
Bone Tumors
•
A tumor is a lump or mass of tissue that divide uncontrollably.
•
Classification:
1.
primary bone tumor
.. Arise originally from the bone
•
benign or Malignant
•
in first 3 decades of life.
•
Benign tumors > malignant.
•
commonest sites around the knee , distal femur and
proximal tibia
2.
secondary bone tumor ..
•
metastasize to the bone form ( breast , prostate etc ..)
•
malignant transformation of benign lesions.
•
Most commonly noticed above the fifth decade of life
•
Histological classification based on dominant tissue:
Cell type
Benign
Malignant
Chondrogenic
Osteochondroma
Enchondroma
Chondroblastoma
Chondromyxoid fibroma
Chondrosarcoma
Osteogenic
Osteoid osteoma
Osteoblastoma
Osteosarcoma
Histocytic
Fibrous histiocytoma
Malignantf fibrous
histiocytoma
Fibrogenic
fibrous cortical defect(non-ossifying
fibroma), fibrous dysplasia, fibroma
Fibrosarcoma
Vascular
Hemangioma
Angiosarcoma
Others
Giant cell tumor, aneurismal bone
cyst, simple bone cyst
Malignant Giant cell
tumor

Clinical presentation:
History:
1.
asymptomatic
accidentally discovered on x-ray, more likely with
benign lesions.
2.
Pain:
it may be caused by:
1.
rapid expansion
2.
central hemorrhage.
3.
pathological fracture.
3.
Swelling or a lump.
4.
Neurological symptoms .. Compression by mass
5.
Pathological fracture

Examination :
•
Possible mass
•
Joint effusion and \or limitation of movemet
in tumor around joint
•
muscle spasm and back stiffness, or painful scoliosis
in case of .Spinal
lesions
•
Lymphadenopathy
should be checked
•
neurovascular check
for tumors in the limbs

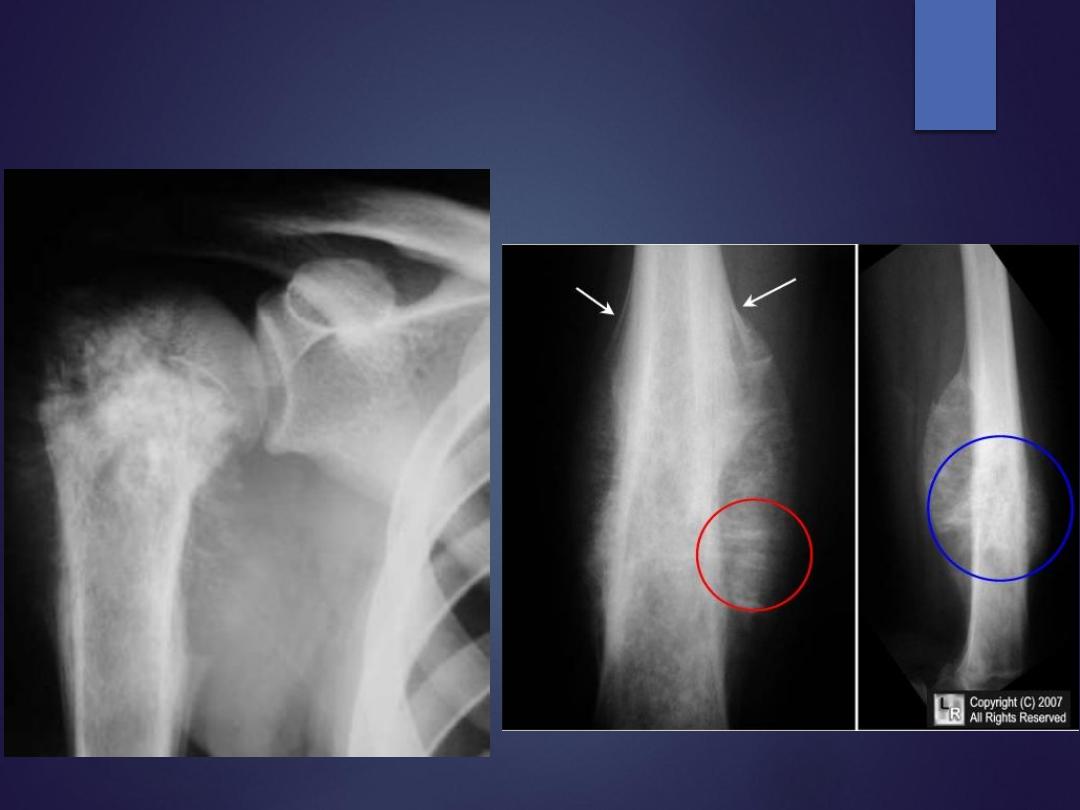
Imaging:
•
X-ray
:
check for
1.
Which bone is involved
2.
Where is the lesion in the bone? (epiphysis , metaphysis or
diaphysis.)
3.
lesion solitary or multiple?
4.
centric or eccentric.
5.
osteolytic or osteoblastic / is center calcified?
6.
margins of the lesion well- or ill-defined?
7.
Any cortical destruction?
8.
Any periosteal reaction?
9.
Any soft tissue extension

