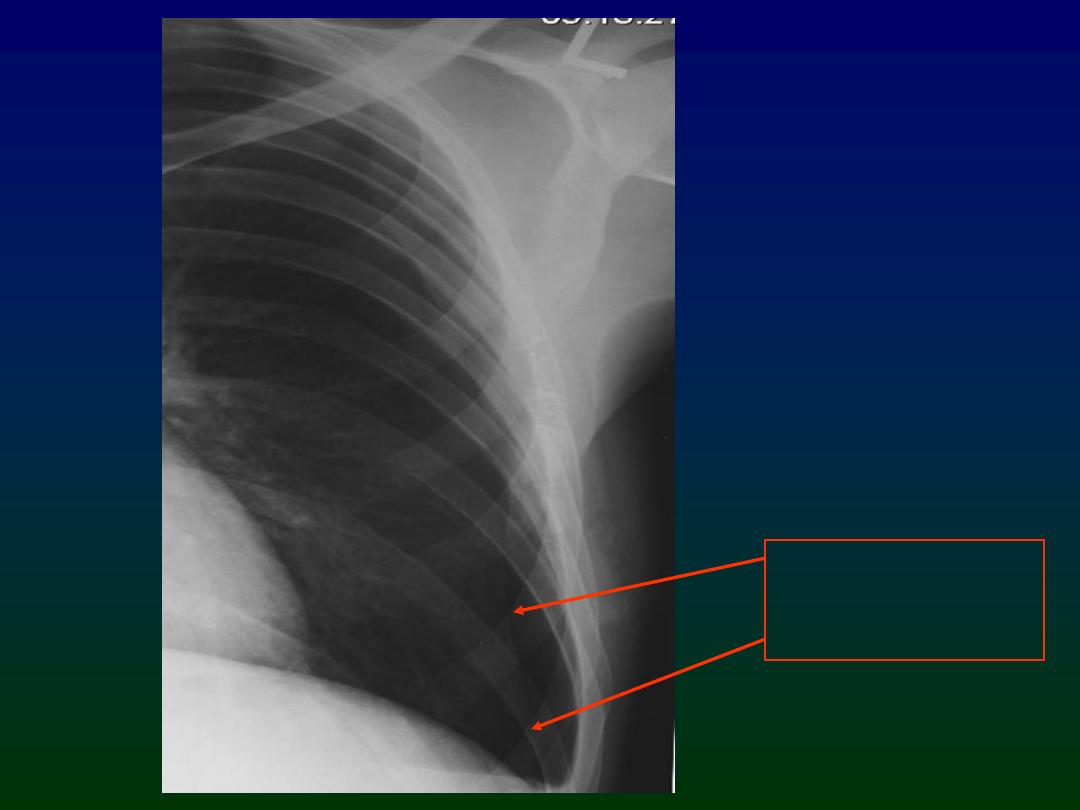
•Faint line just visible (zoomed view to follow)
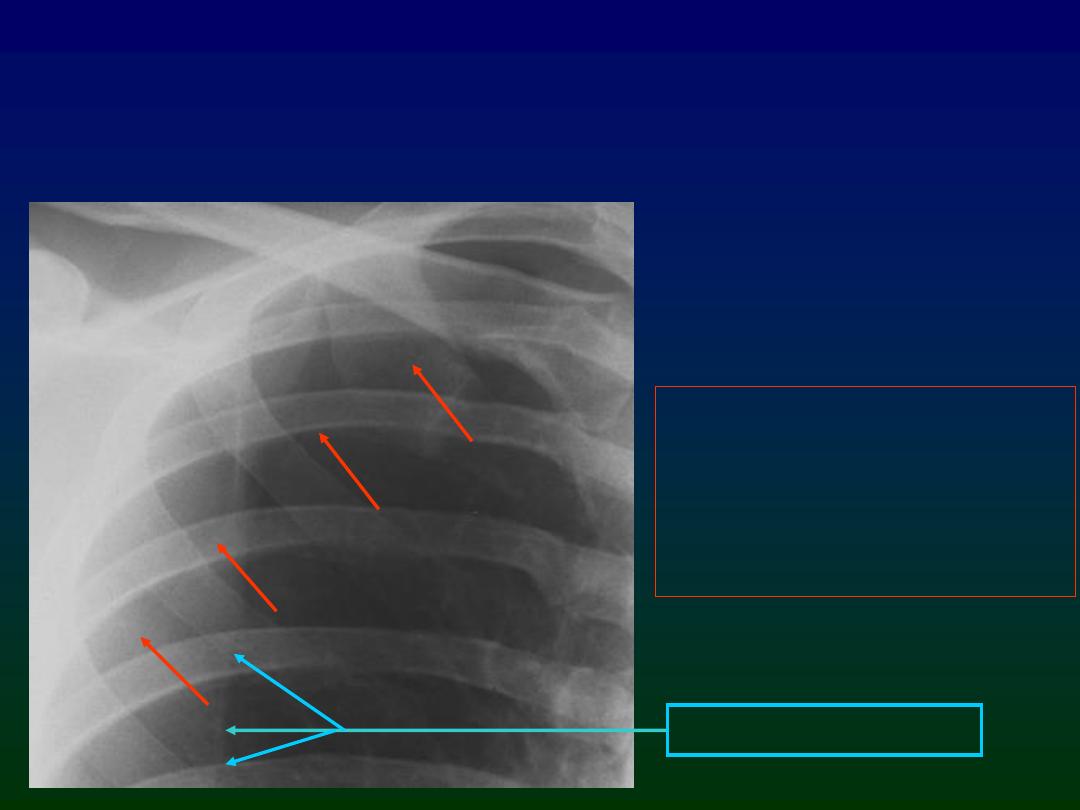
•Pencil-thin white line
running parallel to chest
wall
•No lung markings lateral
to the line
Blade of right scapula
Right pneumothorax
Types of Pneumothorax
• Simple
– Mediastinum remains central
– Clinical condition stable
– Radiological features: mentioned before.
• Tension
