Principles of fractures management
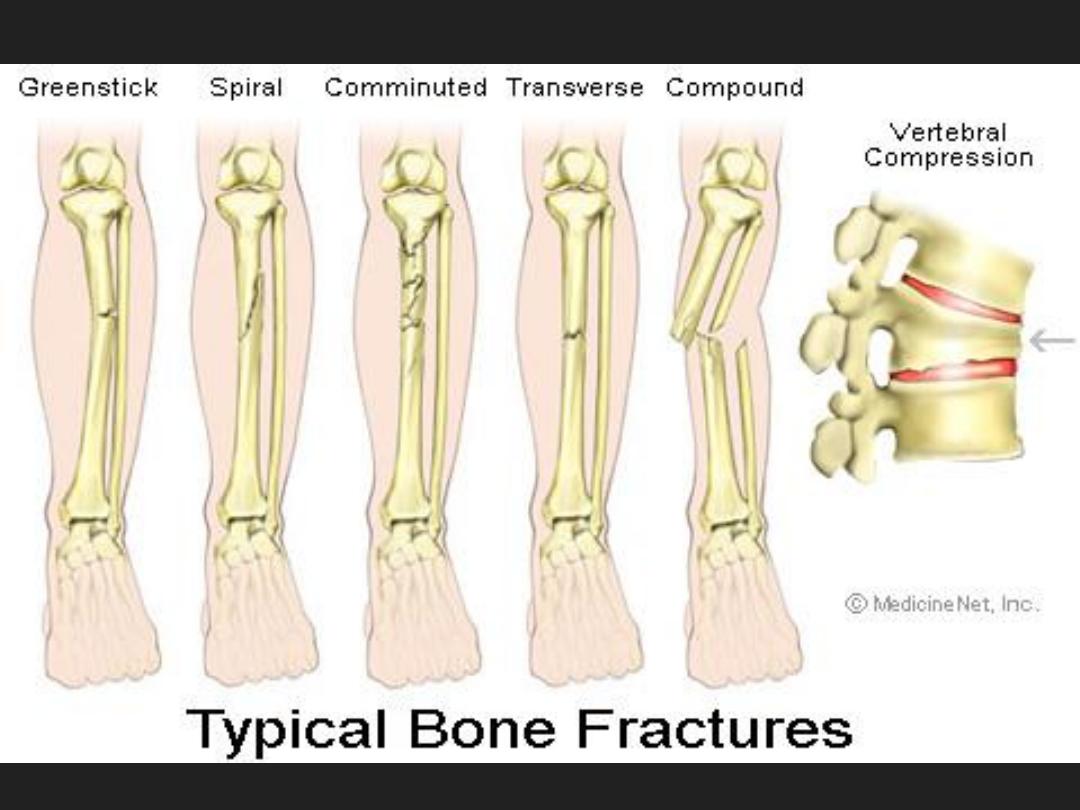
Fracture = break in structural continuity
of bone.
1-closed =
skin intact
2-compound =
fracture hematoma
connected to surface of skin or one of the
body cavities.
Compound fractures
classified according to Gustillo classification.
Gustillo classification:
G.
1
naht ssel:
1
cm wound
G.
2
> :
1
cm but Less than 10 cm wound
G
3
> :
10
cm wound with
G.3 A: adequate soft tissue coverage.
G.3 B: inadequate soft tissue covering.
G.3 C: neurovascular injuries
regardless the soft tissue covering
.

