Clubfoot
Congenital Talipes
Equinovarus
Fifth Year – Tikrit Medical College

Introduction
•
Idiopathic deformity of the foot / unclear etiology
•
Incidence … 1:250 to 1:1000 (1:100 in DDH)
•
Males > Females (F6;M1 in DDH)
•
50 % bilateral (20% in DDH)
•
familial in 25%
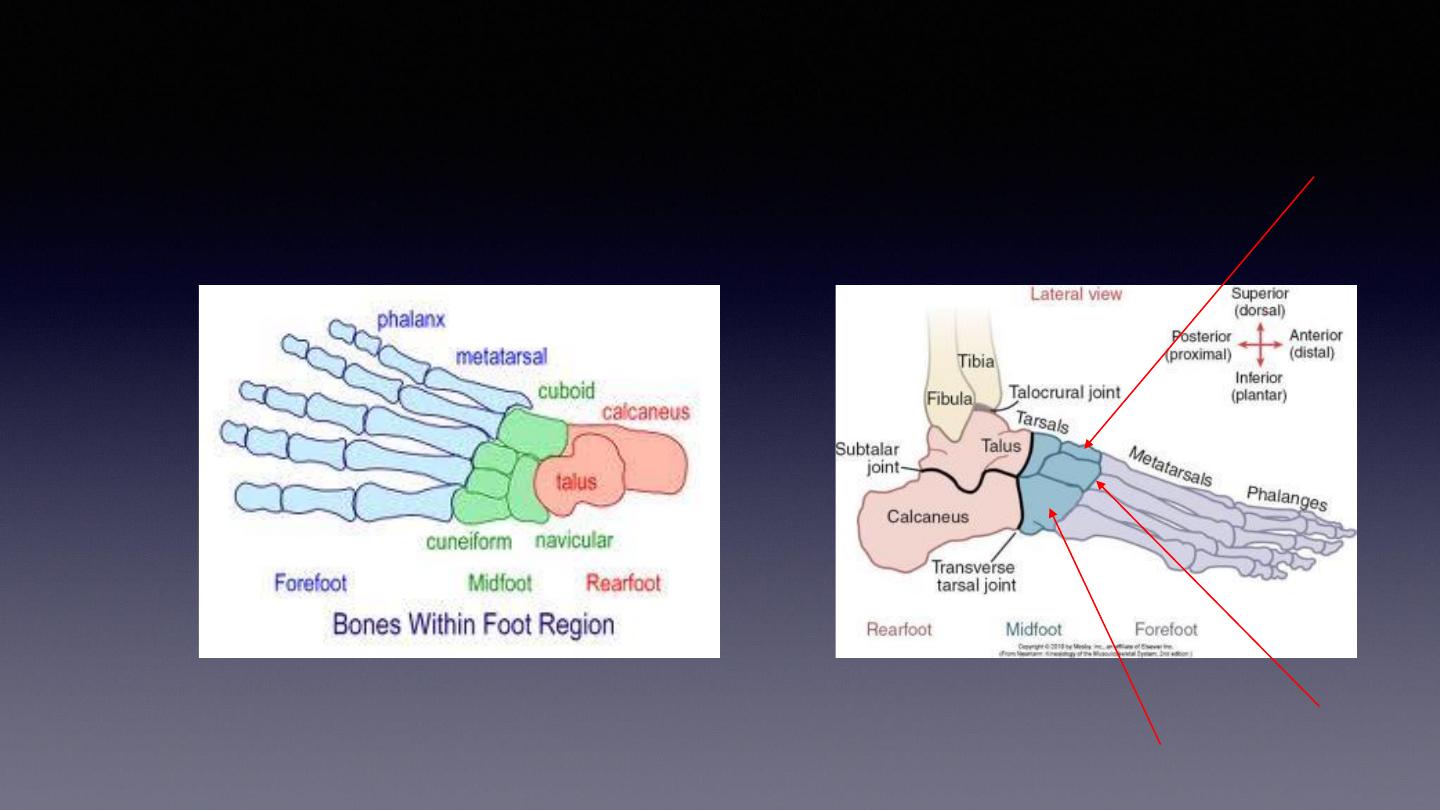
Foot anatomy review !!!!!