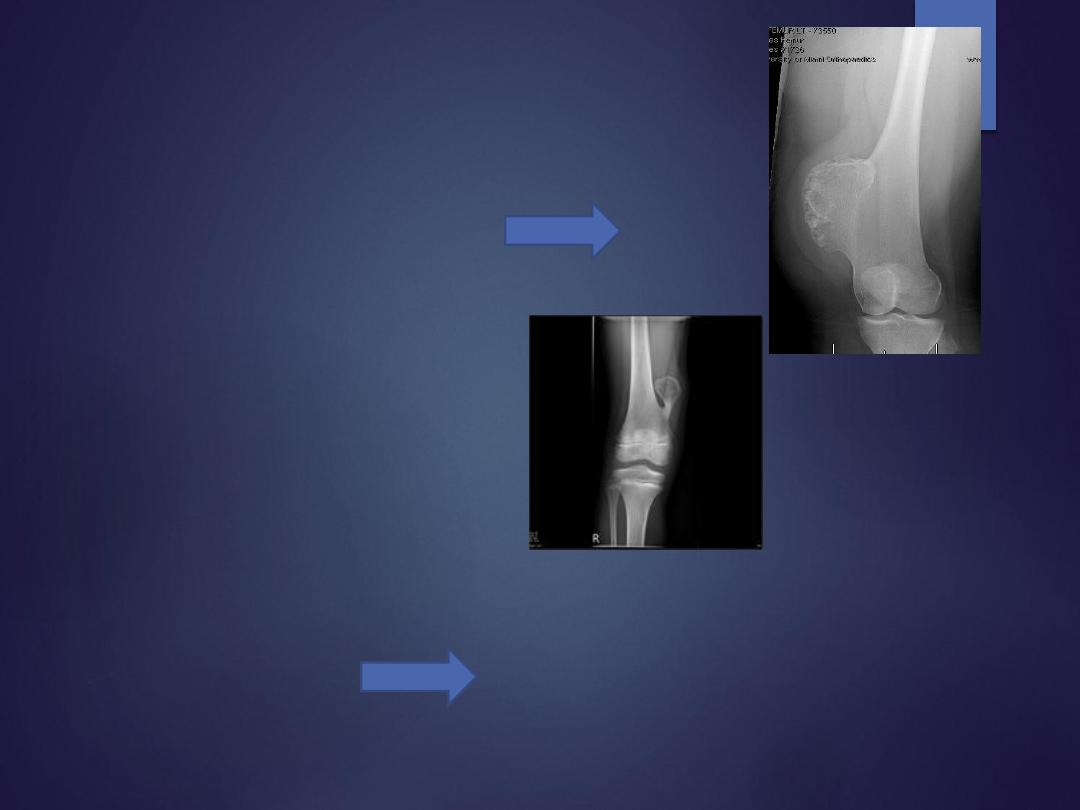
Benign bone lesion
malignant bone lesion