G 1

G2
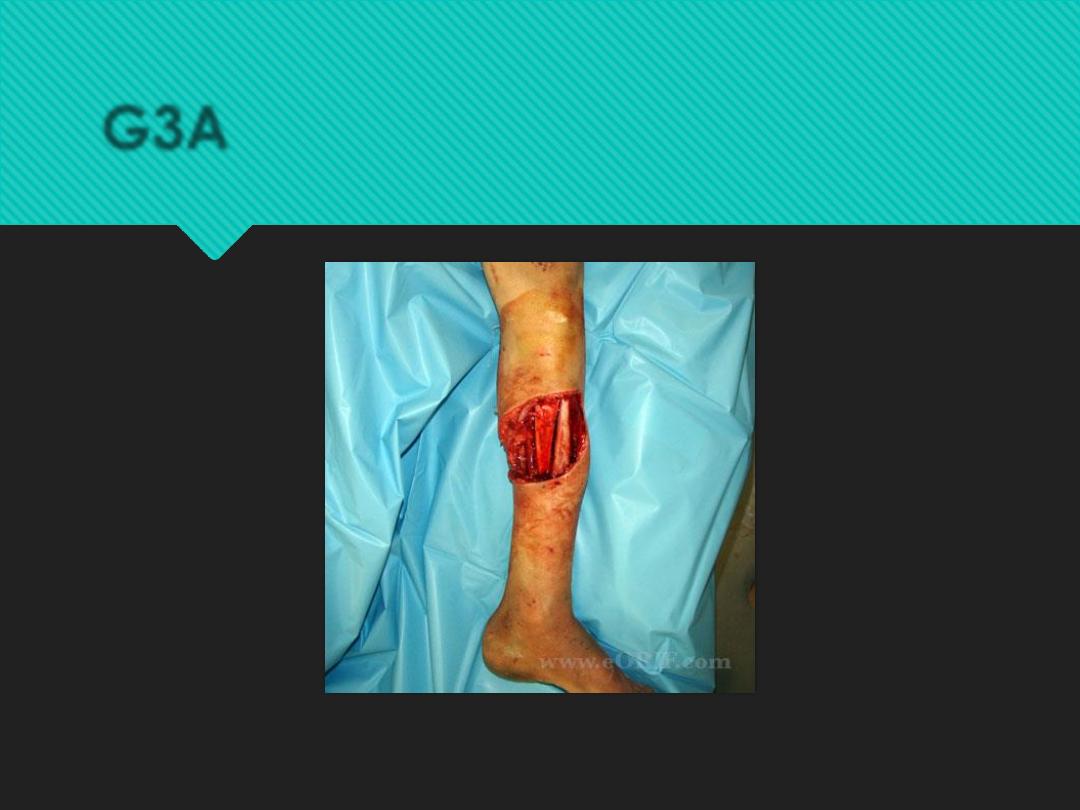
G3A

Gustillo fractures
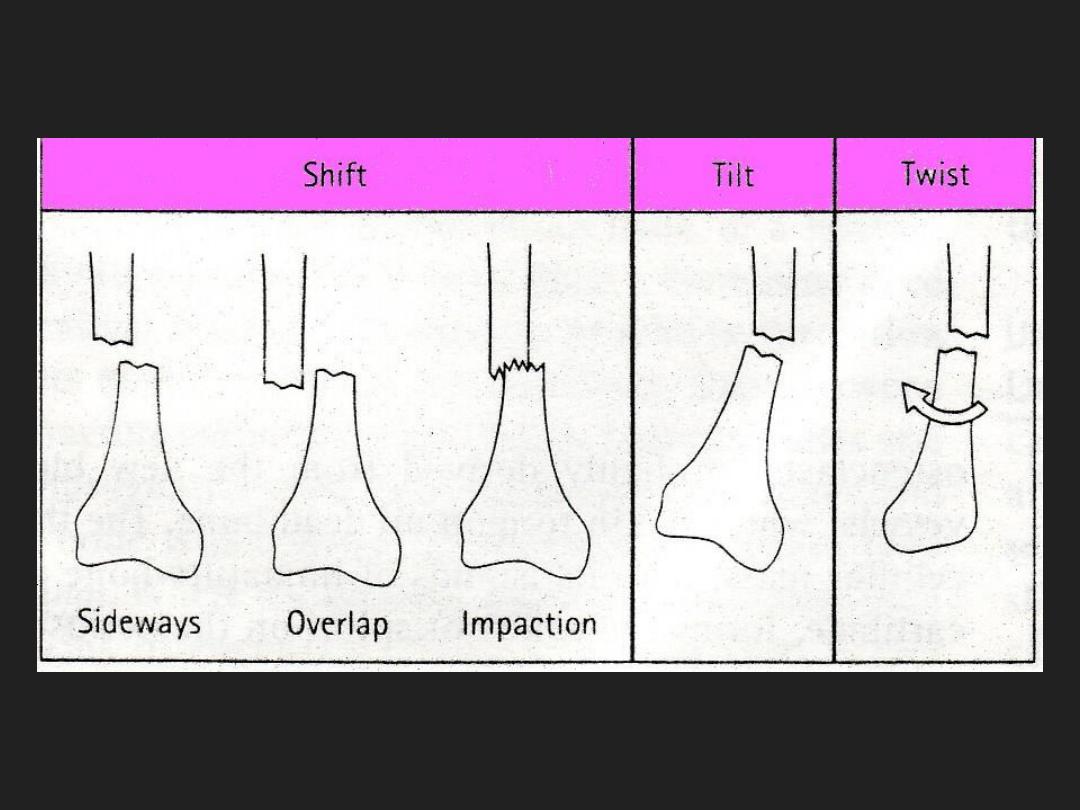
How fractures are displaced:
•
In complete fracture the bones
displaced by gravity or pull of muscles.