Froefoot
midfoot
hindfoot
Middle
cuneiform
cubiform
TMT
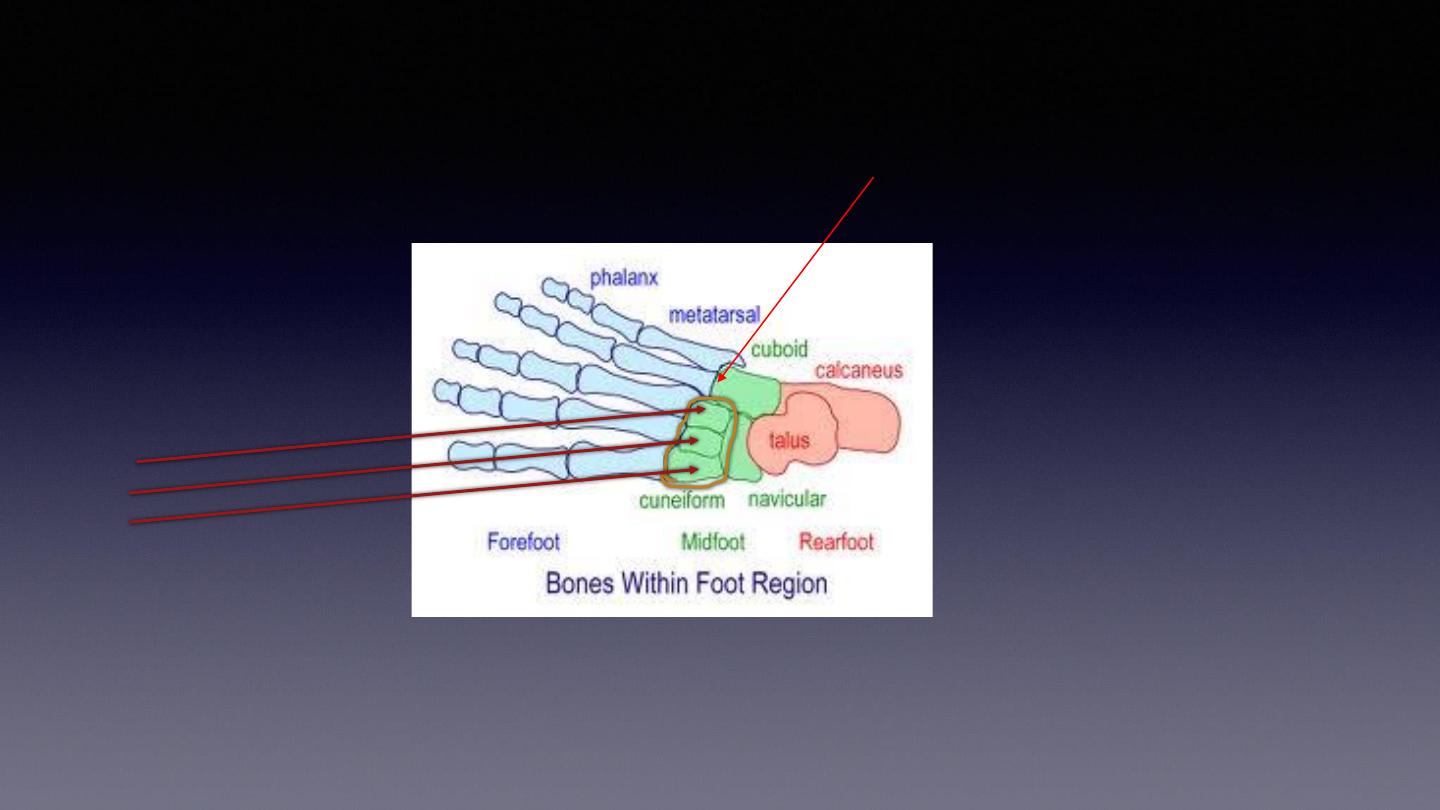
medial
middle
lateral
tarsal
Tarsometatarsal joint (TMT)

Pathoanatomy
•
Muscles contractures lead to the characteristic deformity (
CAVE
); it’s abnormal muscle
tension > contracture of muscle and joint capsule > if leave it >longstanding process>
secondary bony change !!
•
Cavus
