BONE INFECTION
a)
Osteomyelitis
b)
Pott’s Disease
c)
Congenital Infections
a) Osteomyelitis :
1-incidence
2-Etiollogy
3-Location
4-Radiographic Feature
1- Incidence :
Refers to bony inflammation that is almost
always due to infection, typically bacterial
Osteomyelitis can occur at any age, in
those without specific risk factors it is
particularly common between the age of
2-12 years and is more common in
males
Three
noitcefni fo setuor
era
dezingocer
:
1:
Hematogenous
2:
Direct inoculation
3:
Local extension from contiguous infection
3-Location
:
-Tubular bones with most rapid growth and
largest
metaphyses are most commonly affected,
75% :
femur > tibia > fibula; distal end > proximal
end
-Flat bones are less frequently infected,
25% :
vertebral bodies, iliac bones
-Neonates : metaphysis and/or epiphysis
-Children : metaphysis
-Adults : epiphyses and subchondral regions
-
Children
(unifocal) : Staphylococcus (85%),
Streptococcus (10%)
-
Neonates
(multifocal) : Streptococcus,
Staphylococcus
-
Immunocompromised adults
: short bones of
hand and feet : Staphylococcus
-
Drug addicts
: Pseudomonas (85%), Klebsiella
-
Sickle cell disease
: Salmonella
-In otherwise healthy adults, hematogenous
osteomyelitis is very rare, osteomyelitis in
adults usually follows direct implantation after
surgery or trauma
4- Radiographic Features:
1- plan Radiography
2- MRI
3- Nuclear Medicine
1-Plain Radiography :