Other imaging:
•
Radioisotope scanning
: Helpful in metastatic and skip lesions.
•
CT & MRI
: can determine:
✓
The intra osseous and extra osseous extension of the tumor.
✓
Skip lesion in the same bone
✓
Lesions in inaccessible sites ,like the spine or pelvis.
✓
Pulmonary metastasis.
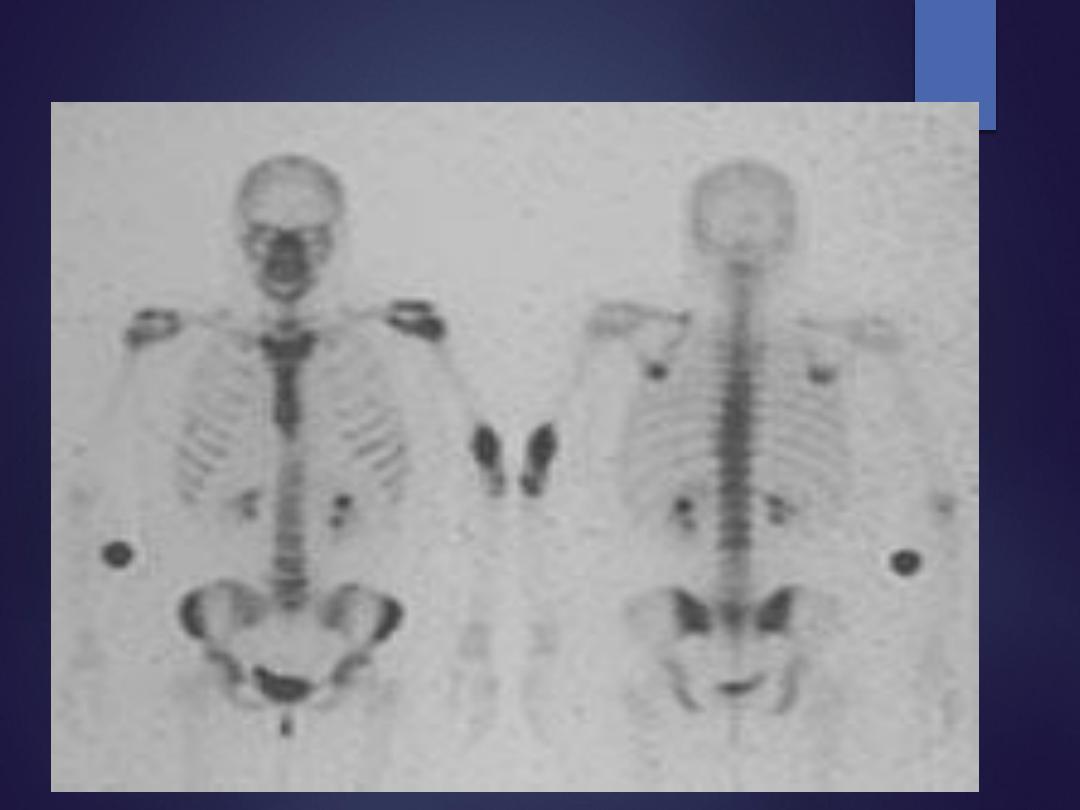
Bone Isotope Scan
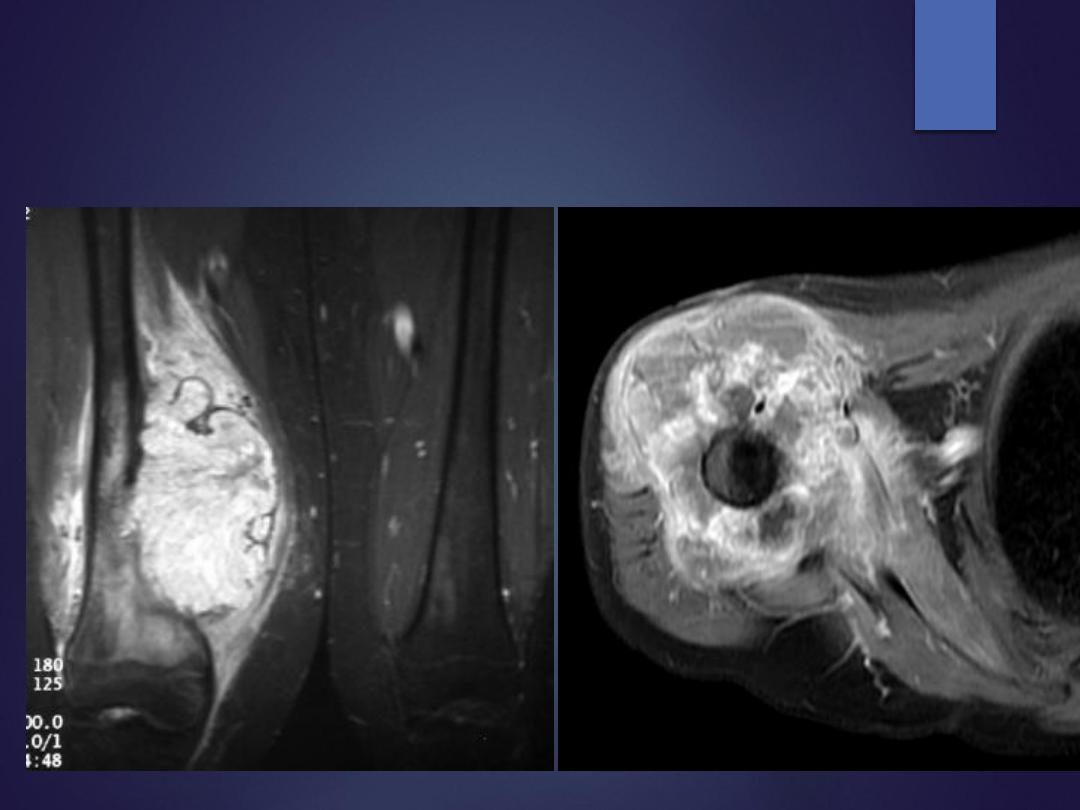
MRI

Lab. investigations
•
Blood tests to exclude other conditions e.g.
•
infection
•
metabolic bone disorders
•
“brown tumor” in hyperparathyroidism.
•
Serum and urine protein electrophoresis
•
for abnormal globulin and Bence-Jones protein in
myeloma.
•
serum acid phosphatase
•
for prostatic carcinoma.