midfoot (tight intrinsics, FHL, FDL)
•
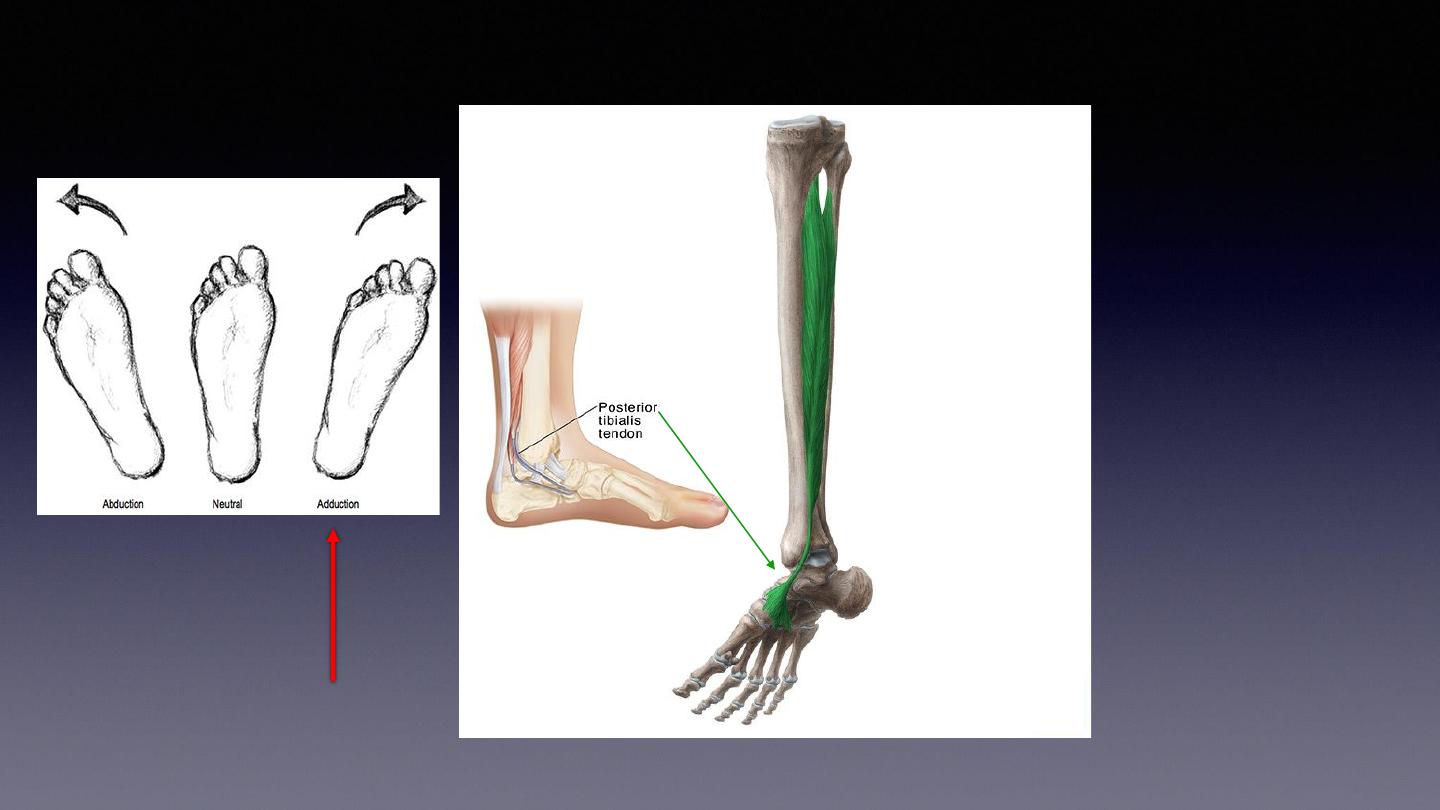
Adducted
forefoot (
from TMT to Fingers
) > tight tibialis posterior .
•
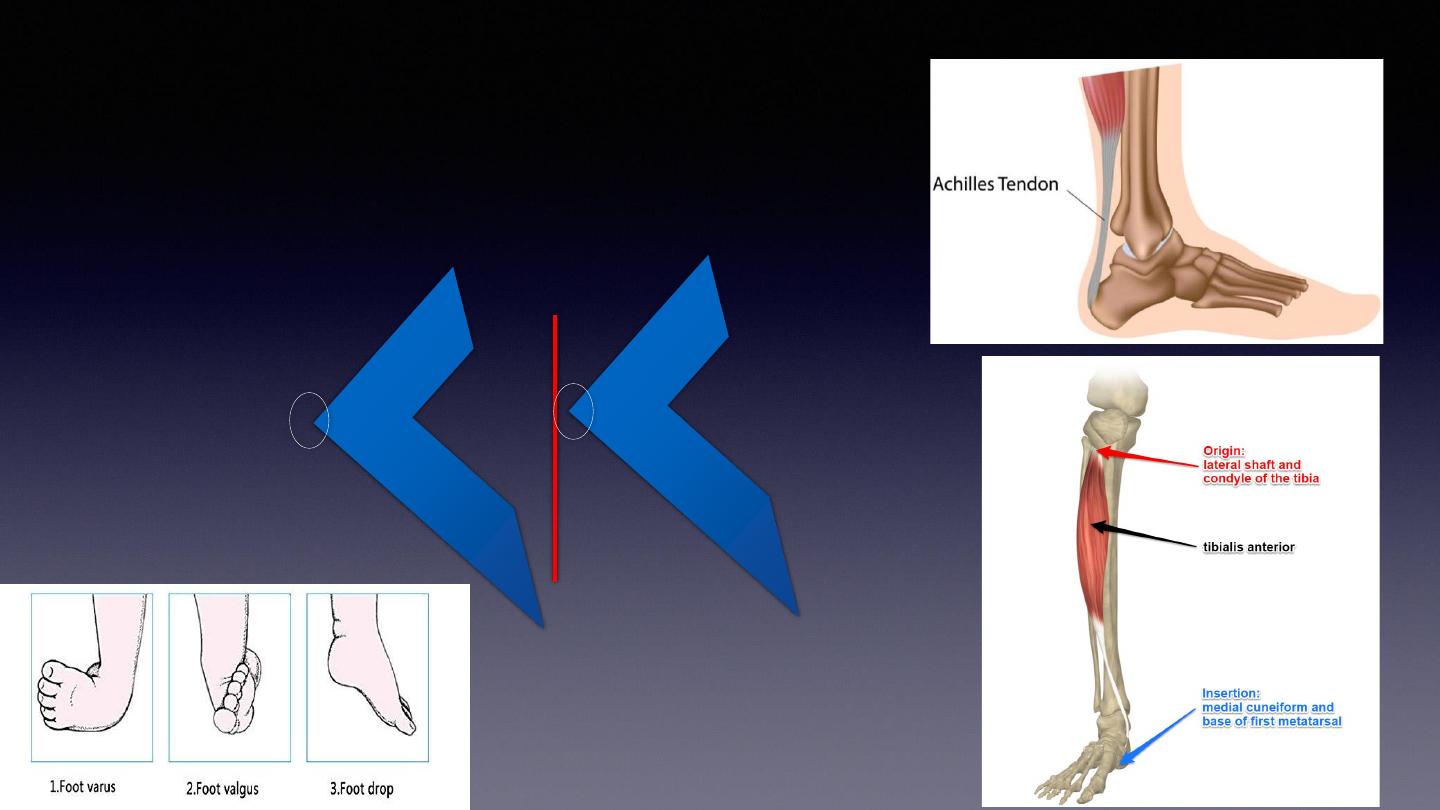
Varus
hindfoot (tight tendoachilles, tibialis posterior, tibialis anterior)
•
Equinus
hindfoot (tight tendoachilles)
* Foot is so stiff (
may fracture if try to fix it manually
).