– The clinical condition is unstable
– Progressive build up of air in the pleural space.
– Radiological features:
1.
Hyper lucency of affected hemi thorax + previous features
2.
Flattening of ipsilateral hemi diaphragm.
3.
Contra lateral shift of mediastinum
4.
Collapsed ipsilateral lung ± contra lateral shift
– Do not late, chest tube is life saving. Death will result if not
quickly recognized and treated with needle decompression.
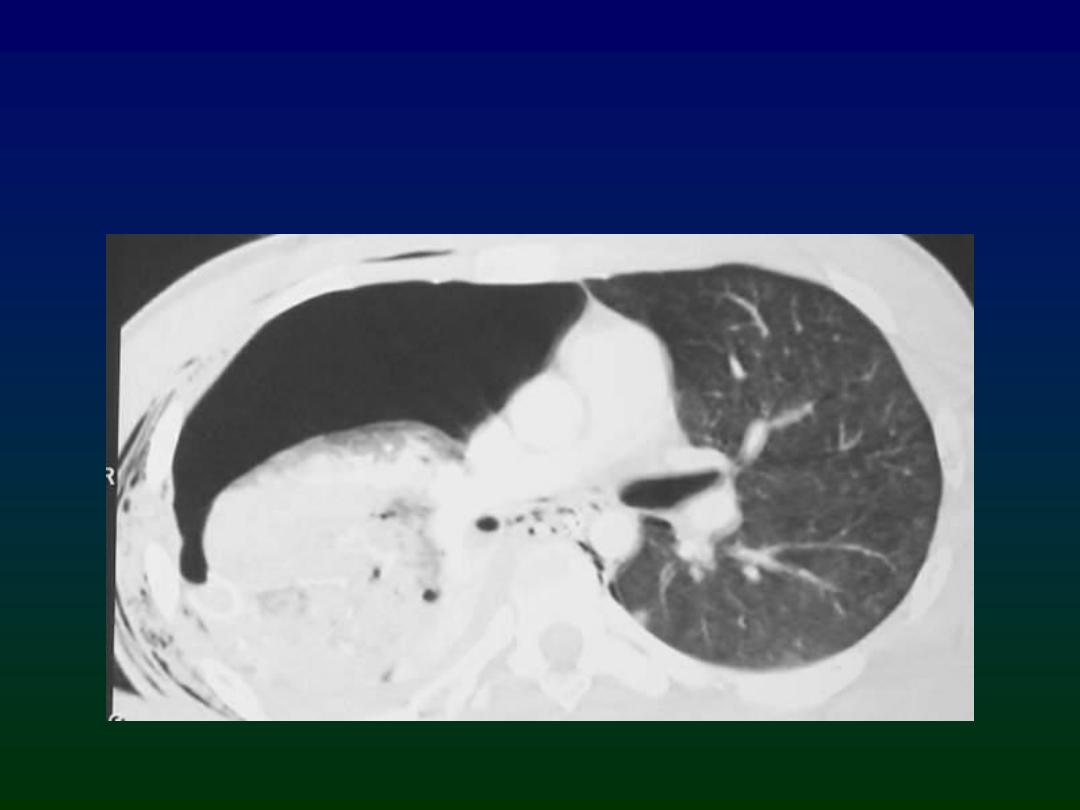
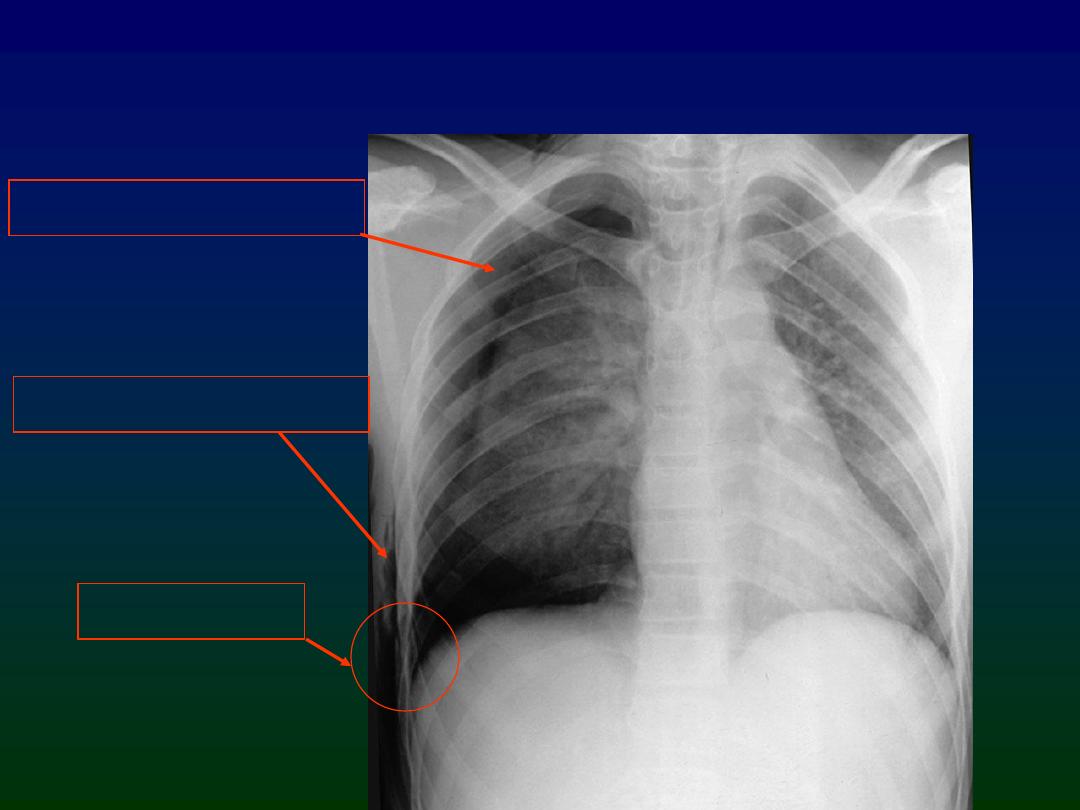
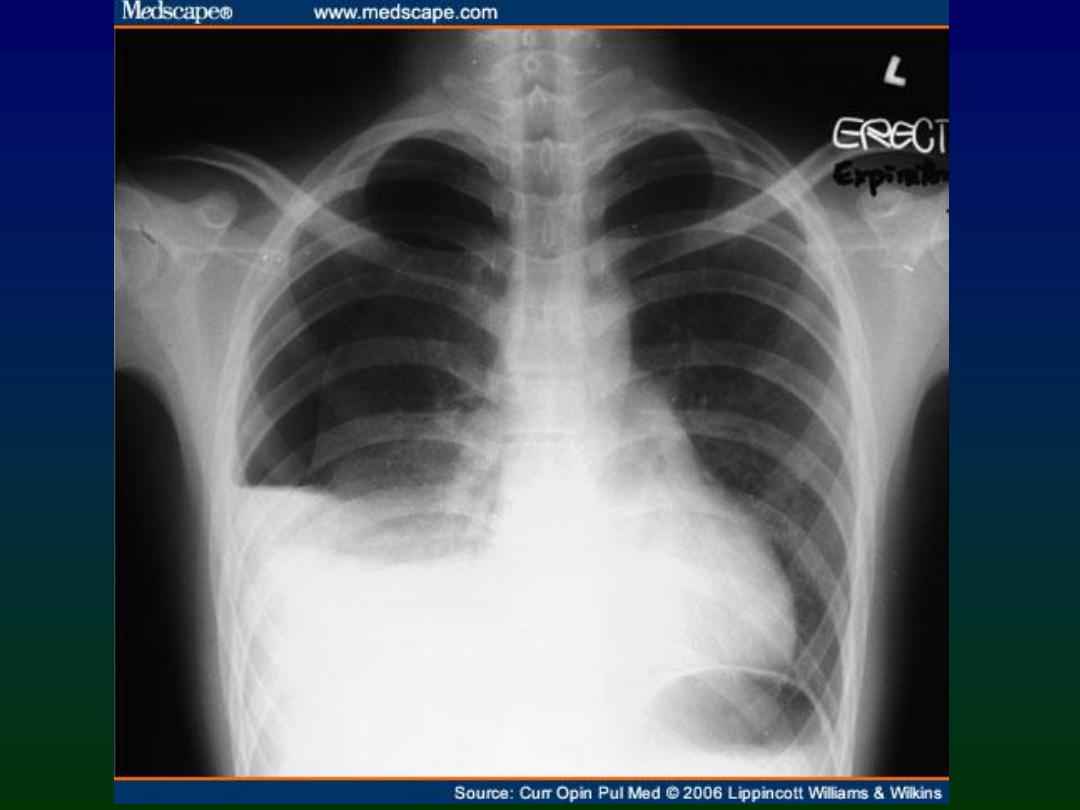
Simple Left Pneumothorax
Simple Left Pneumothorax
No mediastinal shift
Small pleural
effusion
(common
finding)
Visceral
pleural line
(zoomed
view on next
slide)
Note absence of
lung markings
lateral to this line

Pneumothorax with rib fractures
Pneumothorax with rib fractures