Biopsy
•
for accurate diagnosis
two basic methods of doing a biopsy:
1.
Needle biopsy
•
under local anesthesia or GA using an X-ray or CT
guidance
•
value is in sampling inaccessible tumors.
2.
Open biopsy:
•
done through a small incision under general
anesthesia in an operating room.
•
Several samples should be taken
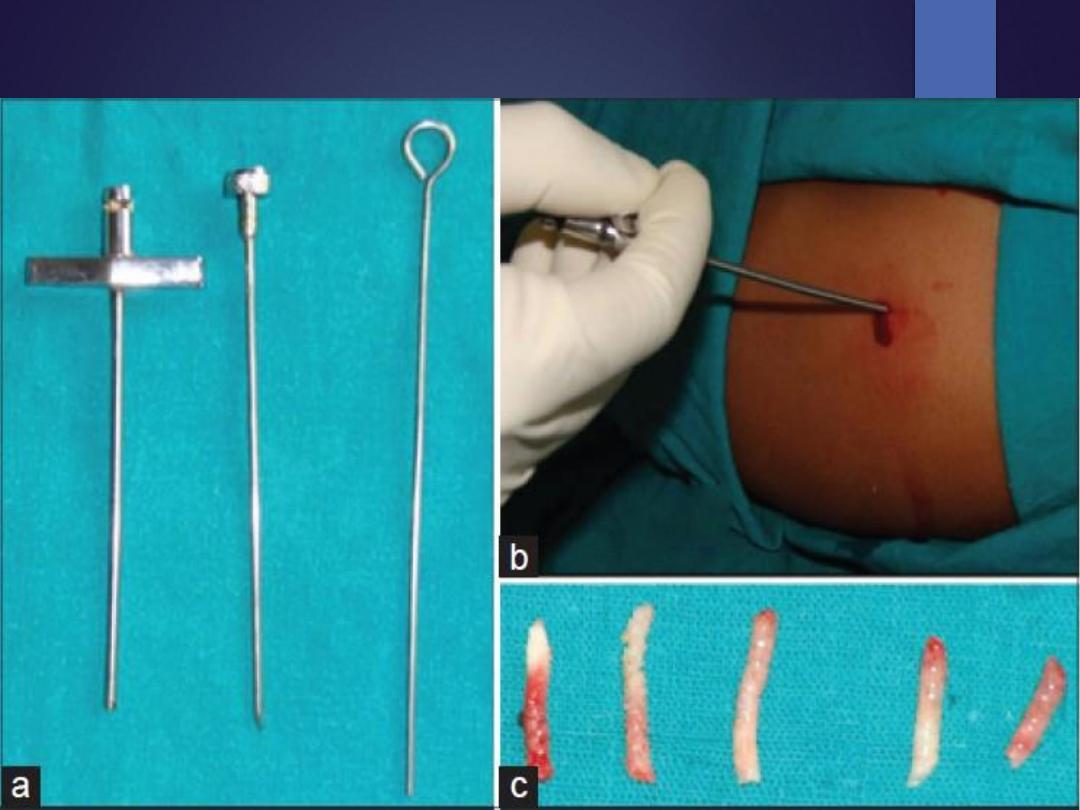
Needle biopsy


Differential Diagnosis
tumor mimicker
1.
myositis ossificans.
2.
stress fracture.
3.
bone infection.
4.
brown tumor of hyperparathyroidism.
Staging the lesion:
•
Enneking’s staging of benign lesion:
•
latent
•
active
•
aggressive
.
•
Enneking’s staging of malignant tumor:
Stage1
: low grade sarcomas
•
1A
: intracompartmental
•
1B:
extracompartmental
Stage 2
: high grade lesions.
•
2A
: intracompartmental
•
2B:
extracompartmental
Stage3:
sarcomas which have metastasized. e.g. to lung.

Management of
Primary Benign tumors:
•
Observation only / might disappear over time(e.g. fibrous cortical
defect, simple bone cyst)
•
Excision to reduce the risk of pathological fracture
•
Excision because its symptomatic / or have a risk of malignant
potentials like Giant cell tumor

Management of Primary Malignant tumors:
•
If the lesion is suspected to be a malignant tumor ,the patient is
admitted for
•
detailed examination
•
blood tests
•
CXR
•
pulmonary CT
•
biopsy.
•
Treatment goals include
•
Removing the tumor
•
preserving the function of the body .
Methods of treatment of malignant tumor
•
Tumor excision with wide excision or radical excision.
•
Limb-sparing surgery:
removes cancerous section of bone but keeps
nearby muscles, tendons, nerves and blood vessels . The excised bone is
replaced with a metallic implant (prosthesis) or bone transplant.
•
Amputation :
removes all or part of an arm or leg when the tumor is large
and/or nerves and blood vessels are involved.
•
Radiotherapy
: uses high-dose X-rays.
•
Shrinks the tumors
•
suitable for inaccessible sites
•
Multi-agent chemotherapy
: neoadjuvant for malignant bone tumors

Benign Bone Tumors

Osteochondroma
the most common benign bone tumor
•
common locations include
•
knee (proximal tibia, distal femur)
•
proximal femur
•
proximal humerus
•
Can be either
1.
solitary ostoechondroma
2.
Multiple Hereditary Exostosis (MHE)
•
Clinical presentation
•
Asymptomatic / painless mass
•
mechanical symptoms
•
symptoms of neurovascular compression
Osteochondroma
•
Radiograph
•
sessile (broad base) or
•
pedunculated
•
Treatment
•
Observation alone .. If Asymptomatic
•
Operative .. If symptomatic or growing fast