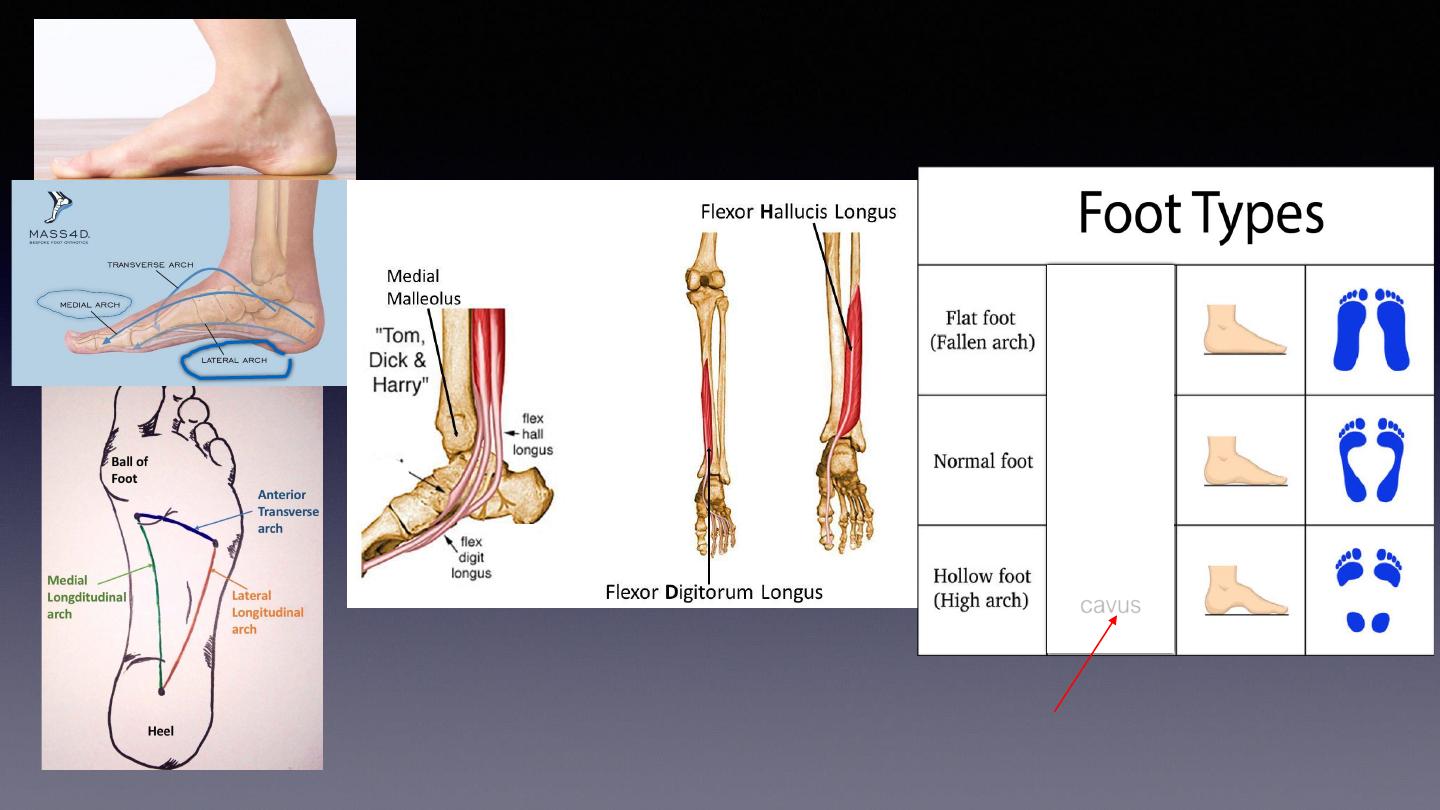
cavus
In midfoot problem
◄
◄
FHL
FDL
Adducted forefoot;
Shift metatarsal to inner side
Soleus
muscle
Valgus : angle of joint toward the mid-line
Varus : angle of joint away from the mid-line
Vaglus is normal in upper limbs elbow
varus
valgus
Mid-line
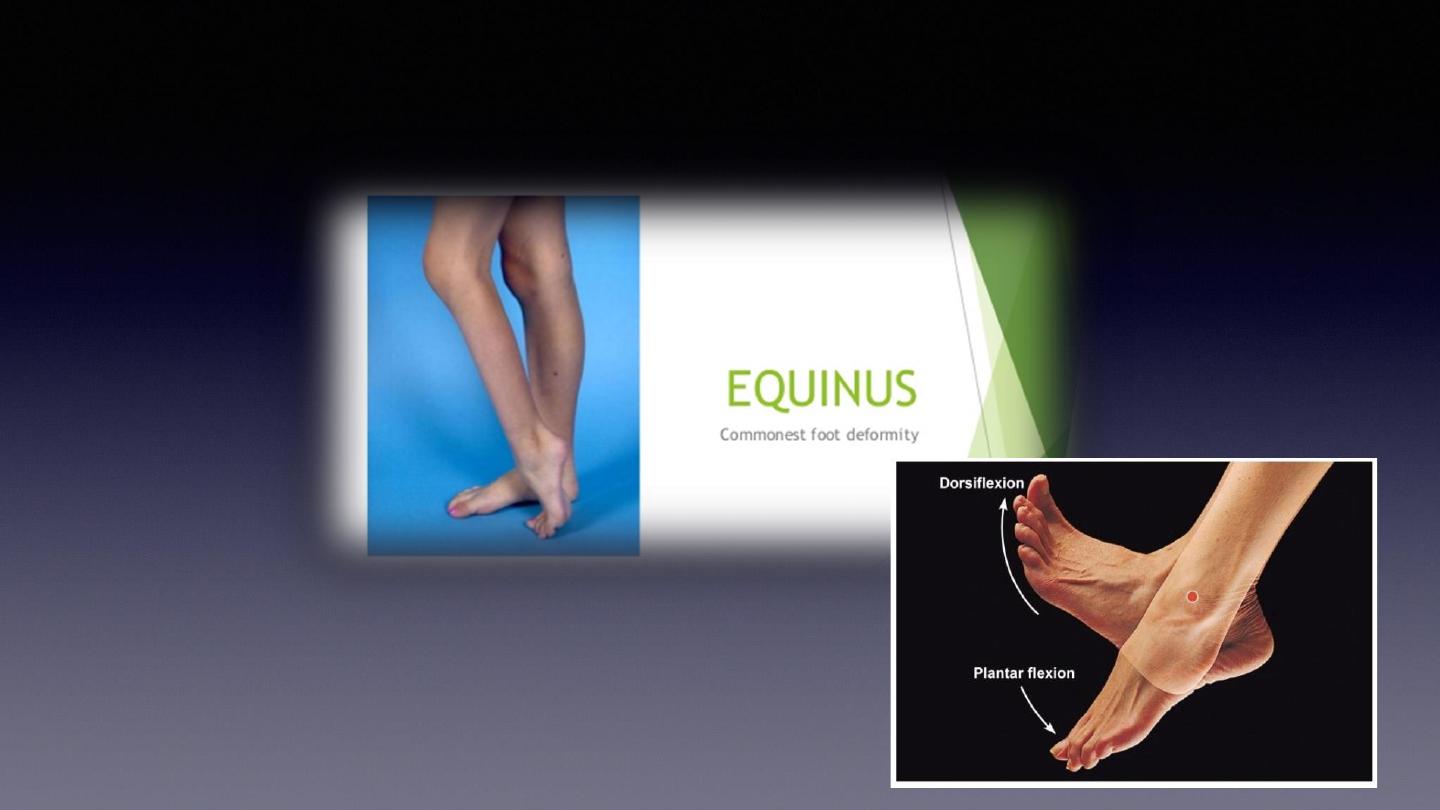
Equinus : is excessive planter flexion (opposite to dorsiflexion).
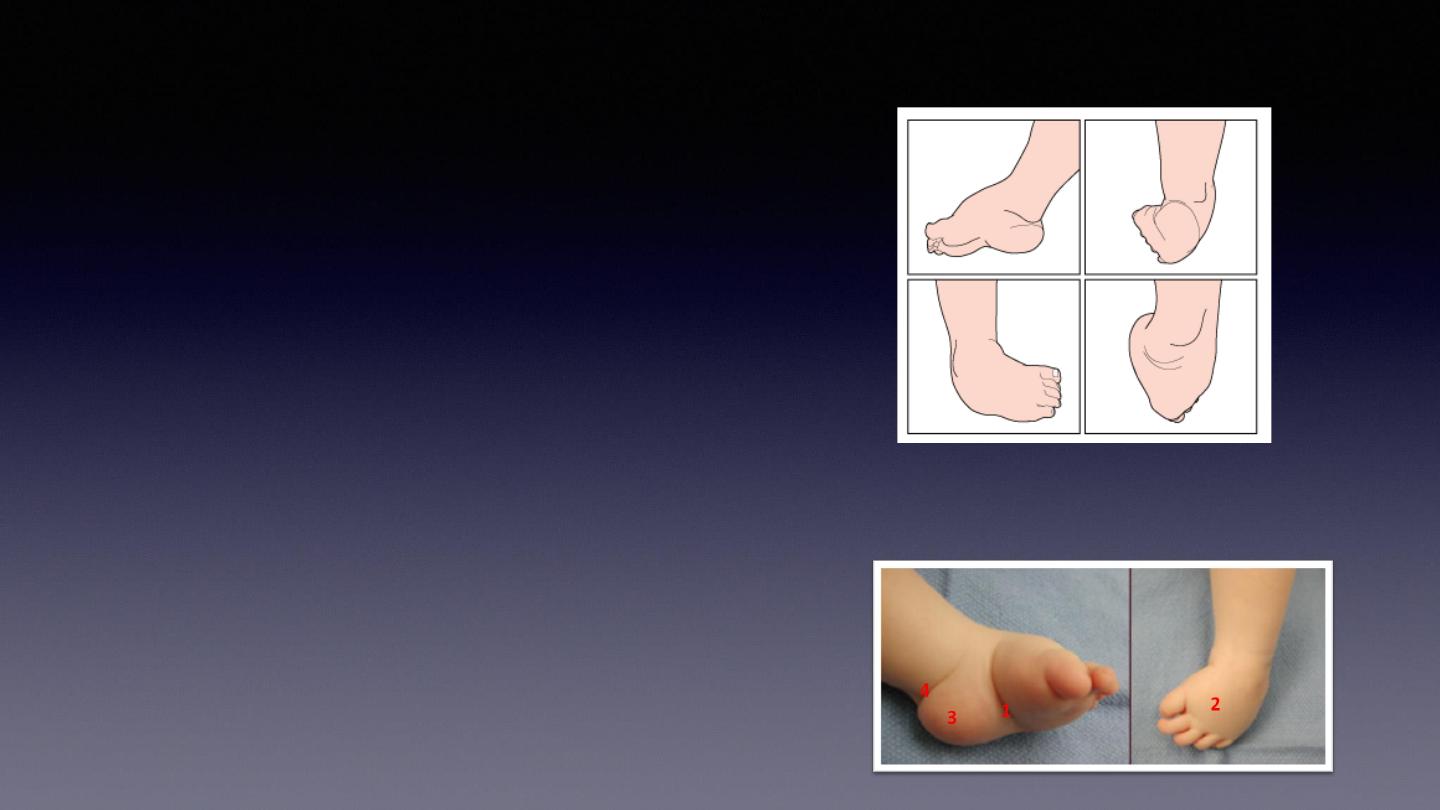
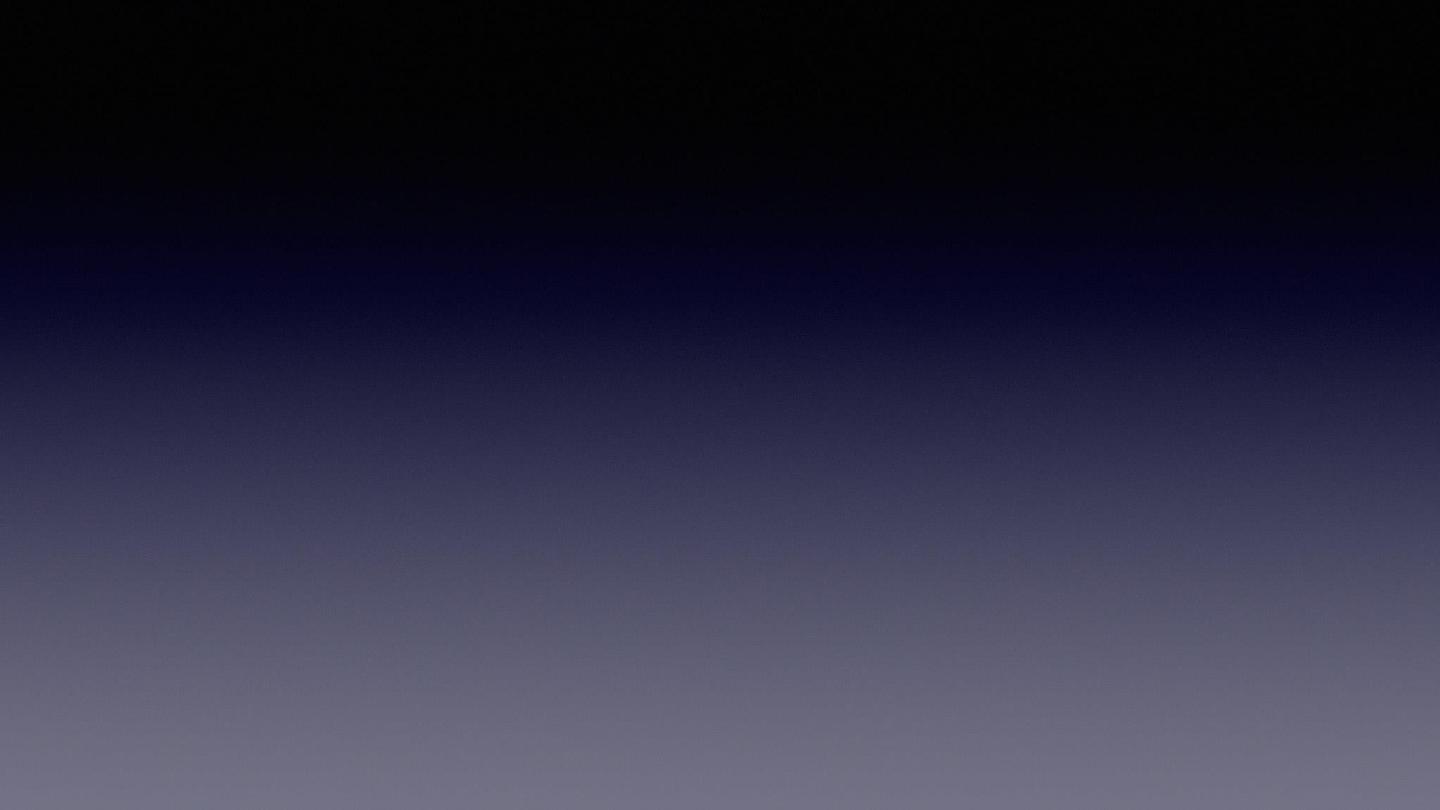
Presentation
❑
small foot and calf
❑
medial and posterior foot skin creases
❑
Rigid hindfoot in equinus and varus
❑
midfoot in cavus
❑
forefoot in adduction
cavus
adduction
varus
Equinus
Planter