a) Soft tissue swelling :
-Earliest sign
-Often in the metaphyseal region
-Loss or blurring of normal fat planes
b) Regional osteopenia
c)
Cortical loss
, 5 to 7 days after
infection, bone destruction
d) periosteal reaction / thickening

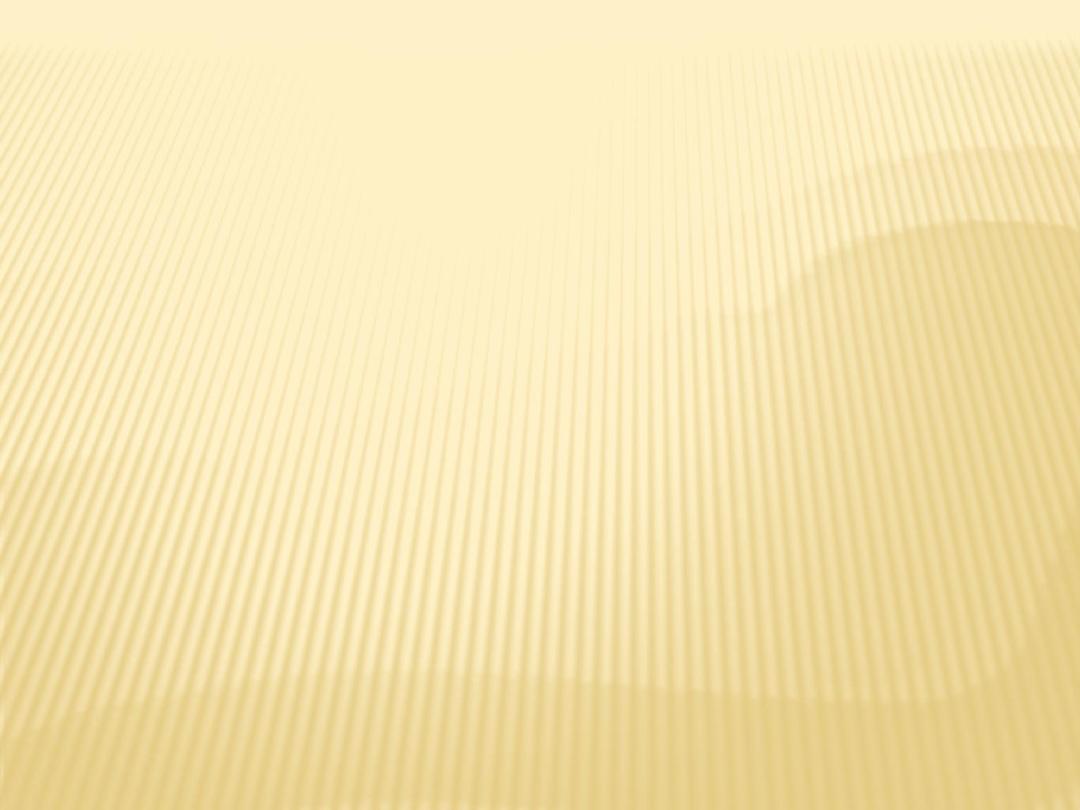
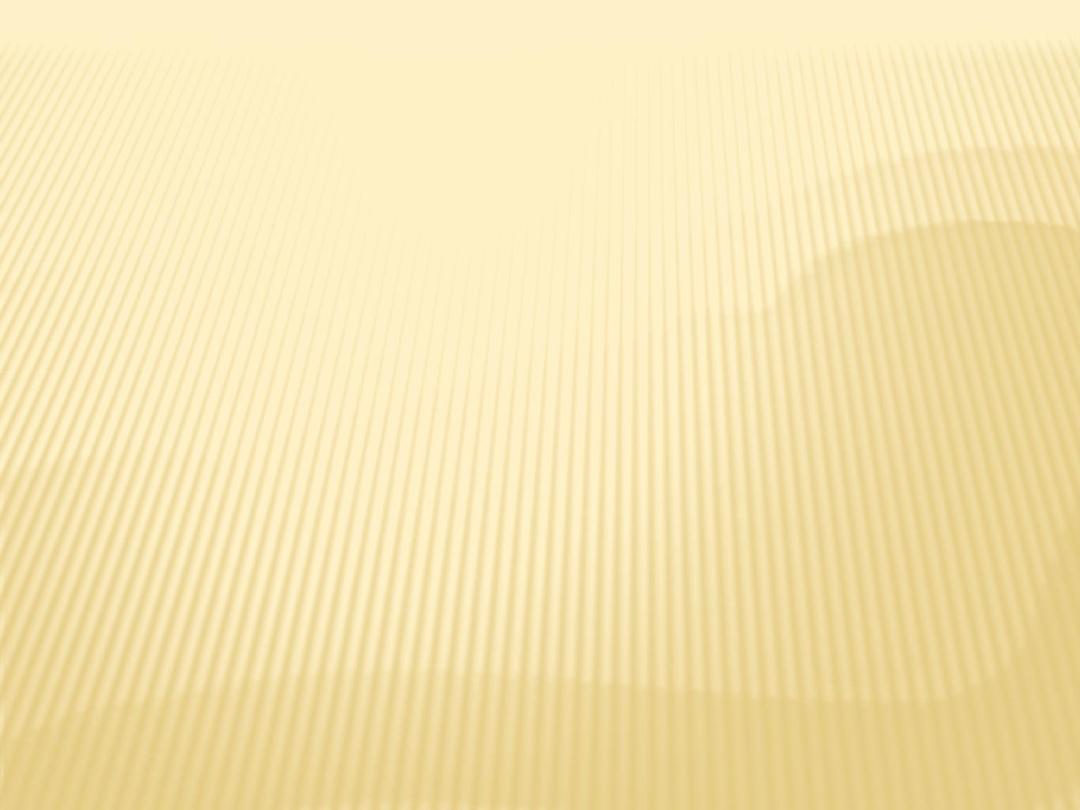
Soft tissue swelling with bone destruction

OM of RT tibia in a neonate
OM distal radius

Diabetic OM

Thumb OM
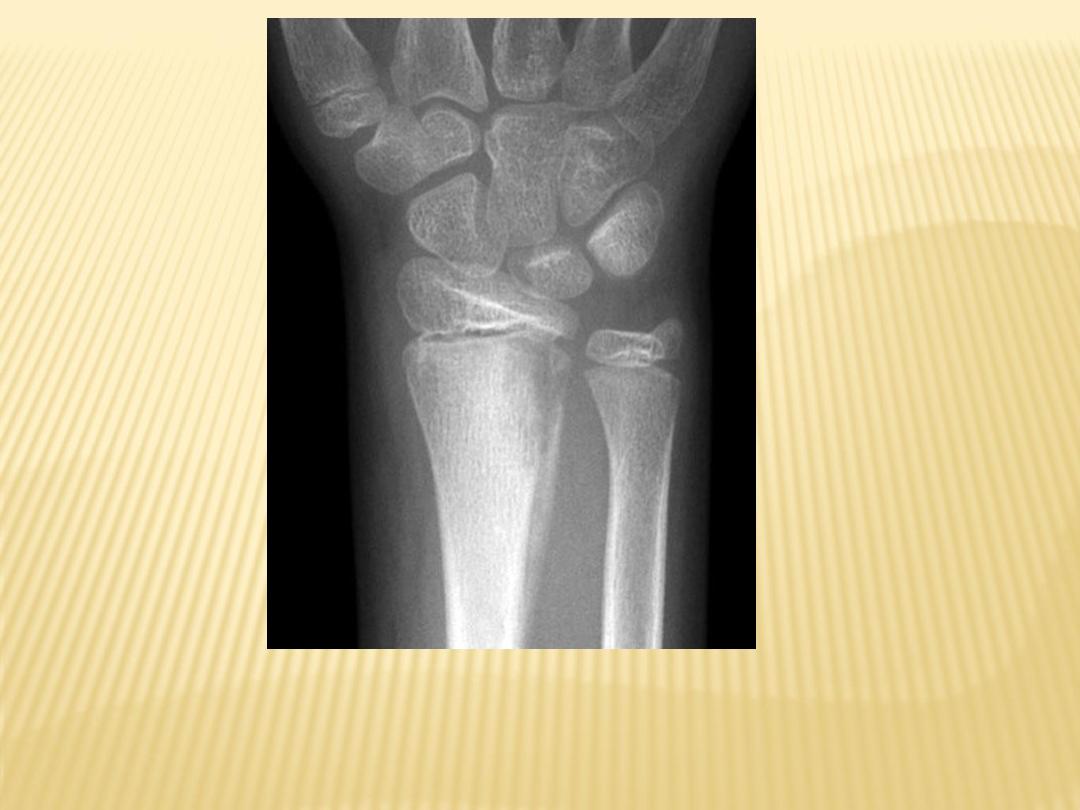
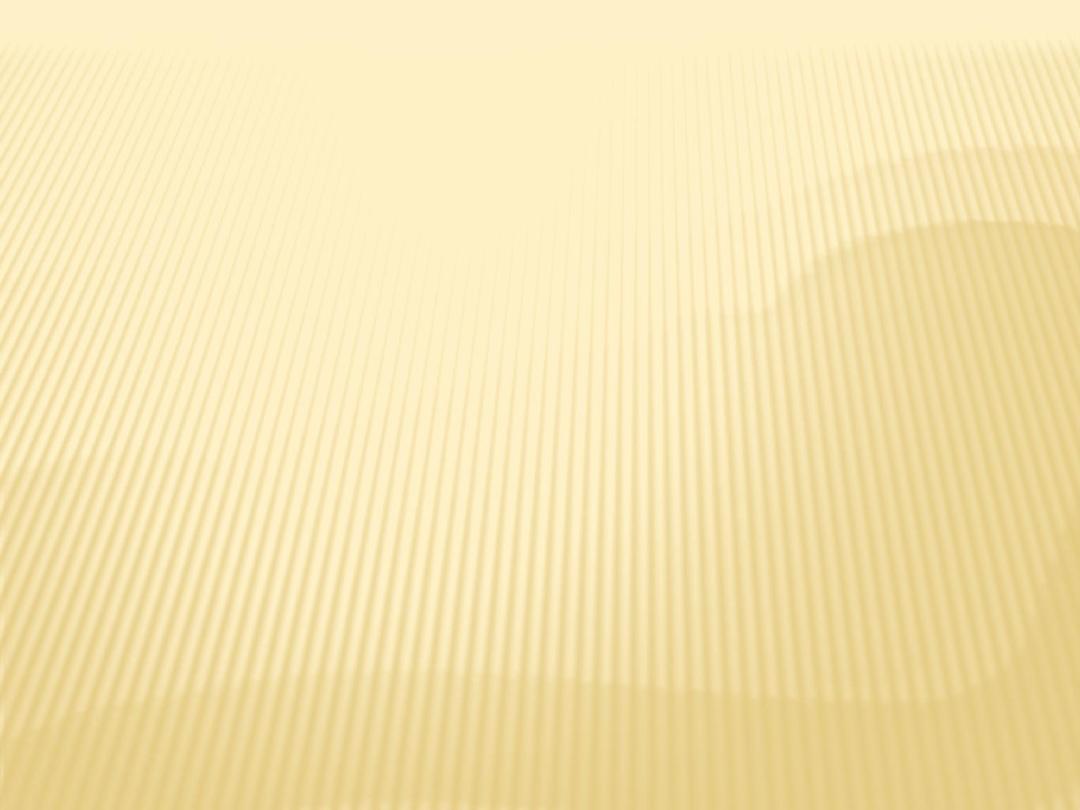
OM humerus

Bone destruction of head of 2nd metatarsal with periosteal new bone formation
characteristic of osteomyelitis
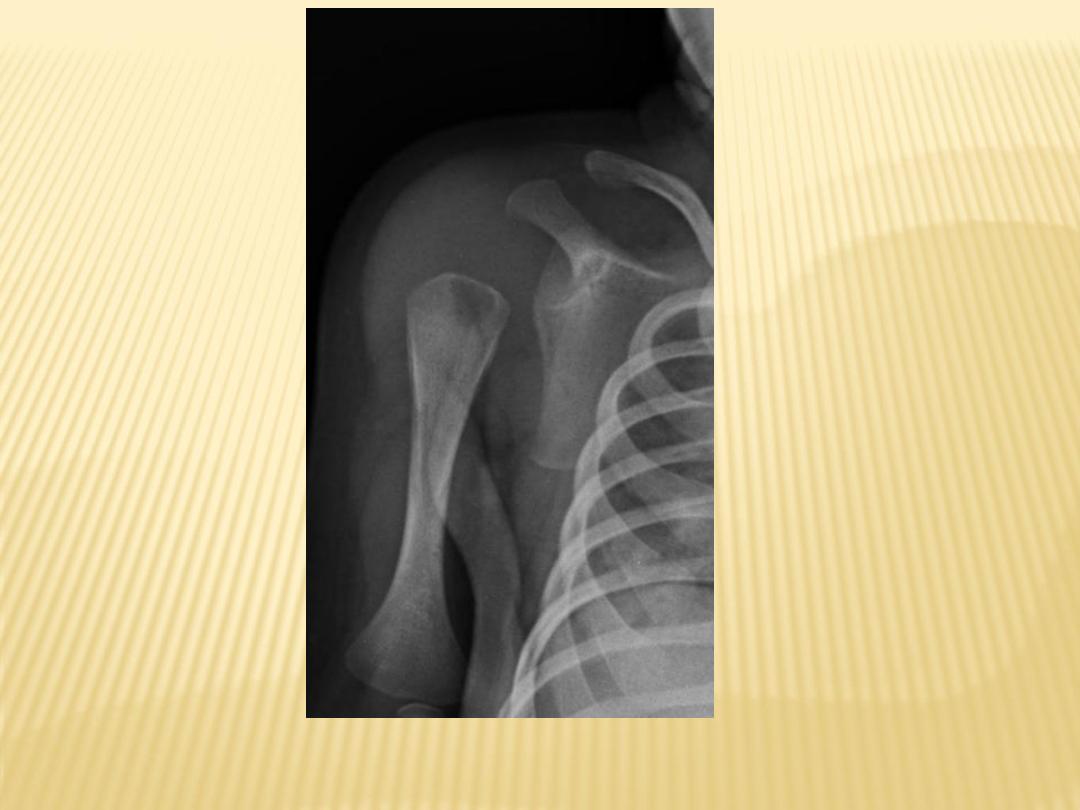
Periosteal reaction