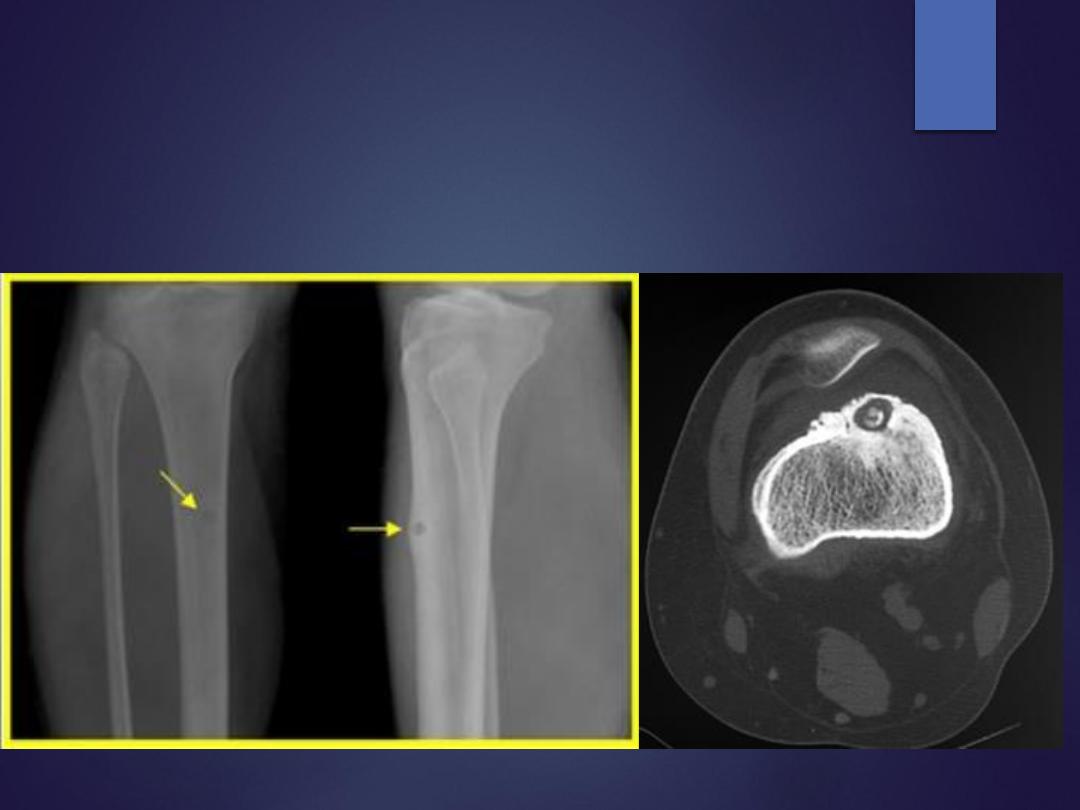
Osteoid osteoma
•
A small, discrete, painful, benign bone lesion
•
Commonest location
•
proximal femur > tibia diaphysis
•
usually within bone cortex
•
Spine .. Produce scoliosis
•
Characterized by central nidus with surrounding sclerotic rim
•
Pain is constant at night and relived with NSAIDS
•
Radiographs
•
reactive bone around radiolucent nidus
•
CT imaging is the study of choice
Osteoid osteoma

Osteoid osteoma
Management
•
clinical observation and NSAID administration
•
percutaneous radiofrequency ablation
•
surgical resection/curettage
•
complete marginal resection of nidus (sclerotic bone is normal and
can be left behind)
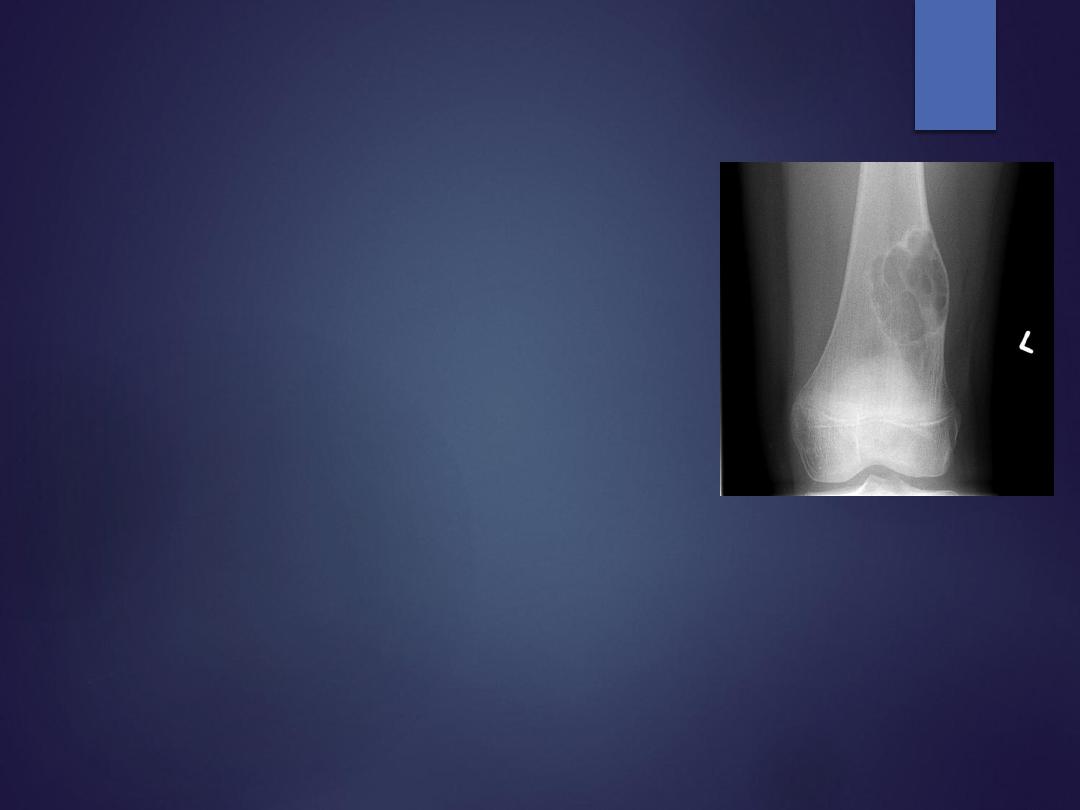
Non-ossifying Fibroma
•
fibrogenic lesion /dysfunctional ossification
•
Locations … metaphysis of long bones
•
Symptoms
•
asymptomatic found incidentally
•
Or pathologic fracture
•
Radiographs is diagnostic
•
metaphyseal cortical eccentric "bubbly" lytic lesion surrounded by
sclerotic rim
•
Treatment
•
observation .. most resolve spontaneously
•
curettage and bone grafting .. If symptomatic or at risk of fracture