Surgical emphysema
Right pneumothorax
Rib fractures
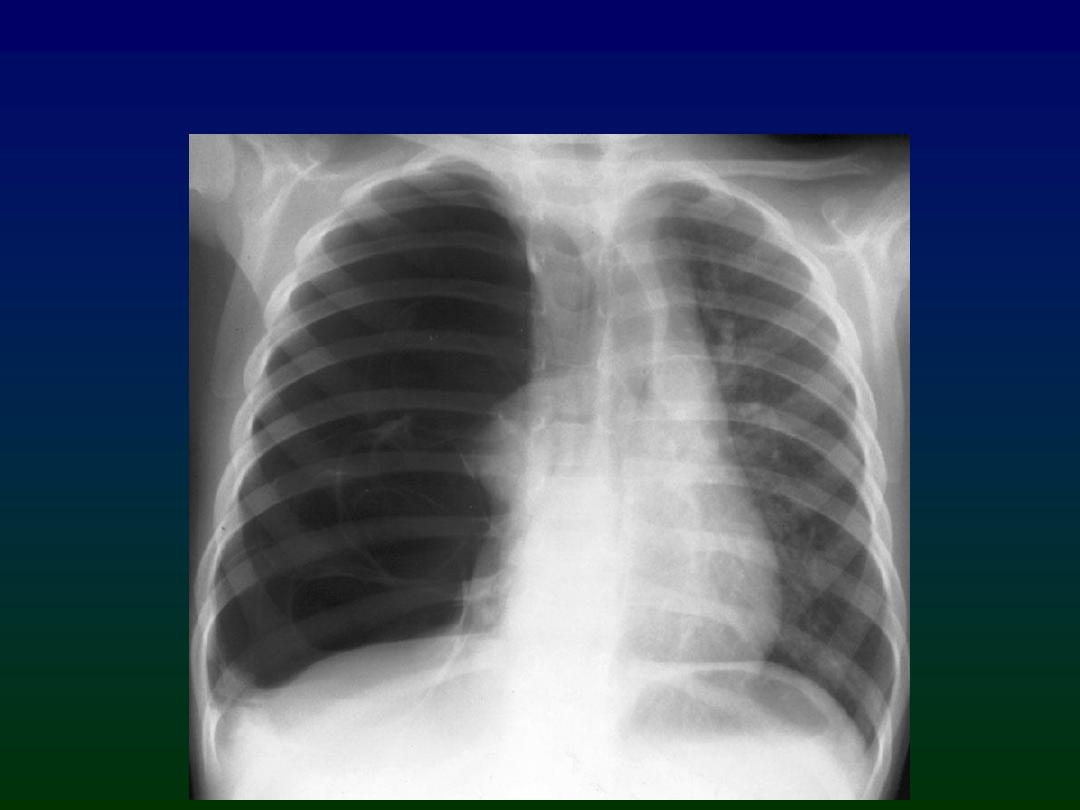
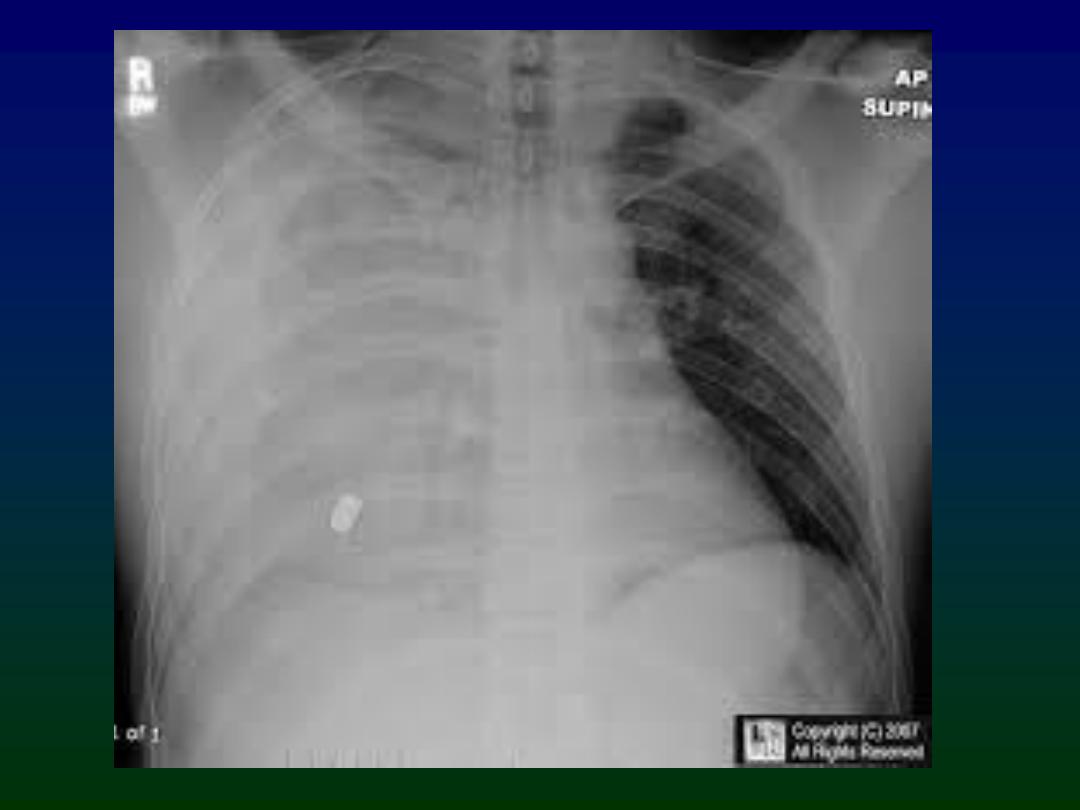
Tension right pneumothorax
Tension right pneumothorax
Mediastinal shift to
left
Causes of Pneumothorax
• Spontaneous
– Rupture of an apical bleb
• Traumatic
– With rib fractures
– Penetrating chest trauma
• Pre-existing lung abnormality
– Pulmonary fibrosis