A periosteal reaction can be seen and the femur is osteopaenic

Periosteal elevation (left-image arrowhead) and osteolysis (right-image
arrowhead) findings consistent with osteomyelitis
e) In untreated cases eventual formation of :
1-Sequestrum :
-Devascularization of a portion of bone with
necrosis and resorption of surrounding bone
leaving a floating piece.
-In some instances the sequestrum becomes
encased in a thick sheath of periosteal new
bone known as an involucrum.
2-Involucrum :
-Thick sheath of periosteal new bone
surrounding a sequestrum.
3-Cloaca :
-Space in which dead bone resides
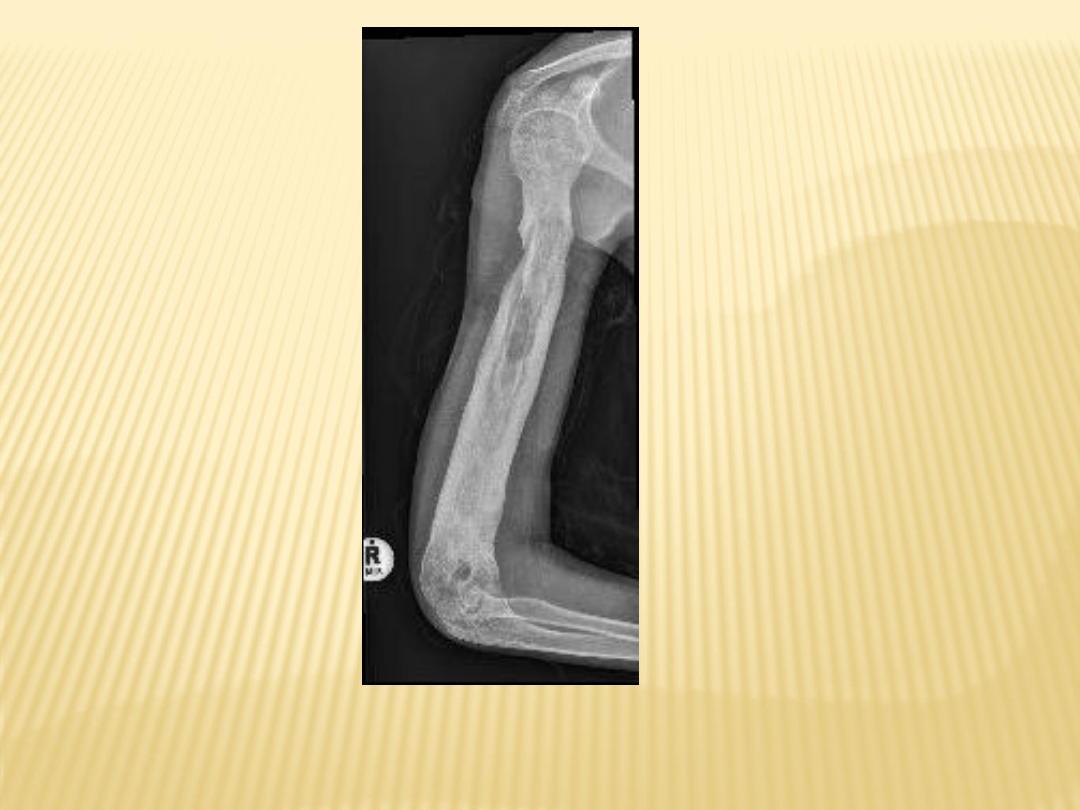
Sequestrum
f) Chronic Osteomyelitis :
1-Brodie's abscess :
-Lucent well-defined lesion with thick