•
translation (shift)
•
alignment (angulation)
•
rotation (twist)
•
Overlap (shortening)
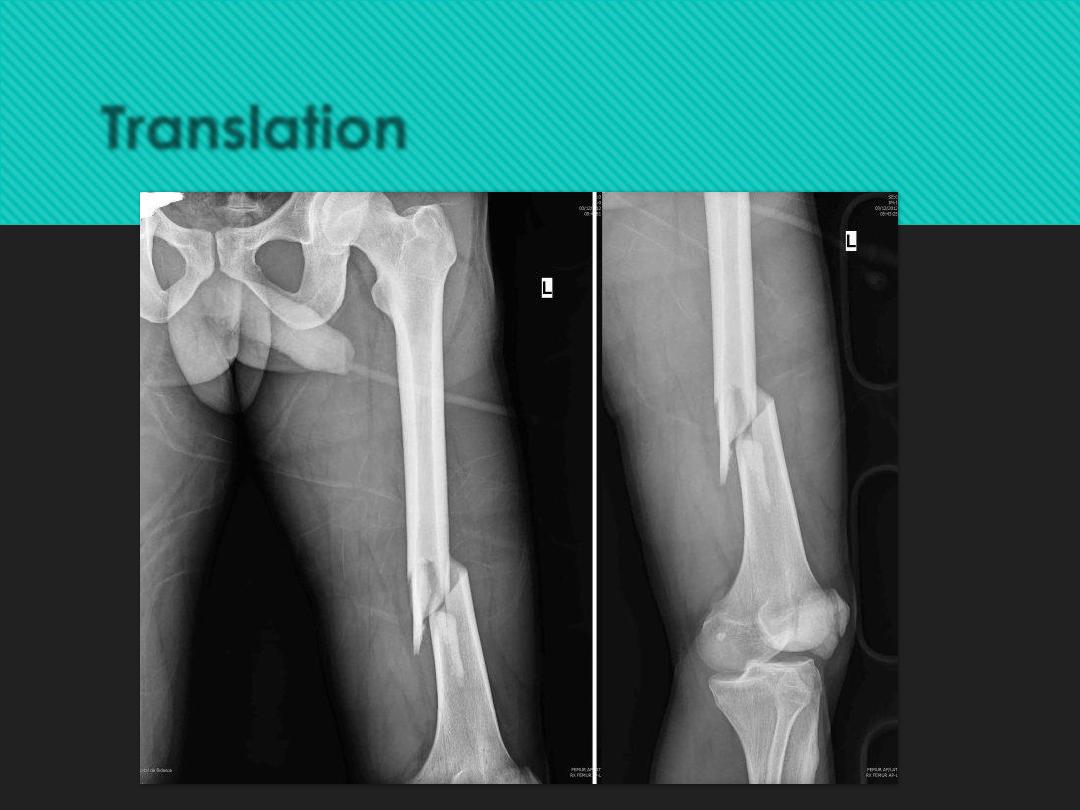
Translation
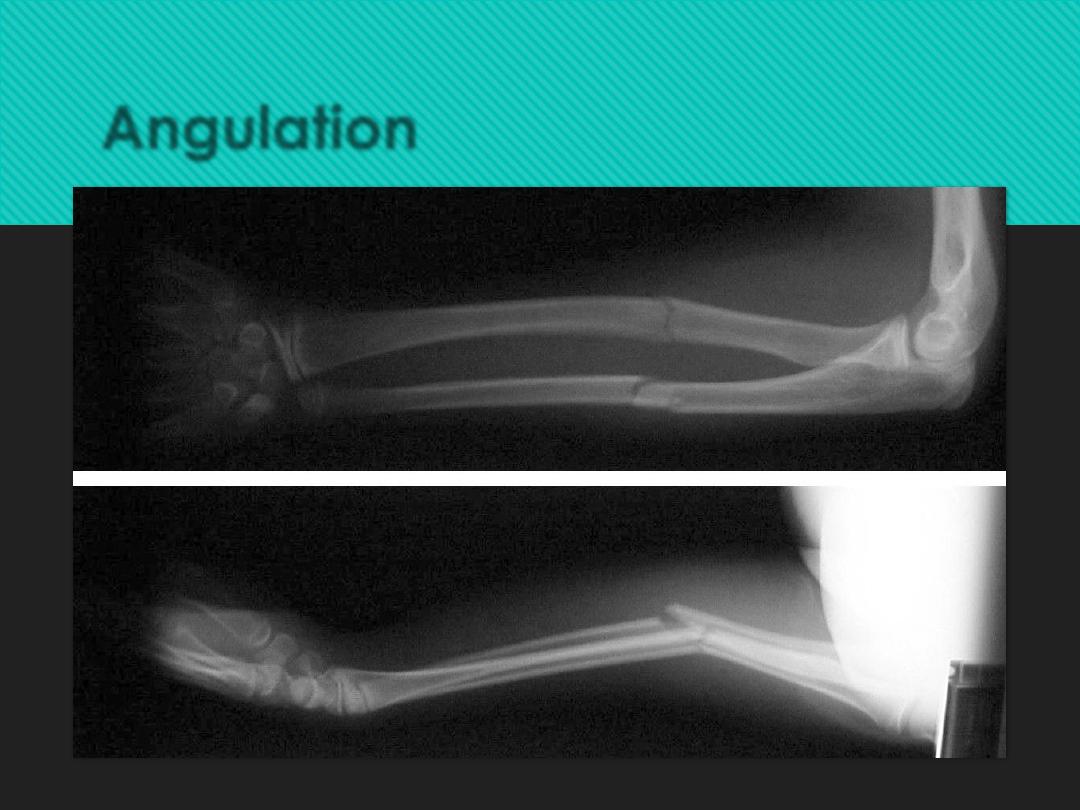
Angulation
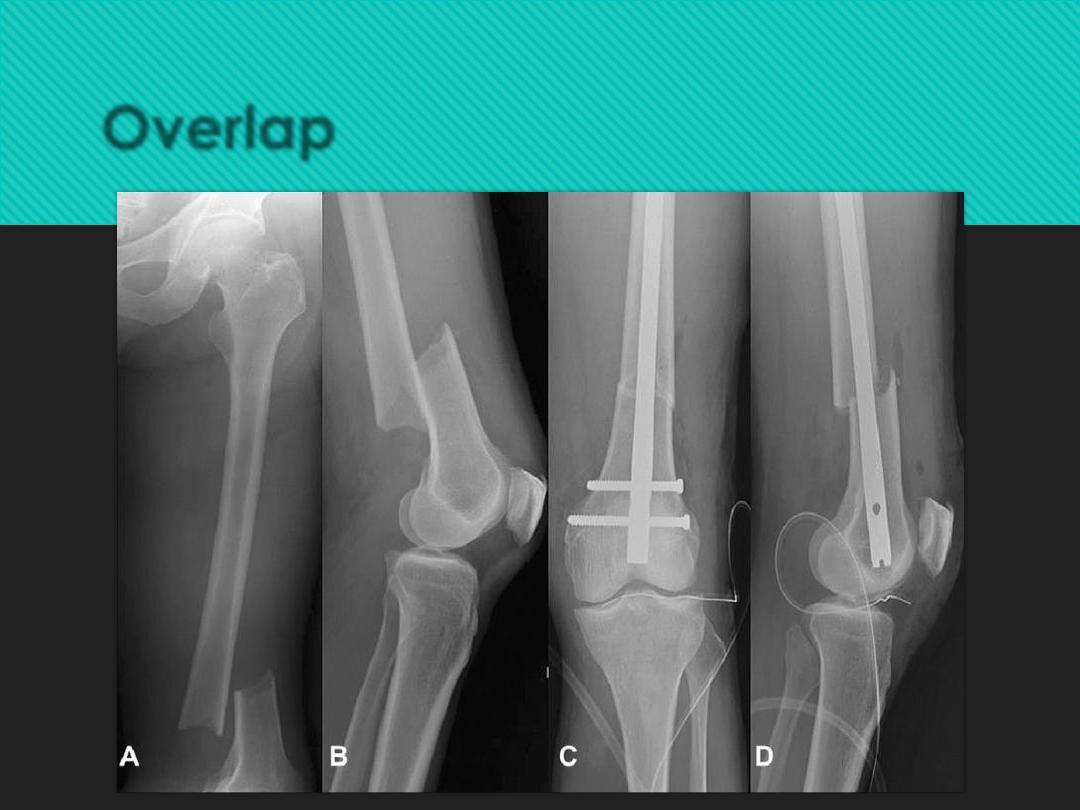
Overlap
X – Ray
The rule of two:
o
Two views anteroposterior and lateral views
o
Two joints joint above and below fracture included.
o
Two limbs as in children for comparison .
o
Two injuries sever injury cause injuries in more than one level.
o
Two occasions some not seen at the time of injury but only one or
two weeks later as in fracture scaphoid or stress fractures.
the upper limbs in children in general
3Wks
The lower limbs in children
Double the time i.e. 6 wks
The upper limbs in adults
Double the time needed in children i.e. 6
wks
The lower limbs in adults
Double the time needed in children
i.e. 12 wks
Fracture healing calendar
:
Treatment of closed fractures:
Three important rules:
1.
reduce
2.
hold
3.
exercise
Reduce:
•
Reduction aim
•
adequate apposition
•
acceptable alignment of the bone
fragments..