– Asthma
– Vasculitis
– Pulmonary metastases close to edge of lung
Other causes of absent lung markings
• Large emphysematous bullae
• Large lung cysts
• Pulmonary embolism
....but only pneumothorax has a white
line parallel to the chest wall
Take Home Points
• Look for a pencil-thin white line parallel to
the chest wall
• No lung markings lateral to the line
• Make sure the patient does not have another
cause for absent lung markings before
inserting a chest drain
• In tension pn.thx : Death will result if not
quickly recognized and treated with needle
decompression
HEMOTHORAX
• Blood accumulation in chest cavity
• May occur slowly or rapidly depending on
size of disrupted blood vessel
• May occur due to penetrating or blunt
trauma
• In massive hemothorax, blood loss is
complicated by low oxygen levels in blood
(hypoxia)
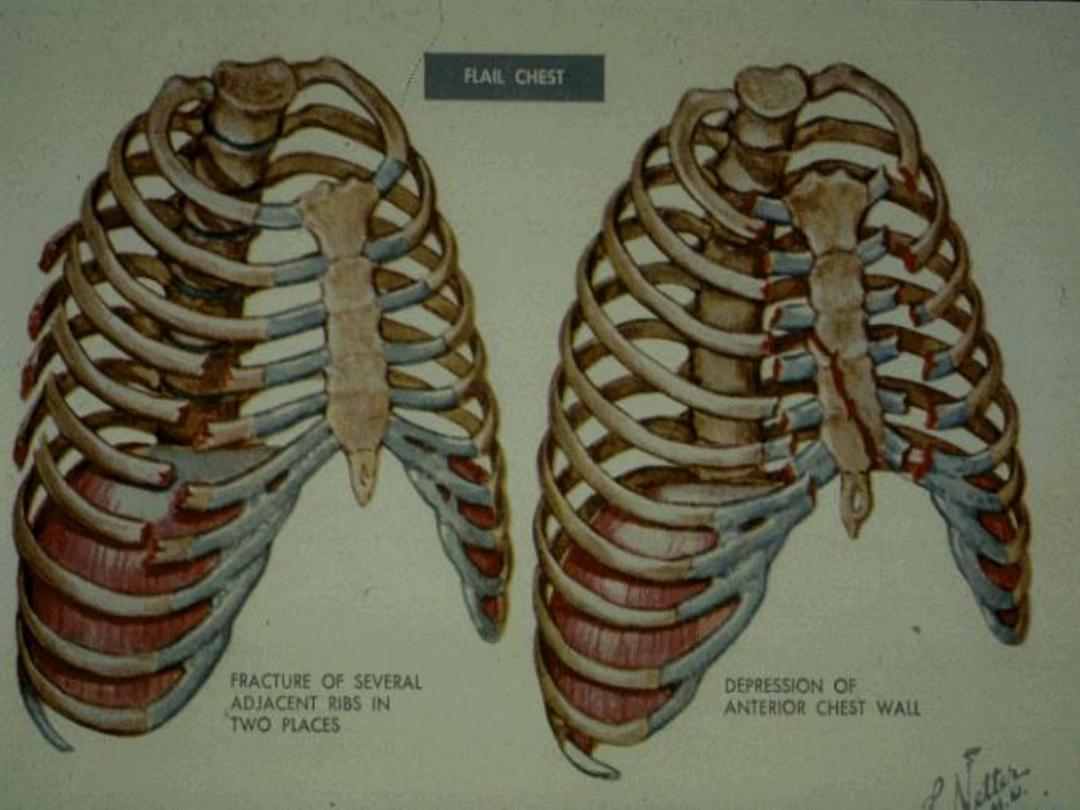
FLAIL CHEST
• Three or more ribs fractured in two or more
places or a fractured sternum
• Severe pain at site
• Rapid shallow breathing
• Paradoxical respirations (may be difficult to
detect initially)
• Pneumothorax may be present
• Possible underlying contusion to lung could lead
to hypoxia
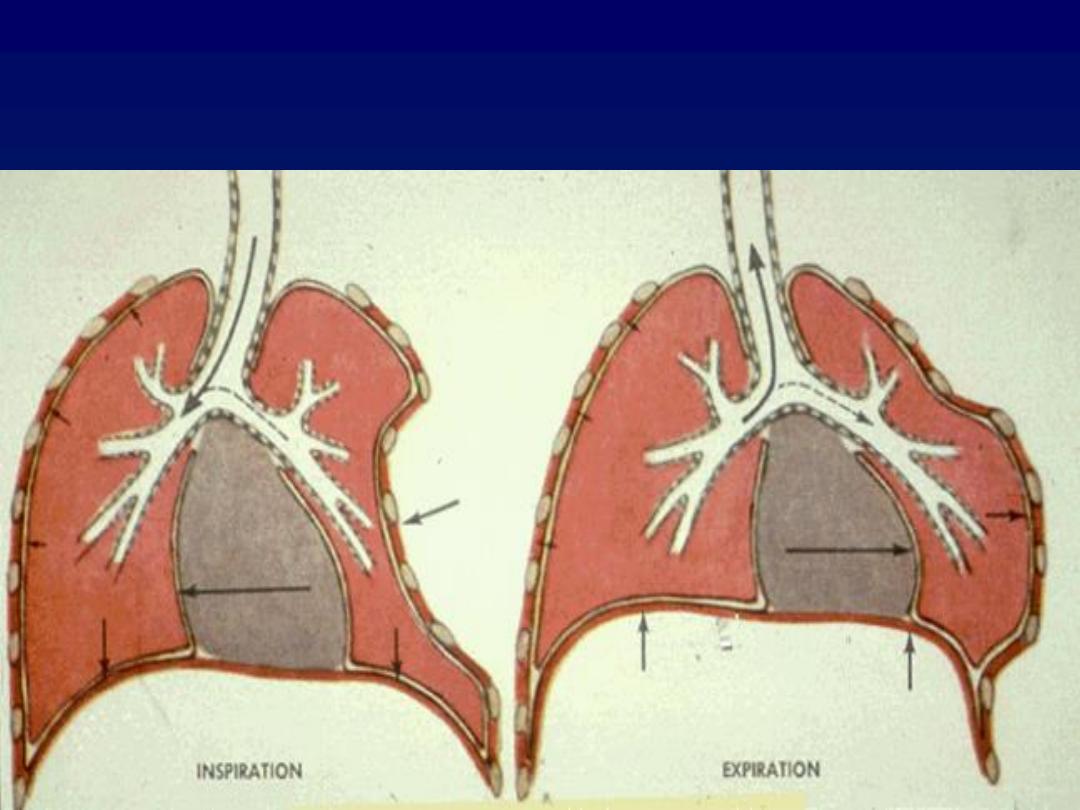
PARADOXICAL RESPIRATIONS