sclerotic rim
-Lucent tortuous channel extending
toward growth plate prior to physeal
closure (pathognomonic)
-Typically in metaphysis or diaphysis of
long bones
2-Thick and dense cortex
3-Sinus tracts to skin
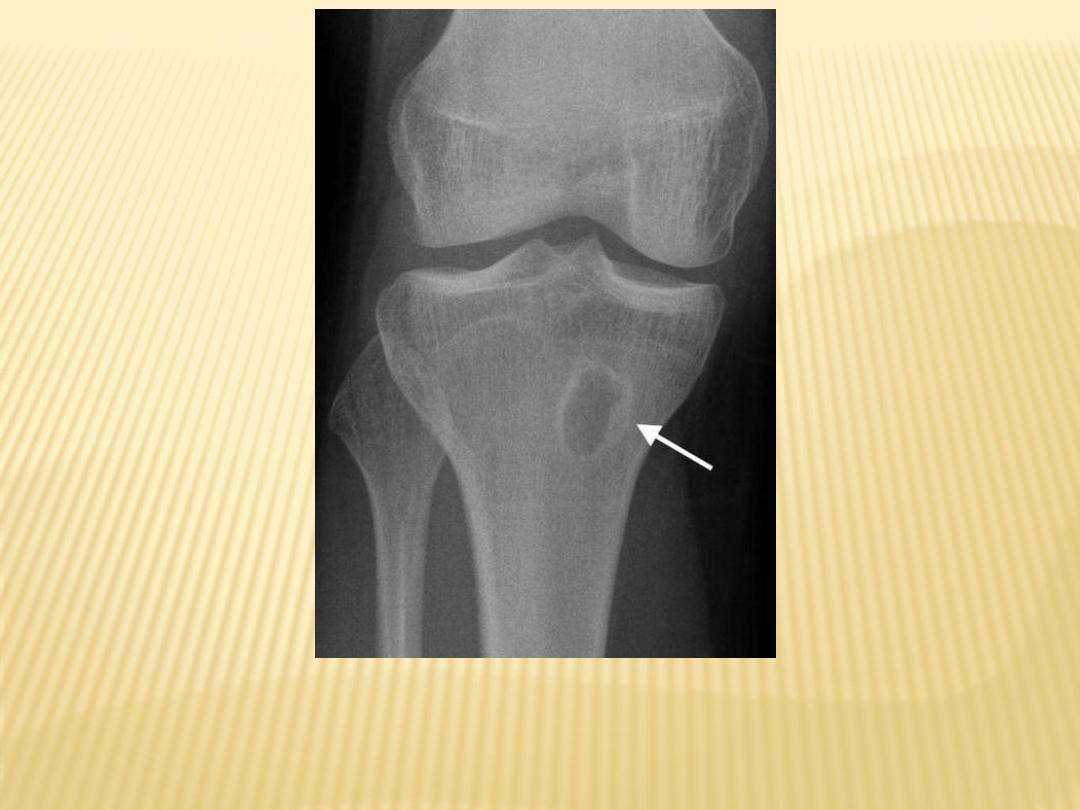
Brodie's abscess

Brodie's abscess
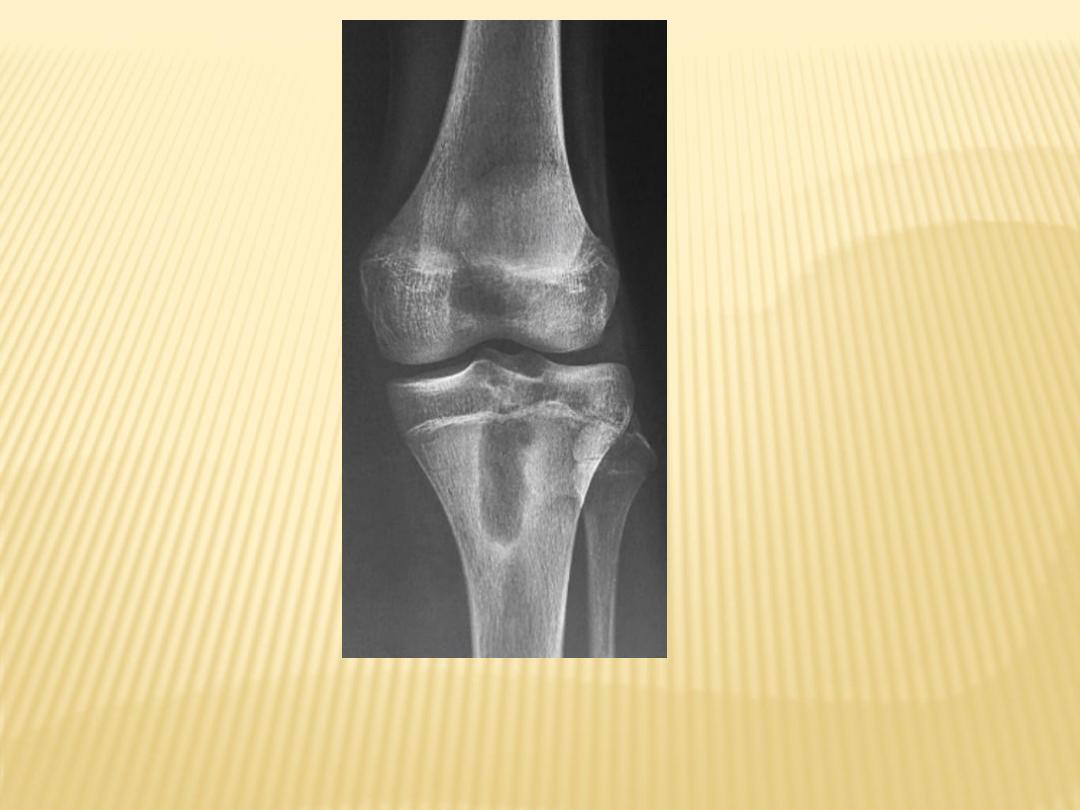
Brodie's abscess

Brodie's abscess
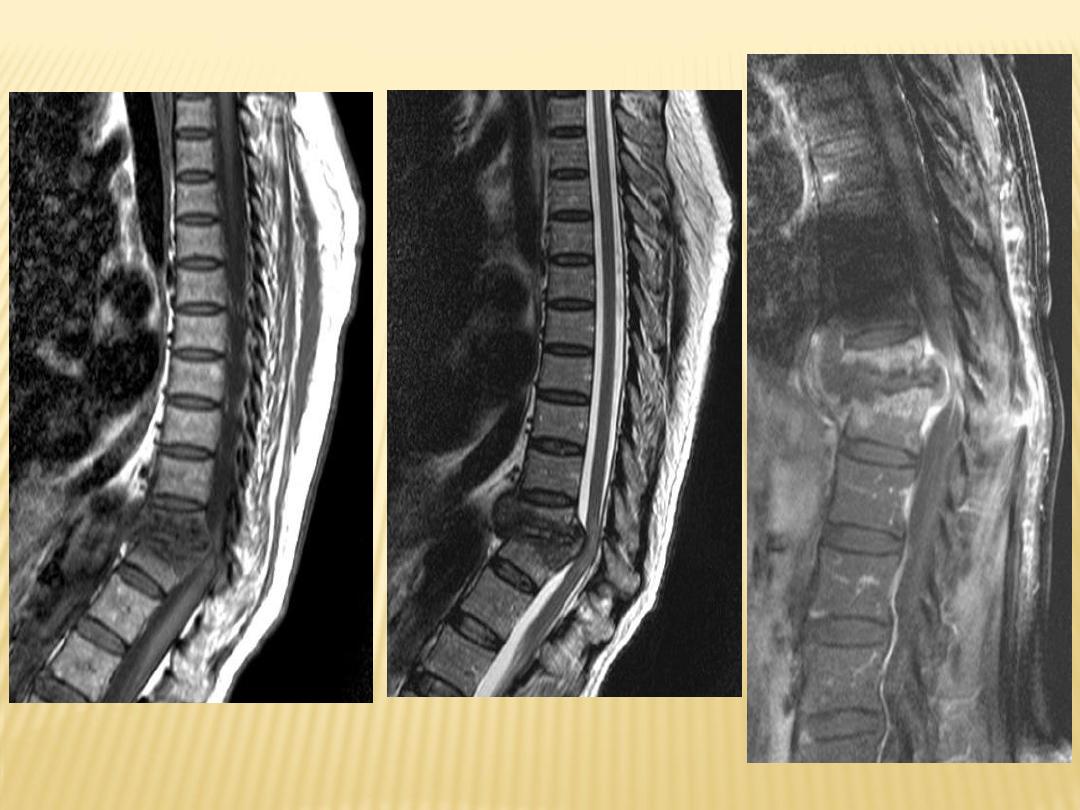
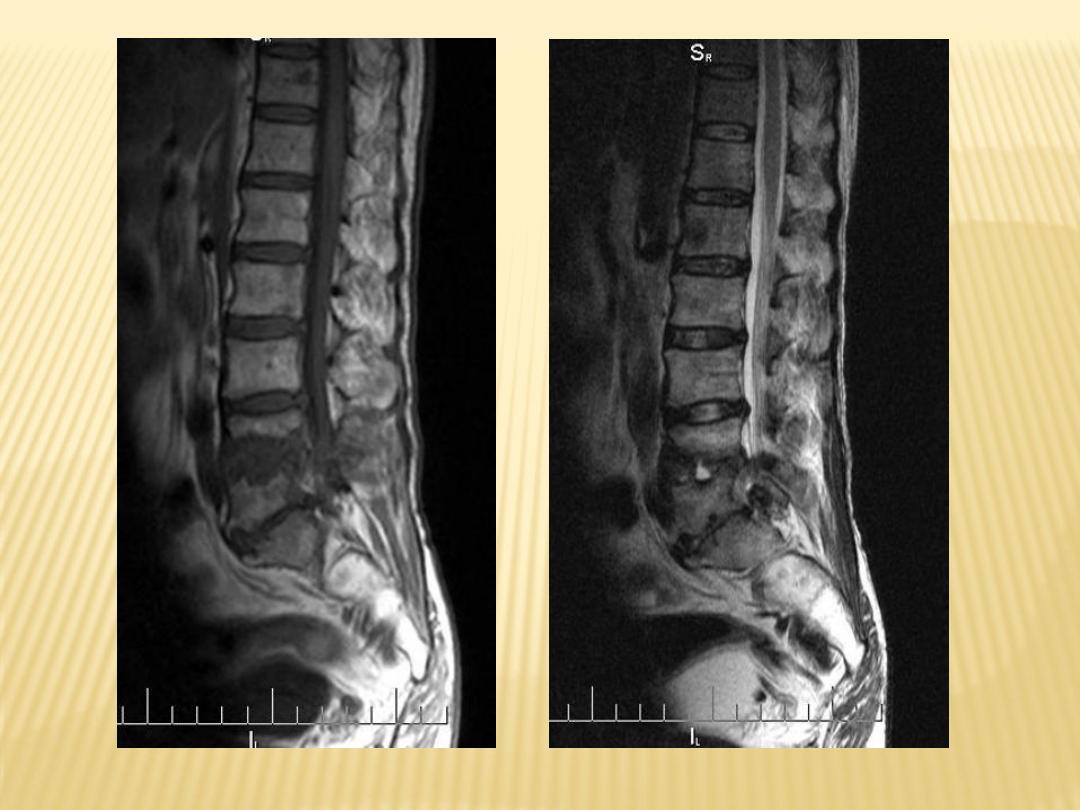
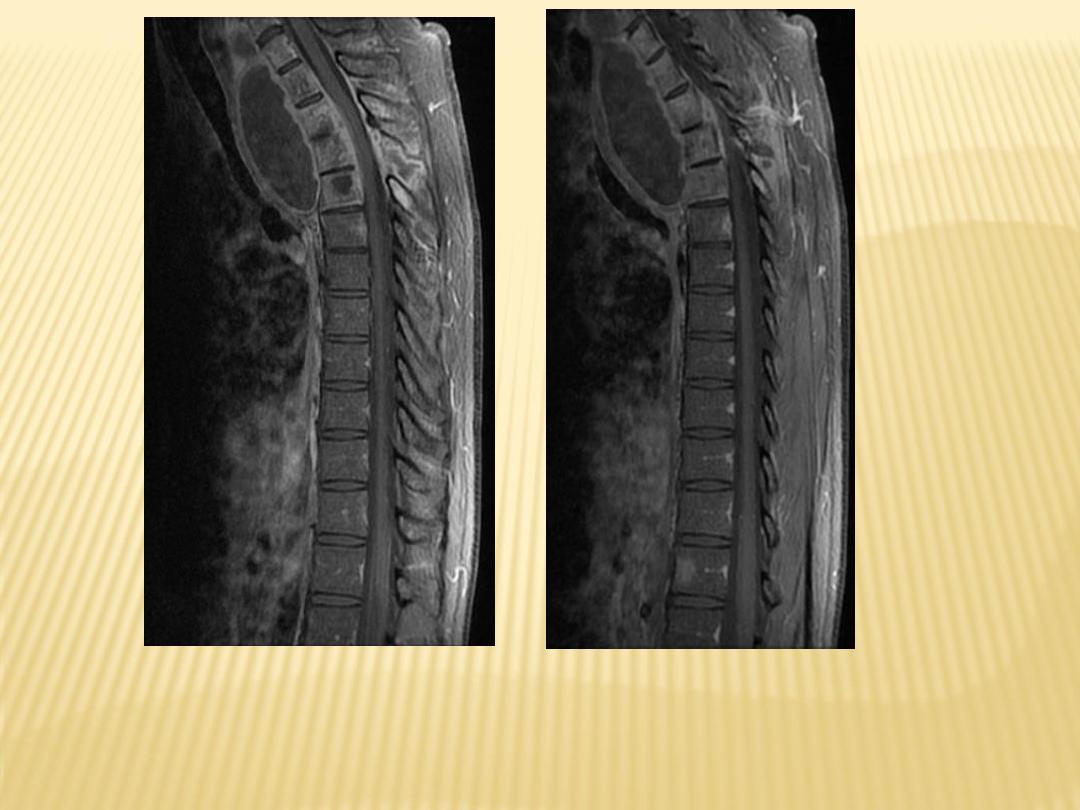
2-MRI
:
-Bone marrow hypointense on T1 +
hyperintense on T2 (water-rich
inflammatory tissue).
-Post contrast enhancement of
bone marrow, abscess margins,
periosteum and adjacent soft
tissue collections.