methods of reduction:
closed reduction:
•
under anesthesia or muscle relaxation
•
the distal part of the bone is pulled in line
of bone
•
disengaged – reverse mechanism of
injury – repositioned
open reduction: indications:
•
failure of closed reduction
•
displaced articular fractures
Hold
Immobilization is performed by:
1.
continuous traction
2.
cast splint
3.
functional brace
4.
internal fixation
5.
external fixation
Continuous Traction
problems
•
not accurate reduction
•
patient remain in bed for long period.
Two types ?
1.
skin traction: not more than 5 kg using adhesive
straps
2.
skeletal traction: pin inserted in the bone distal
to the fracture , this when high weight is
needed.
Skin traction application
Skeletal traction
Complication of traction:
1.
circulatory embarrasement. Especially
in children.
2.
nerve injury . in older people, drop foot
may happen
3.
pin-site infection.
Cast splint :
•
Plaster of Paris (POP)
•
Hold fractures after reduction
•
rotation of the fracture prevented by including the
joint above and the joint below,
•
The patient can leave the bed early in LL fractures
using of crutches allow ambulation
.
Pop casting
Closed reduction and POP casting
Complication of POP
1.
stiffness of joints 'fracture disease’ - avoide by
early physiotherapy.
2.
tight cast -- leading to compartment syndrome
3.
pressure sores over bony prominences ,
localized burn precisely over pressure spot.
4.
skin abrasion or laceration -- during removal.
5.
lose cast after swelling subside --- should be
replaced
.
Functional bracing
•
Using POP or plastic materials
•
cast are applied over the shaft of the bones
leaving the joints free,
•
cast segments connected by metal or plastic
hinges allowing movement in one plane.
•
Not rigid !!! applied only when the fracture is
beginning to unite
.
Functional brace
Internal fixation
1.
screws
2.
transfixing pins ,
3.
nails ,
4.
plate and screws
5.
intramedullary nail
6.
circumferential bands
Advantages
:
1.
allow early movement and prevent stiffness.
2.
allow early leaving of hospital.
3.
accurate reduction as in intraarticular fracture.