Unicameral bone cyst
simple bone cyst
•
A non-neoplastic, serous fluid-filled bone lesion / failure of bone
formation
•
usually found in the metaphysis of long bones in young patients <20 years
•
found in the
•
proximal humerus
•
Proximal femur
•
Distal tibia and radius
•
Symptoms
•
most asymptomatic unless fracture occurs (usually with minor trauma)
•
pathologic fracture in ~50%
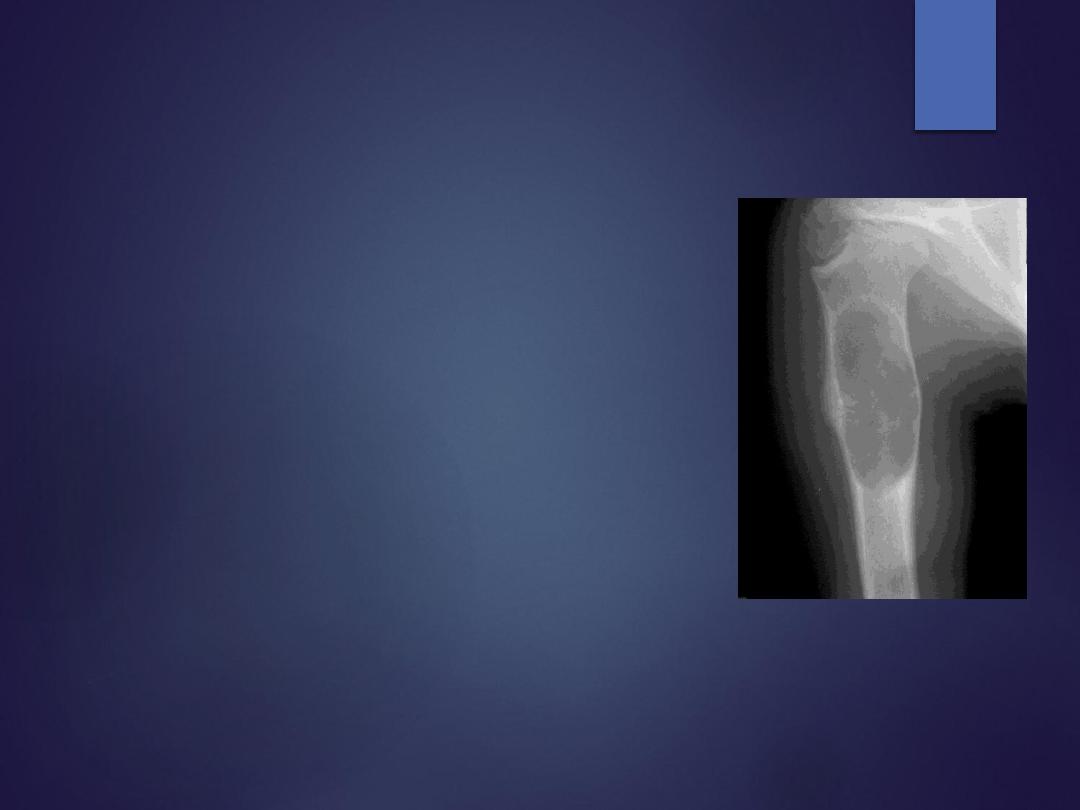
Unicameral bone cyst (simple bone cyst)
•
Radiographs
•
central, lytic, well-demarcated metaphyseal lesion
•
thinning of cortices
•
Treatment
•
Observation if at low risk of fracture
•
aspiration/methylprednisolone injection
•
curettage and bone grafting +/- internal fixation based on tumor
location