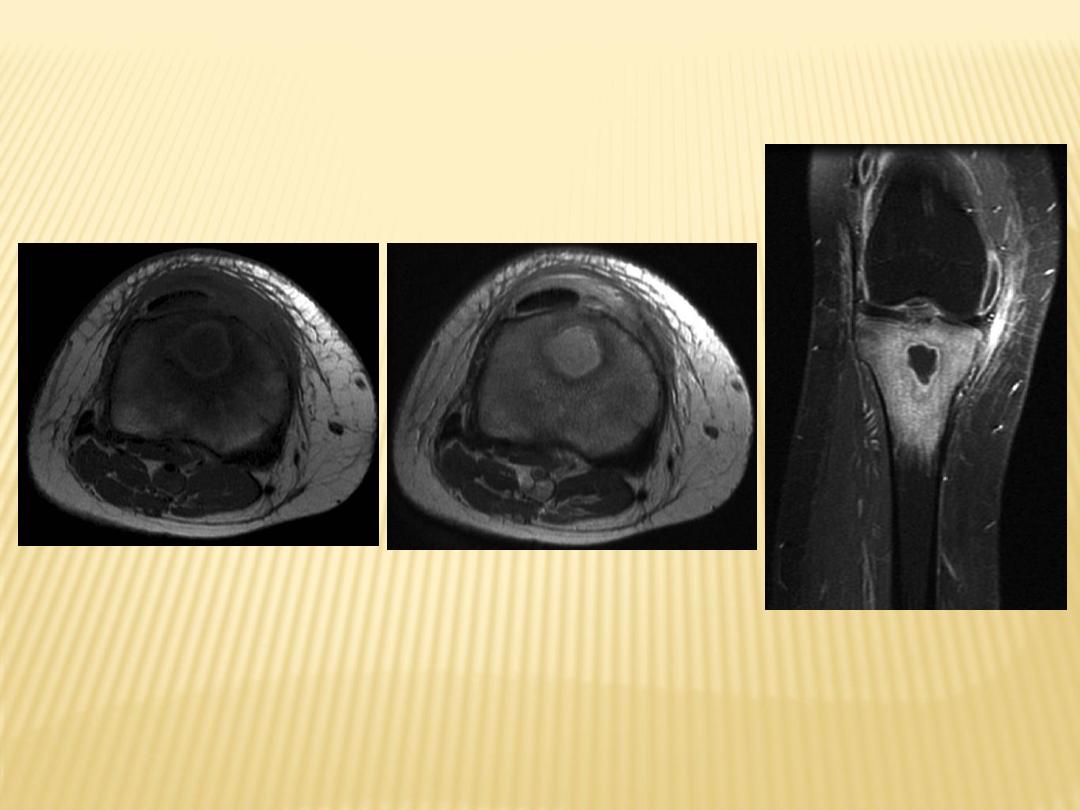
T1
T2
T1+C
1-Incidence
2-Radiographic Features
3-Differential Diagnosis
1-Incidence
:
-Also known as tuberculous
spondylitis
-Refers to vertebral body and
intervertebral disc involvement with
tuberculosis.
-N.B. :
Brucellosis can present as
granulomatous osteomyelitis of the
spine that can be difficult to
distinguish from TB.
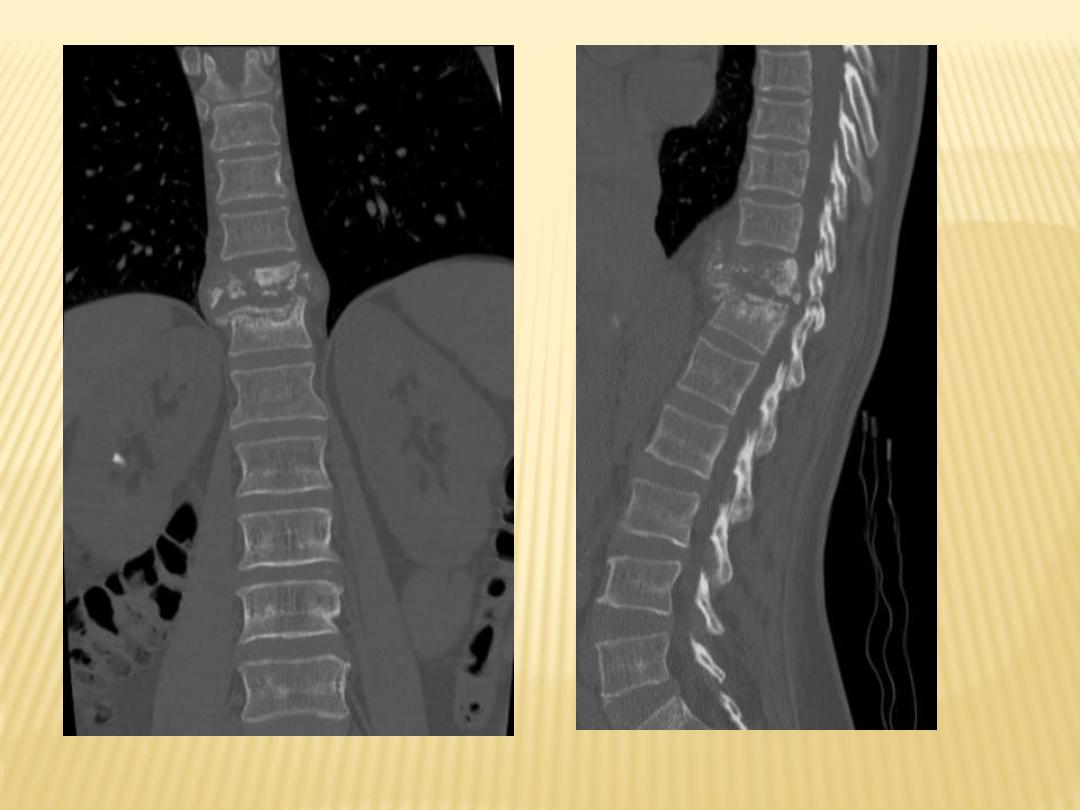
2-Radiographic Features :
1-Bone destruction
is prominent, more
prolonged onset than with pyogenic bone
destruction
2-Loss of disk height
, 80% (affects
intervertebral discs, but mets no)
3-Gibbus deformity
: anterior involvement
with normal posterior vertebral bodies
(Kyphosis)
4-Vertebra plana
or pancake vertebra
(vertebral body has lost almost its entire height
anteriorly and posteriorly)
5-Involvement of several adjacent vertebral
bodies
with disk destruction
6-Large paraspinous abscess
7-Extension into psoas muscles (psoas
abscess)

Destructive processes involving T11 associated with kyphosis
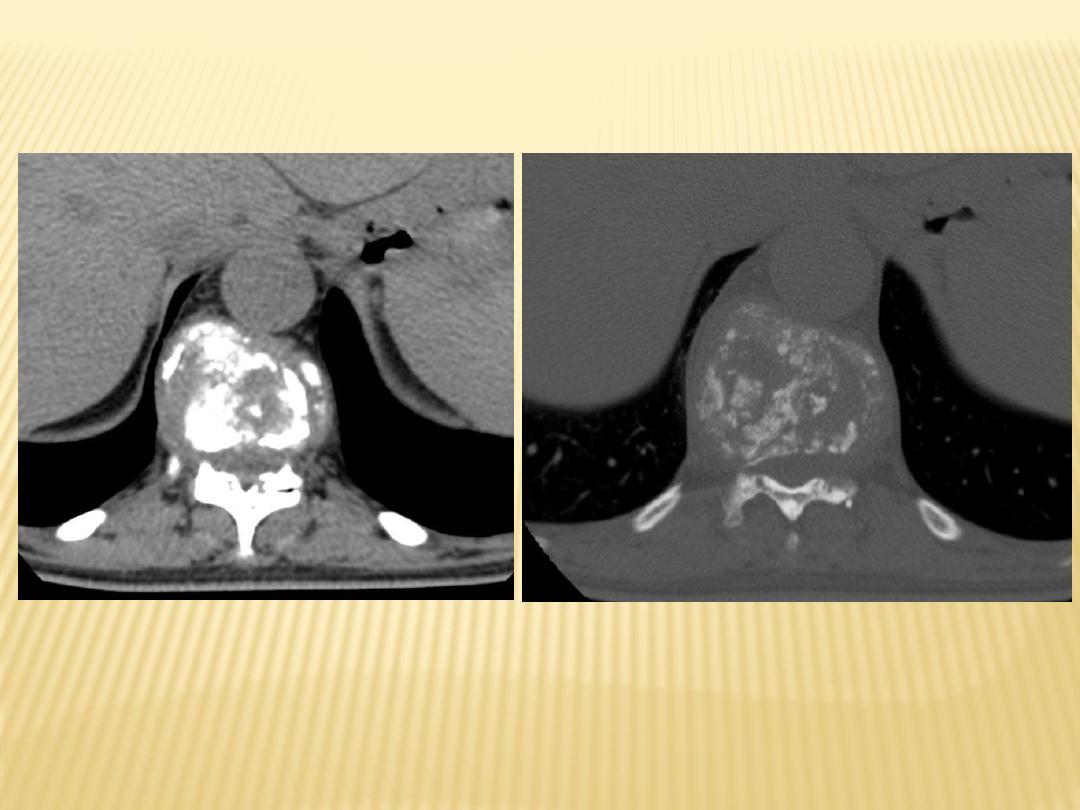

With paravertebral abscess

With paravertebral abscess
3-Differential Diagnosis :
-From non-specific infections :
a) Site :
-Lumbar vertebrae are more affected in non-specific
infections
-T.B. : Cervical , dorsal then lumbar
b) Course :
-Acute with non-specific and prolonged in T.B.