Flexed
Treatment
1- Non operative
•
serial manipulation and casting (
Ponseti method
)
•
Ponseti
method has 90% success rate
•
goal is rotate foot laterally around a fixed talus
•
order of correction (CAVE)
•
midfoot cavus
•
forefoot adductus
•
hindfoot varus
•
hindfoot equinus
Ponseti method
Ponseti method
•
Weekly serial casting (with knee in 90° of flexion )
•
Correction order in CAVE
•
Achilles tenson lengthening at week 8 required
in 80 %
•
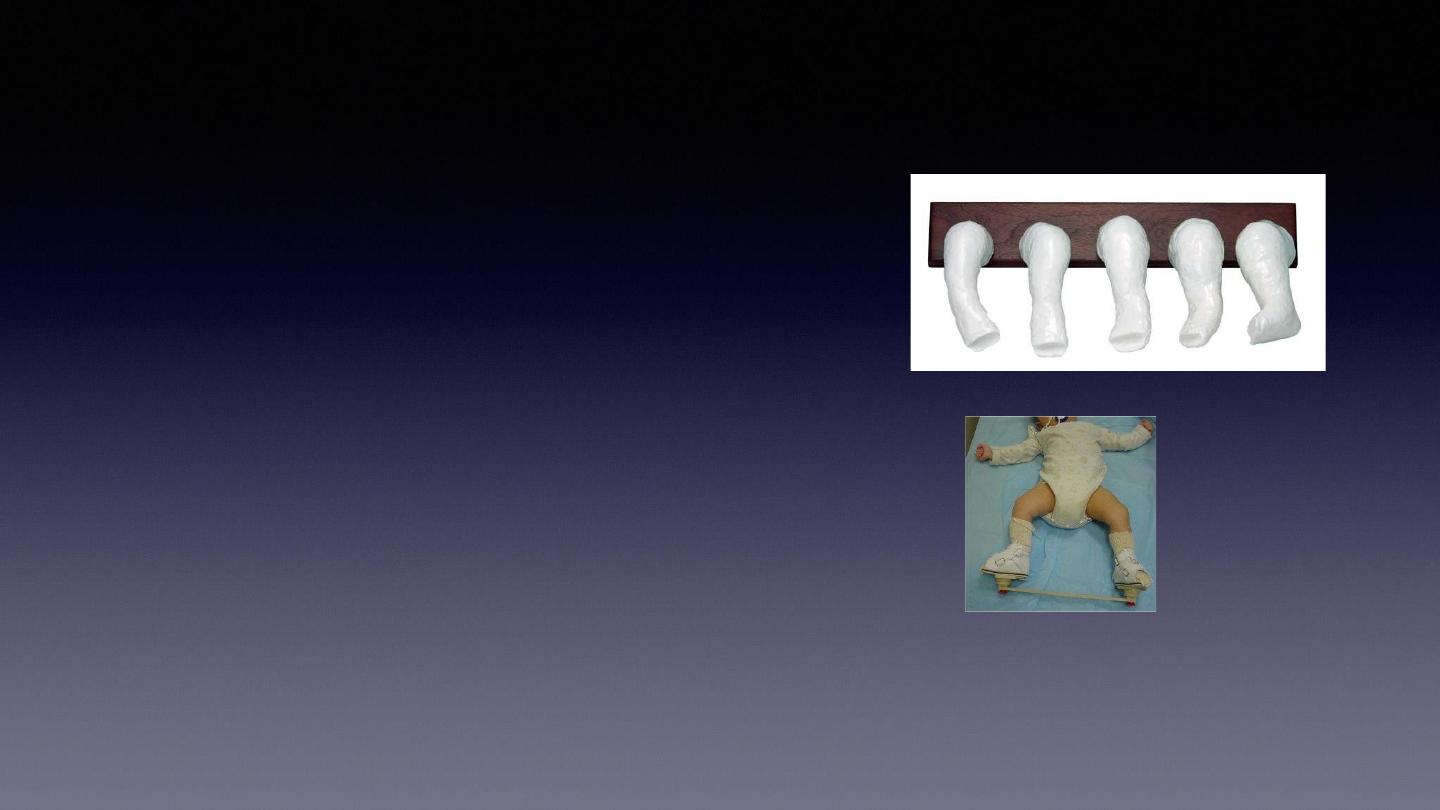
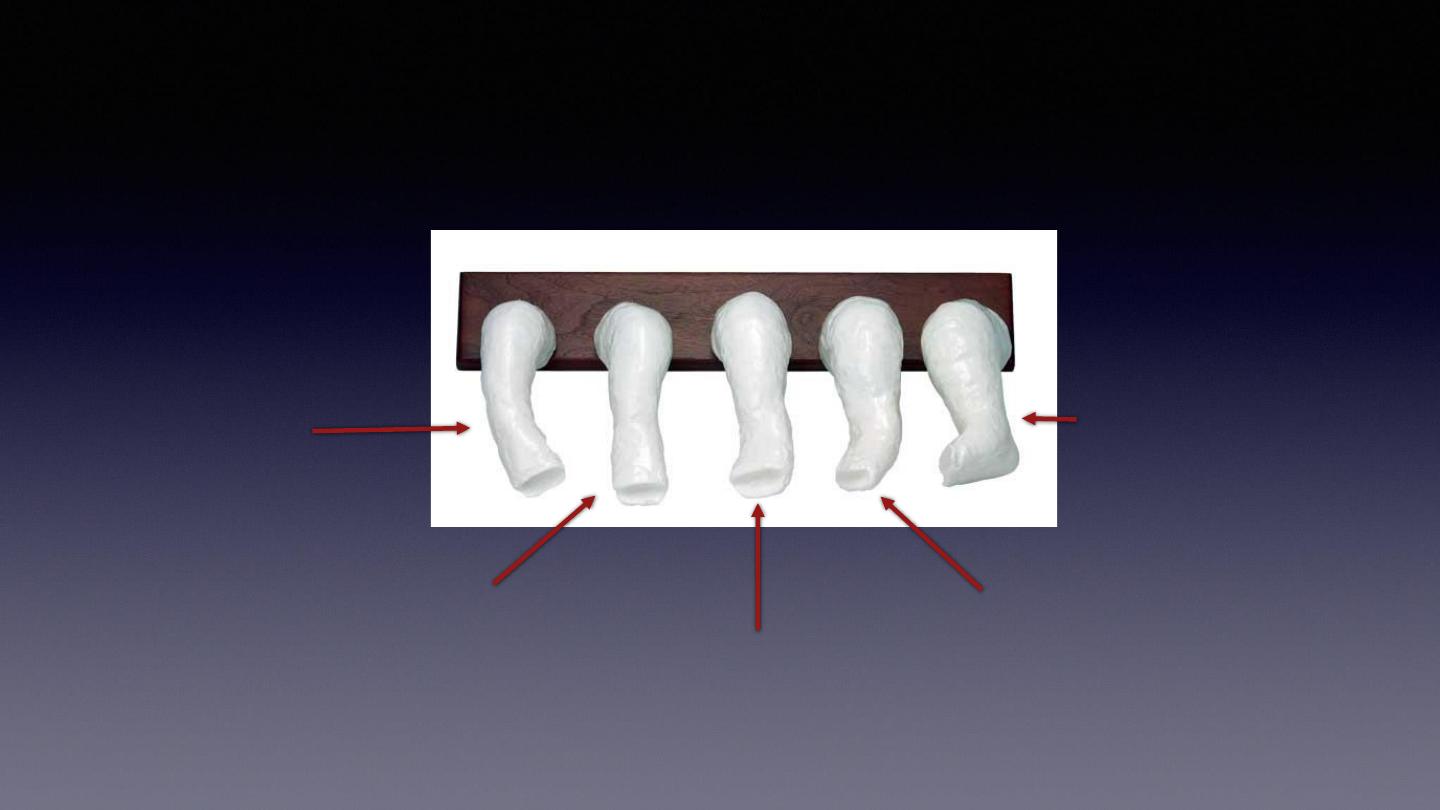
Foot abduction orthosis (FAO)
•
worn after full correction 23 hours / day for 3 months
•
then night time/nap time only until age 4 years
First week