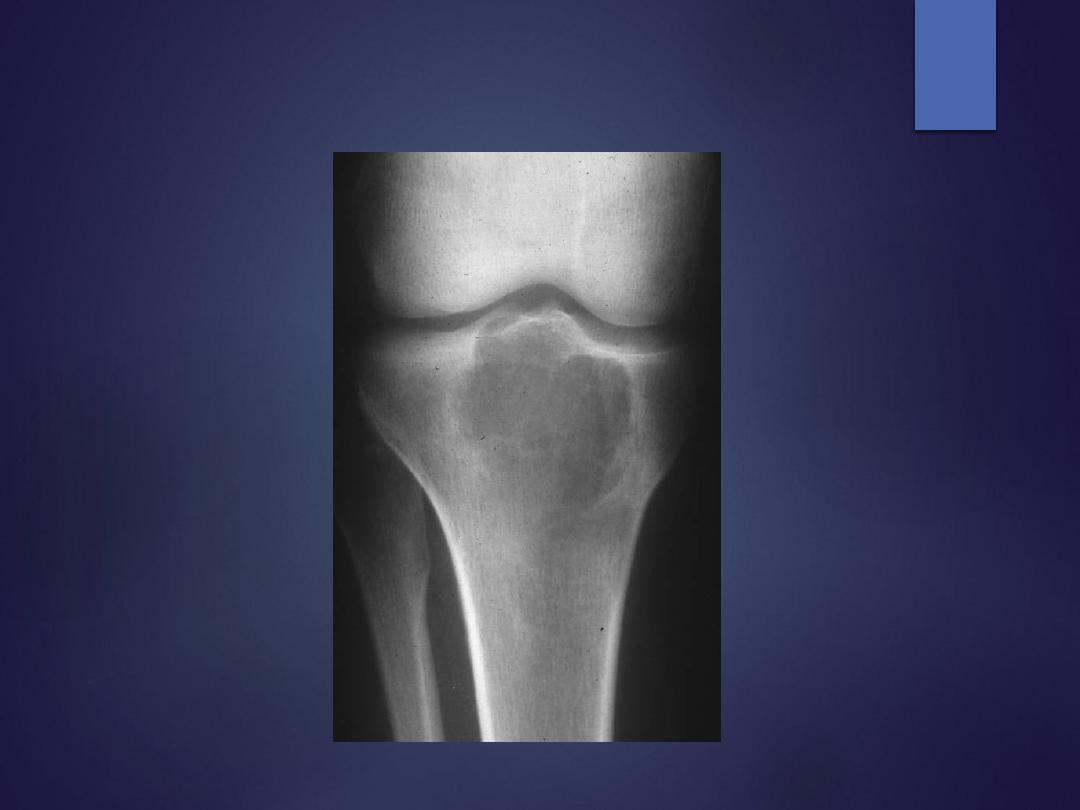
Giant cell tumor
•
A
benign
aggressive tumor found in the metaphysis of long bones in
mature
adults
•
distal femur > proximal tibia > distal radius
•
Clinical features
•
pain in the involved joint
•
palpable mass
•
Radiograph
eccentric lytic epiphyseal/metaphyseal lesion extends subchondral bone
•
Chest radiograph or chest CT .. 5% pulmonary metastsasis
•
Bone scan is very hot
•
MRI ,… signal change
Giant cell tumor

Giant cell tumor
Treatment
•
medical management ??? New modality ..
•
bisphosphonates
•
denosumab
•
Operative
•
extensive curettage and reconstruction (with adjuvant treatment)
•
10-30% recurrence with curettage alone verses 3% with adjuvant
treatment (phenol , hydrogen peroxide , argon llaser ..)