c) Soft tissue mass , collapsed vertebrae :
-More with T.B.
d) Sclerosis :
-More with non-specific infections
c) Congenital Infections : Celery stalking
1-Incidence
2-Radiographic Features
1-Incidence :
-Rubella, bone changes in 50% of
patients
-Syphilis, musculoskeletal involvement
is much more common, 95% of the
time
2-Radiographic Features :
-Celery stalking of metaphysis with
longitudinally aligned linear bands of
sclerosis.
-Periosteal reaction :
*
Absence in rubella
*
Prominent in syphilis
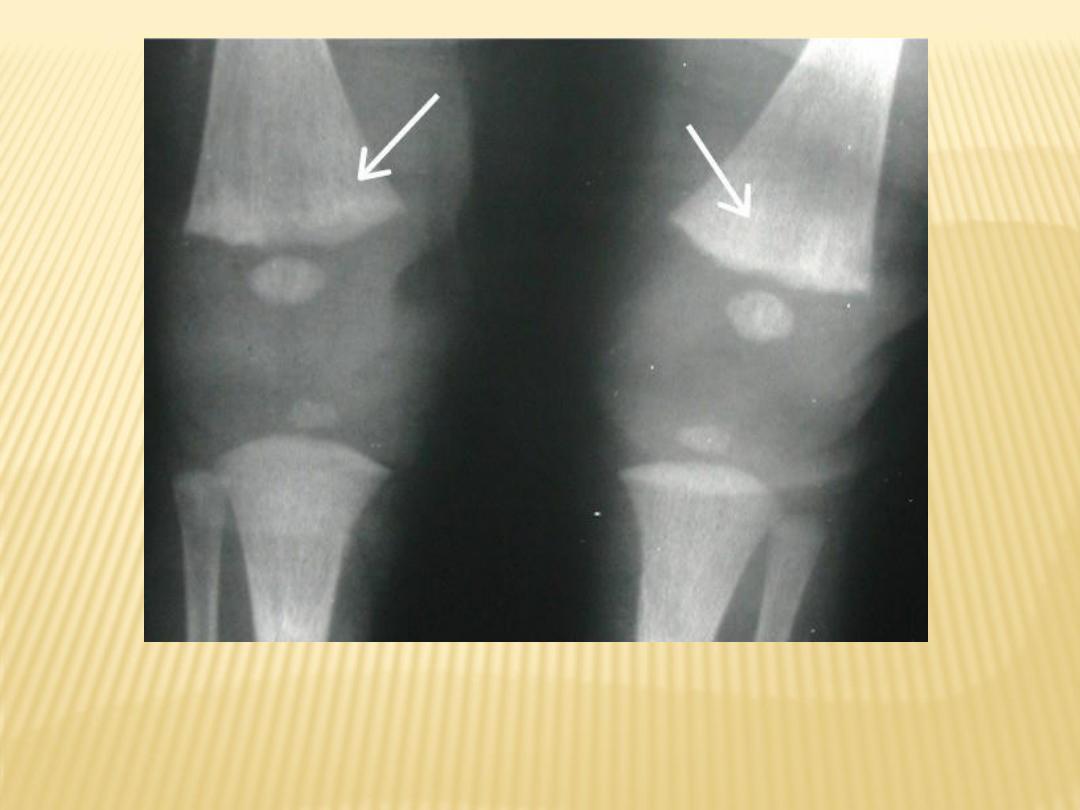
-
Rubella
: delayed appearance of
epiphyses.