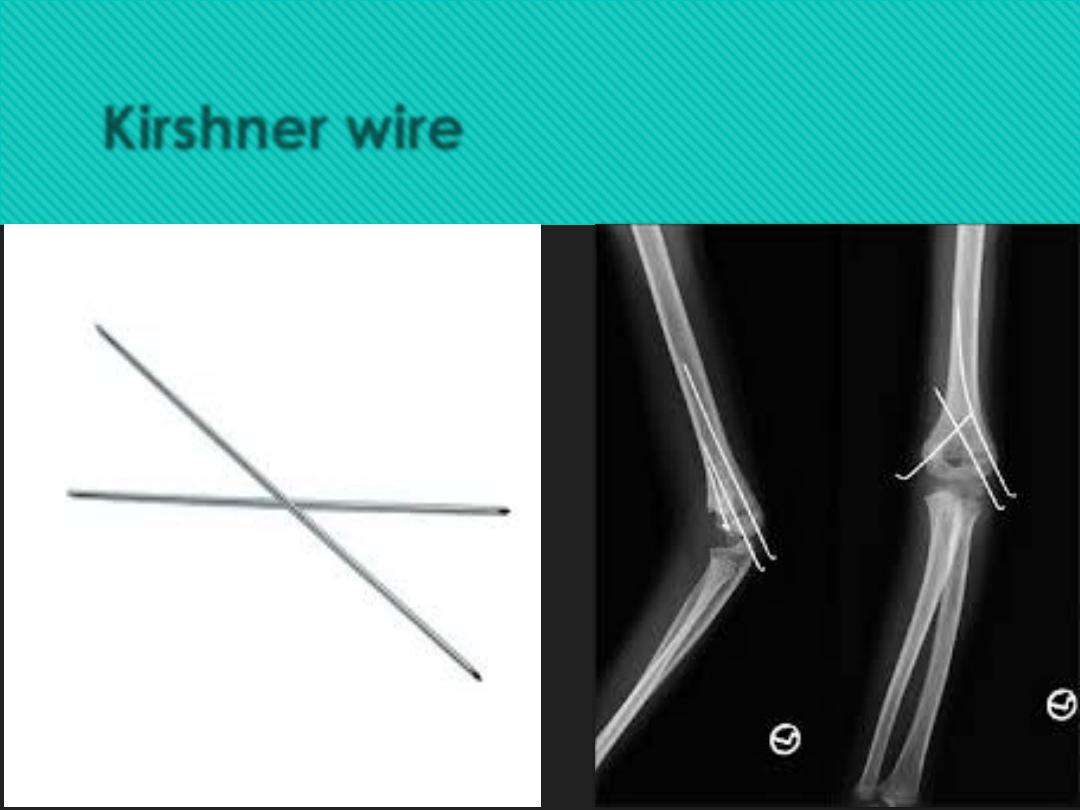
Kirshner wire
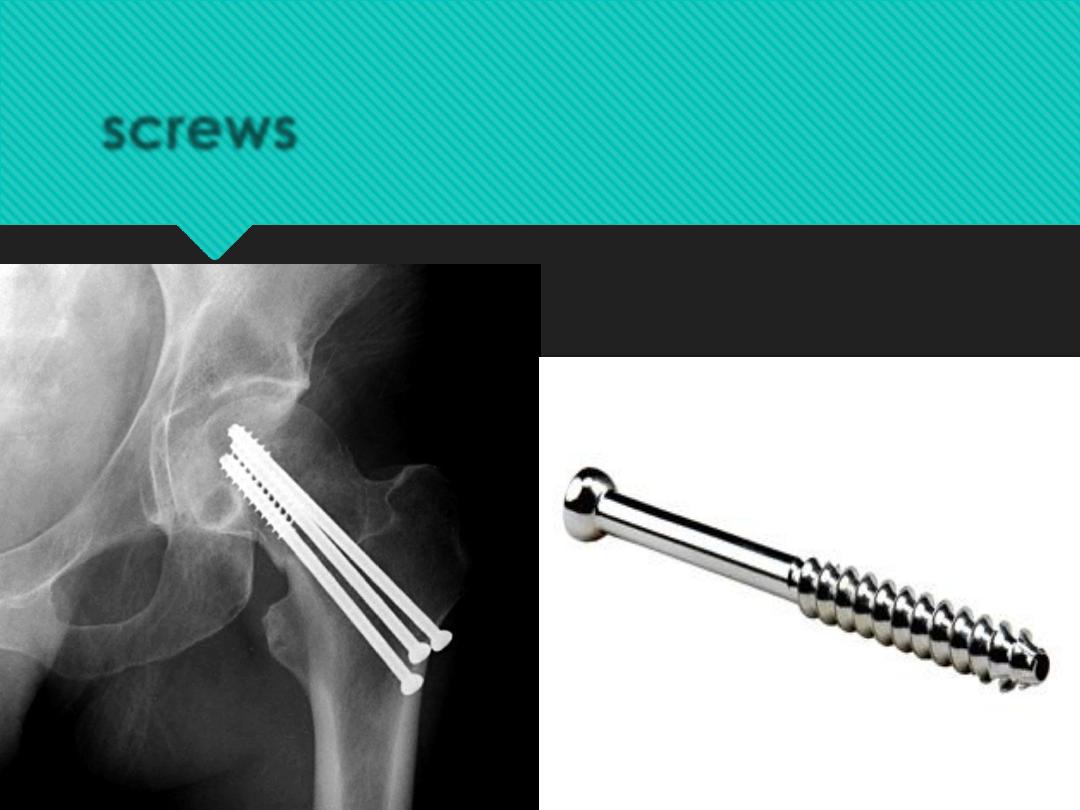
screws
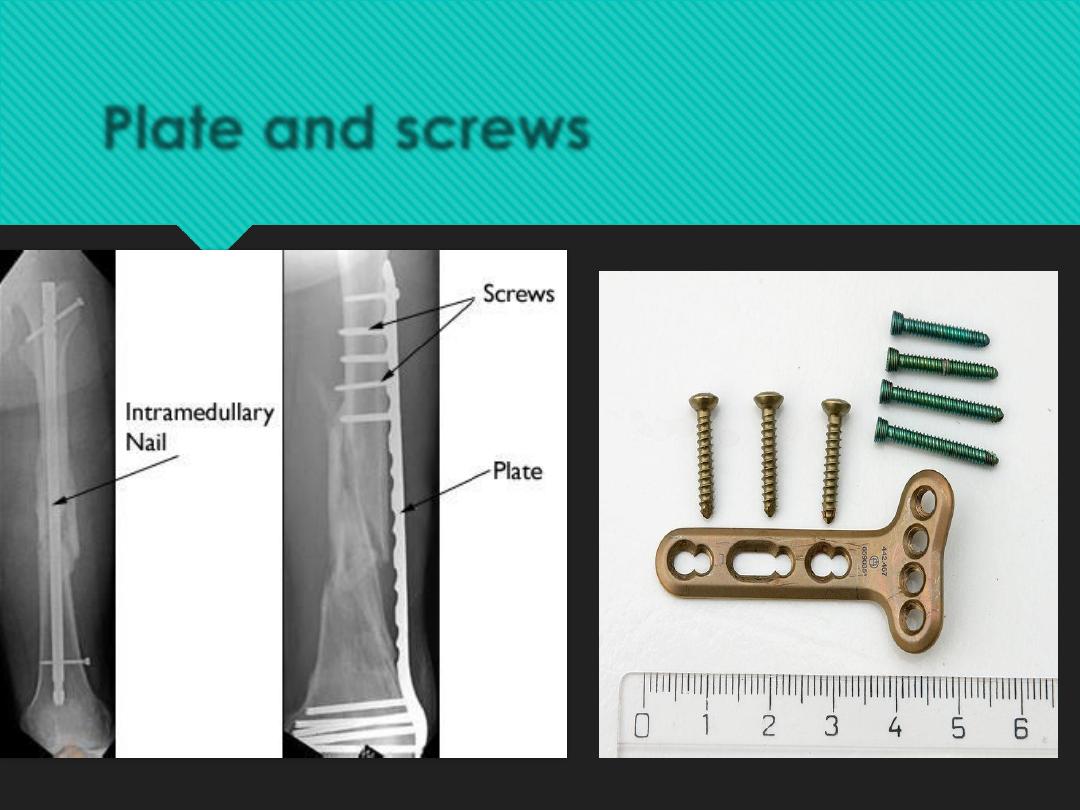
Plate and screws

Intramedullary nail
Indications of internal fixations
1.
failure of closed reduction.