Malignant Bone Tumors

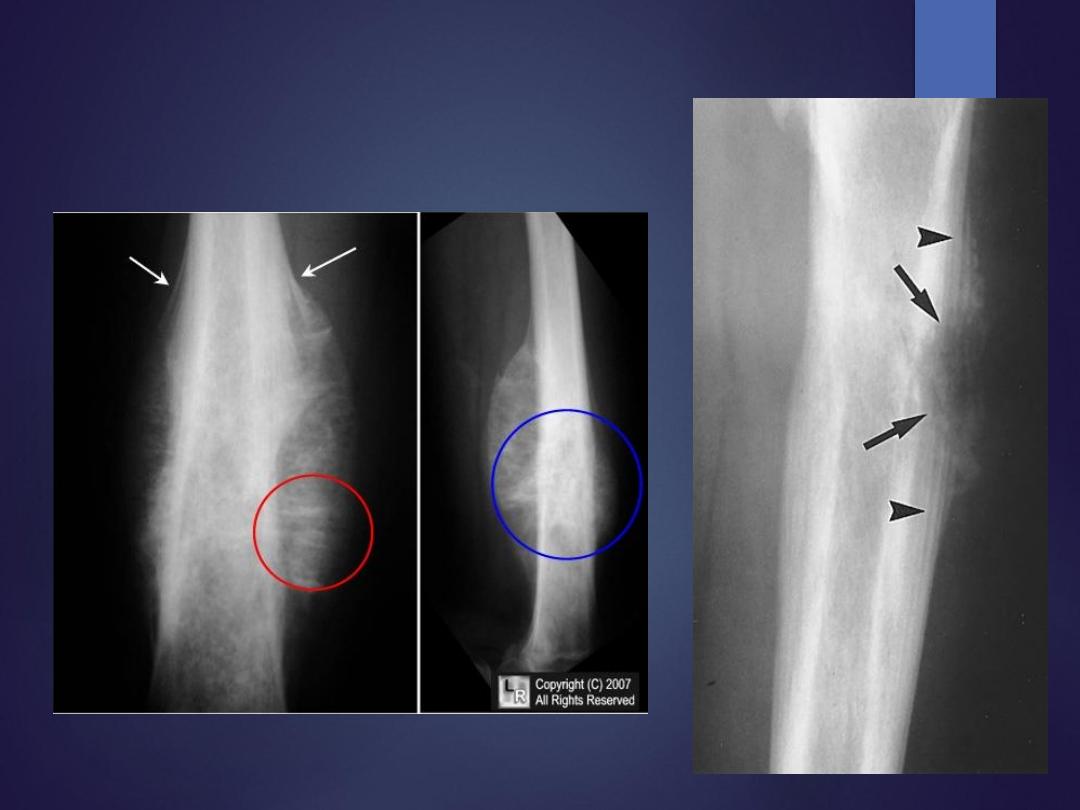
Osteosarcoma
•
the most common primary sarcoma of bone
•
in children and young adults <25 years
•
common site / distal femur & proximal tibia
•
commonly diagnosed at Stage IIB (high grade, extra-
compartmental, no metastases)
•
10-20% of patients has pulmonary metastases
•
Presentation
•
rapidly progressive pain, fever, and swelling
•
may feel mass on examination
•
Radiographs
•
mixed blastic and destructive lesion
•
sun-burst or hair on end pattern
•
periosteal reaction (Codman's triangle)

Osteosarcoma
•
MRI must include entire involved bone to determine
•
soft tissue
•
neurovascular involvement
•
skip metastases in same bone
•
Bone scan
•
chest Ct for metastasis

Osteosarcoma
Treatment
•
multi-agent chemotherapy and limb salvage resection
•
preoperative chemotherapy given for 8-12 weeks
followed by …
•
resection then …
•
maintenance chemotherapy for 6-12 months after
surgical resection
•
Prognosis 76% long-term survival with modern treatment.

Ewing's Sarcoma
•
typically from 5-25 years of age
•
second common malignant bone tumor in children
•
~50% are found in the diaphysis of long bones
•
Genetics t(11:22) translocation in all cases
•
Presentation
•
pain with fever
•
mimics an infection !!!!!
•
swelling and local tenderness
•
Radiographs
•
destructive lesion in the diaphysis or metaphysis with a moth-eaten
appearance
•
periosteal reaction give "onion skin" or "sunburst" appearance
•
MRI .. soft-tissue extension and marrow involvement
•
CT chest and bone scan for metastasis
Ewing's Sarcoma

Ewing’s Sarcoma
Treatment
•
Neoadjuvant chemotherapy with limb salvage resection followed
by postoperative chemotherapy
•
the standard of therapy in most patients
•
Neoadjuvant chemotherapy given for 8-12 weeks followed by
surgical resection then maintenance chemotherapy for 6-12 months
•
Prognosis
•
60-70% long term survival with
isolated
extremity disease
•
15% long term survival if patient presents with
metastatic
disease

Bone Metastasis / Secondary Bone
Tumor
•
most common malignancy of bone is metastatic disease
•
metastatic lesions are usually found in older patients (> 40 years)
•
carcinomas commonly spread to bone include (Breast, lung,
thyroid, renal, prostate)
•
common sites of metastatic lesions include spine> proximal
femur> humerus
•
Symptoms
•
pain
•
pathologic fracture
•
metastatic hypercalcemia

Evaluation of bone metastasis
Workup for older patient with bone lesion and unknown primary
includes
•
Imagining:
•
plain radiographs in two planes of affected limb
•
CT of chest / abdomen / pelvis
•
bone scan to detect extent of disease
•
Labs
•
CBC , ESR
•
LFTs, Ca, Phos, alkaline phosphatase
•
serum and urine immuno-electrophoresis
•
biopsy .. where a primary carcinoma is not identified, obtaining a
biopsy is necessary to rule out a primary bone lesion.

Treatment of metastatic bone disease
•
Nonoperative …
•
bisphosphonate therapy
•
chemotherapy, radiotherapy, and hormone therapy
•
Operative
.. aim is not cure but to improve the quality of life !!!
•
stabilization of complete fracture with postoperative radiotherapy
•
prophylactic stabilization of impending fracture, postoperative
radiation