-
Syphilis
: Wimberger's sign (bilateral
destructive lesion on medial aspect of
proximal tibial metaphysis)
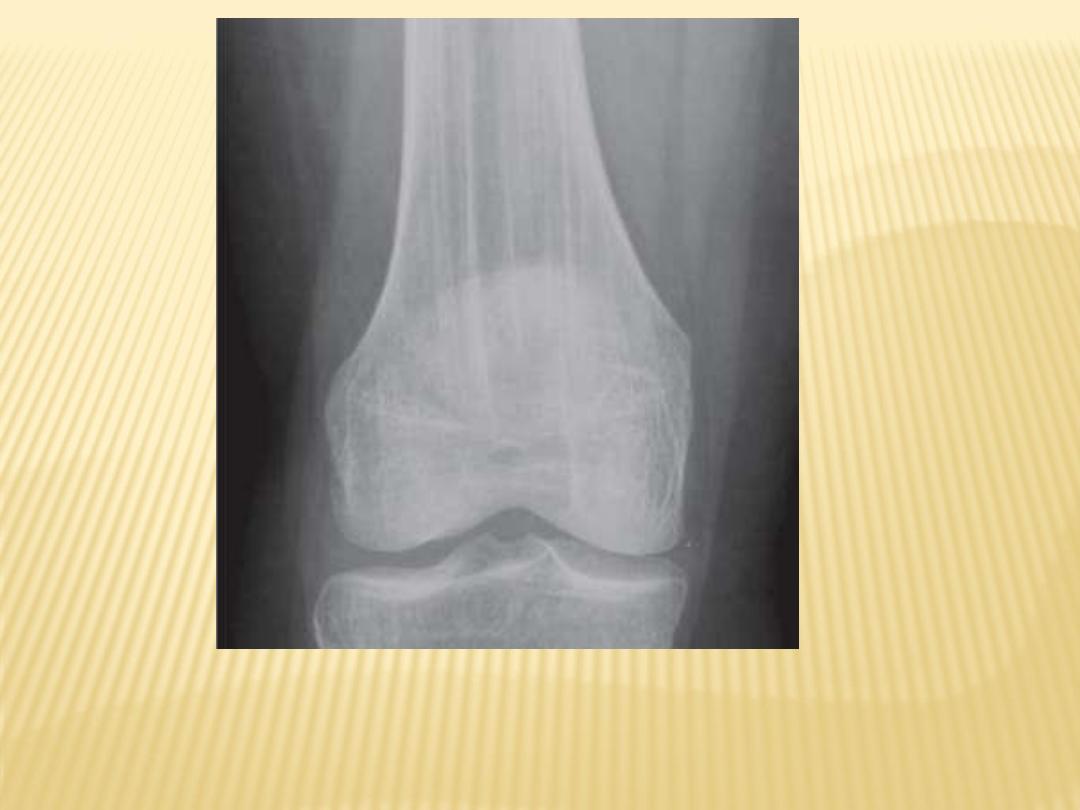
Celery stalking of metaphysis
Congenital rubella in a newborn male demonstrates
shows fraying and longitudinal alternating
radiolucent and radiodense stripes (celery stalking)
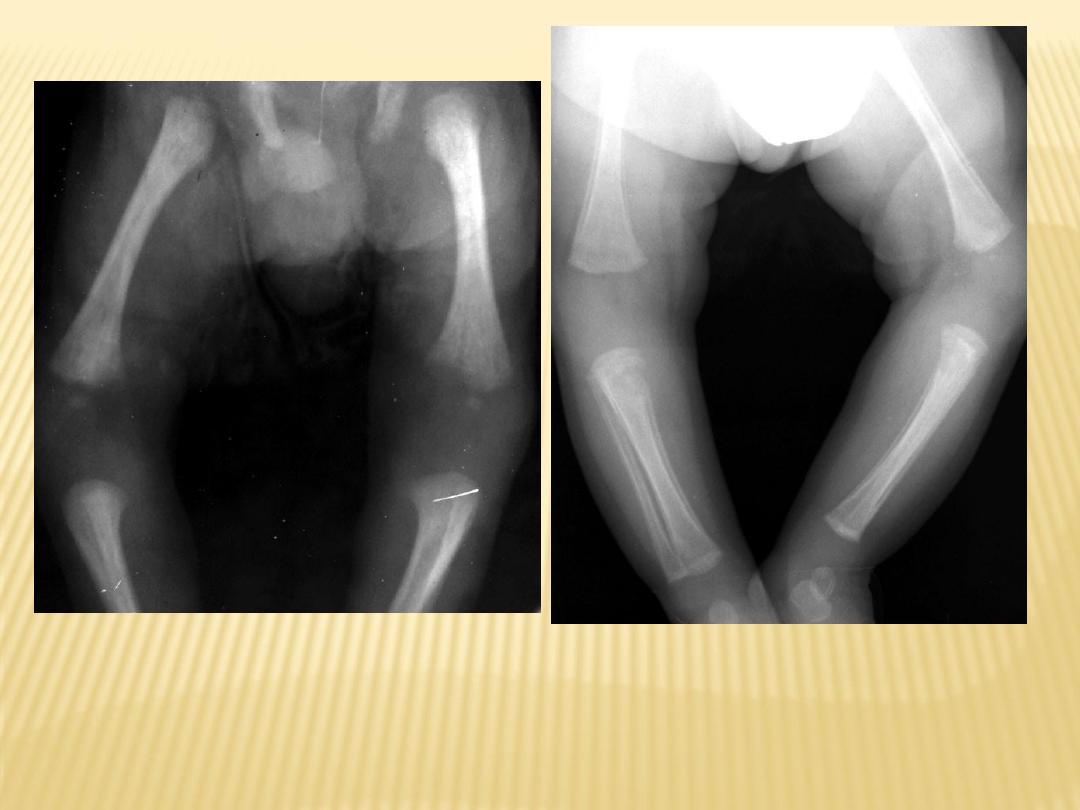
Congenital syphilis in a 2-month old female shows
marked periosteal reaction with destruction of the
proximal medial tibial metaphyses (Wimberger
corner sign).
Wimberger
’s sign
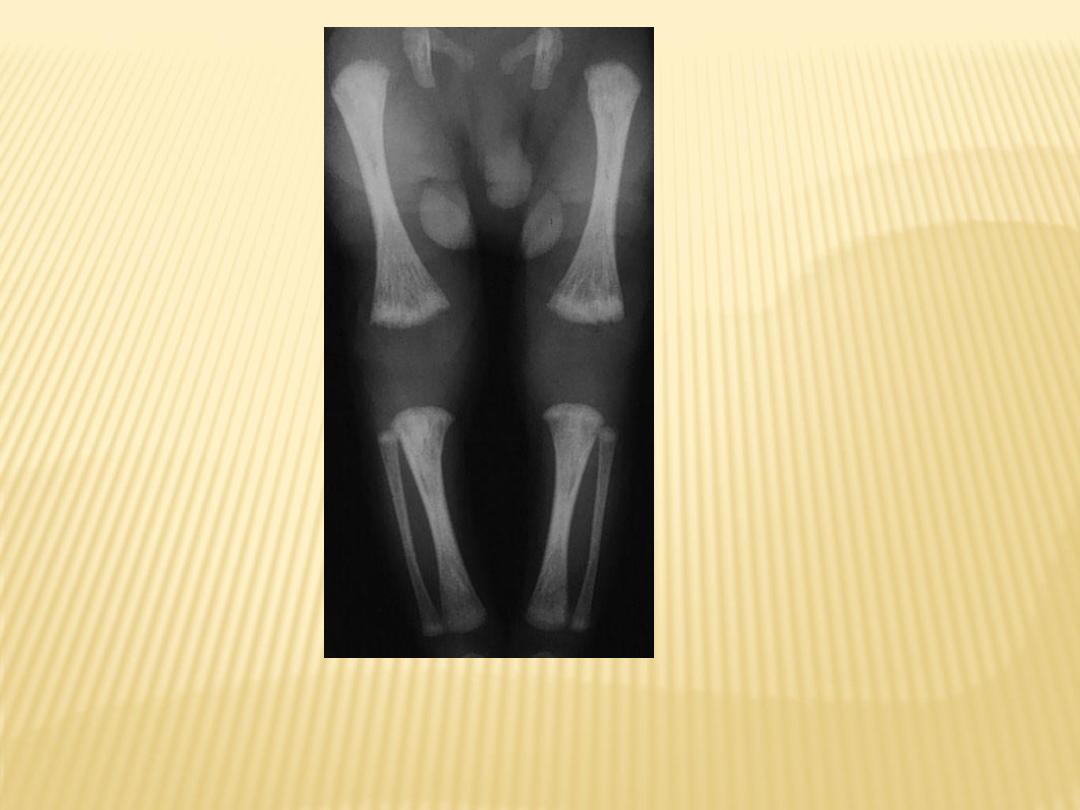
Celery stalking of metaphysis
Celery stalking of metaphysis
*N.B. :
Celery stalking of metaphysis is seen in :
1-Congenital infections
-Congenital rubella
-Congenital syphilis
-Congenital CMV
2-Osteopathia striata