2.
unstable fractures
3.
fractures that unite poorly as in fracture
neck femur.
4.
pathological fractures.
5.
multiple fractures.
6.
For nursing purpose as in paraplegics , and
multiple injuries
.
Complications
1.
Infection :
2.
Non – union: if bone ends fixed rigidly with a
gap between the ends.
3.
Implant failure.
4.
Refracture if the implant removed too soon
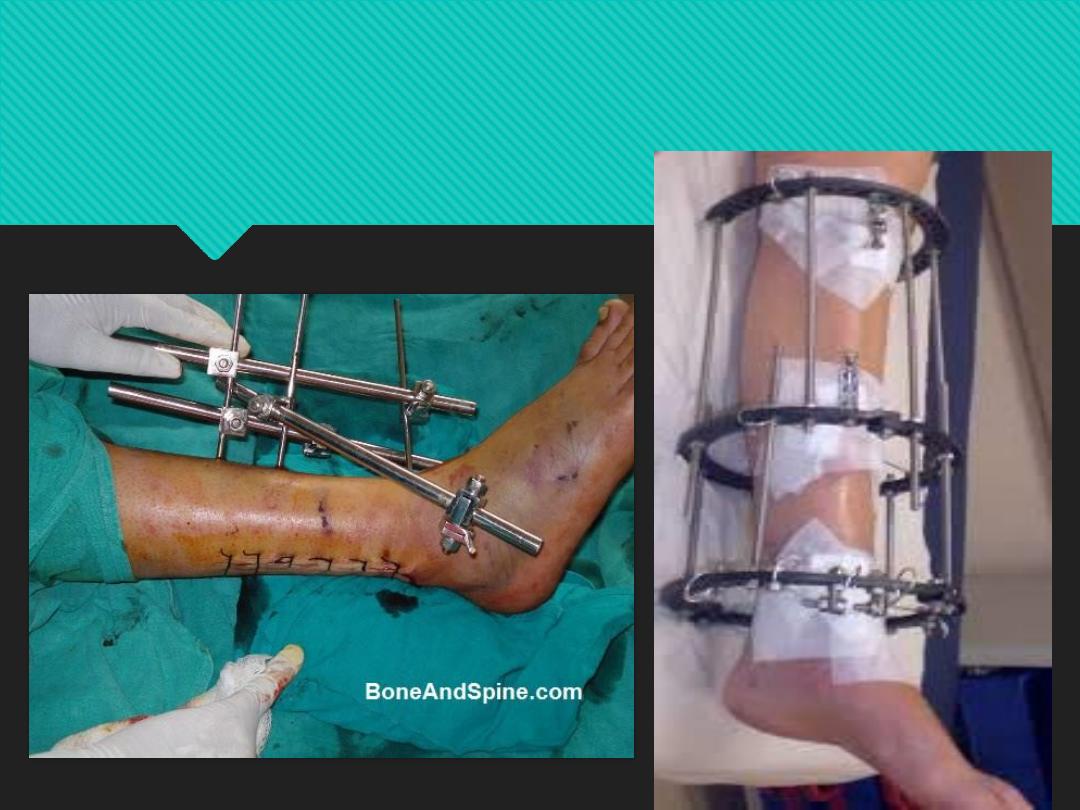
External fixation:
bone fixed below and above the fracture by pins or
tensioned wires and these connected to each other
by rigid bars.
Indications:
1.
Fractures with sever soft tissue damage.
2.
Fractures with sever nerve or vessels damage.
3.
Severely comminuted and unstable fractures.
4.
Non-uinited fractures .
5.
bone elongation.
6.
Pelvic fractures
7.
Infected fractures.
8.
Sever multiple injuries
.
Complications of EX FIX
1.
Damage to soft –injure nerves or vessels.
2.
Over distraction
3.
Pin – tract infection.