elevate first metatarsal
Second week
Correction of adduction
Third week
Correction of varus
(slightly valgus)
Fourth week
Over correction of
Varus to valgus
Fifth week-8wks
Correction of equinus by
Elongation of achilles
Tendon (cutting) lengthening
Casting on dorsiflexion
Ponseti is not forceful , it is gradual correction by stretching following by casting.
Operative
1- posteromedial soft tissue release and tendon
lengthening
•
performed at 9-10 months of age so the child can be ambulatory at one year
of age (because at 10 months , foot is sizeable \\ secondly, surgery at 10
months followed by 1.5months casting then the child meet the age of
waliking , which help to fix the problem as the body weight pressing the
abnormal foot, premature surgery may lead to recurrence of deformity
beofore the baby meet the age of walking.).
•
Indications
•
resistant feet in young children (failed to respond on ponseti )
•
"rocker bottom" feet that develop as a result of wrong serial casting
•
syndrome-associated clubfoot
•
delayed presentation
>1-2 years of age
Rocker bottom foot
, also known as
congenital vertical talus, is an anomaly of
the foot. It is characterized by a
prominent calcaneus (heel bone) and a
convex rounded bottom of the foot.
operative management in older
children
•
older children from 3 to 10 years (bony changes occur \ no role of soft tissue
release ~ no role of muscle release)
•
medial arch lengthening or lateral arch shortening osteotomy, or cuboid
decancellation
•
refractory clubfoot at 8-10 years of age
•
triple arthrodesis (partial removal of rigid joint and fuse it in desired position).
•
talectomy
•
salvage procedure in older children (8-10 yrs) with an insensate foot
Complications
•
deformity relapse
•
in child < 2 years
repeat casting
•
relapse in child > 2 years
•
initially with casting
•
then repeat Achilles tendon lengthening +- Tibialis anterior split transfer
•
residual cavus
•
pes planus from overcorrection
•
in toeing gait
•
osteonecrosis of talus (due to forceful ponseti)