
Developmental Dysplasia of the Hip
Fifth year lecture – orthopedic
Dr. Omar I. Mahmood

Developmental Dysplasia of the Hip
Introduction
Abnormal development resulting dysplasia , subluxation or dislocation of
the hip
•
DDH spectrum includes
1. Dysplasia (simple) … a shallow / underdeveloped acetabulum
2. Subluxation (moderate)
3. Dislocation (severe)
Developmental is not congenital , it is ongoing process. >> up to 2.5 years,
During this period ,, if there is abnormal hip should discovered early and treated
Early > everything will resolved >> otherwise > simple dysplasia up to dislocation
May occur.
Dysplasia ; (abnormal formation) of acetabulum > abnormal shape
>> is not concave enough to accommodate for the femoral head
Sublaxation ( partial loss of contact between two articular surface)
Newborn baby
normal position
Flexion&
abduction
Of hip joint\ اما بل مهاد
Make him adduction
And extension
Adduction is the
position of dislocation of abnormal hip.
So, when treat the patient we try to do
abduction \\
المهادmay predispose dislocation
Because it induce adduction specially in abnormal hip.
This child
Does not has
Risk of DDH
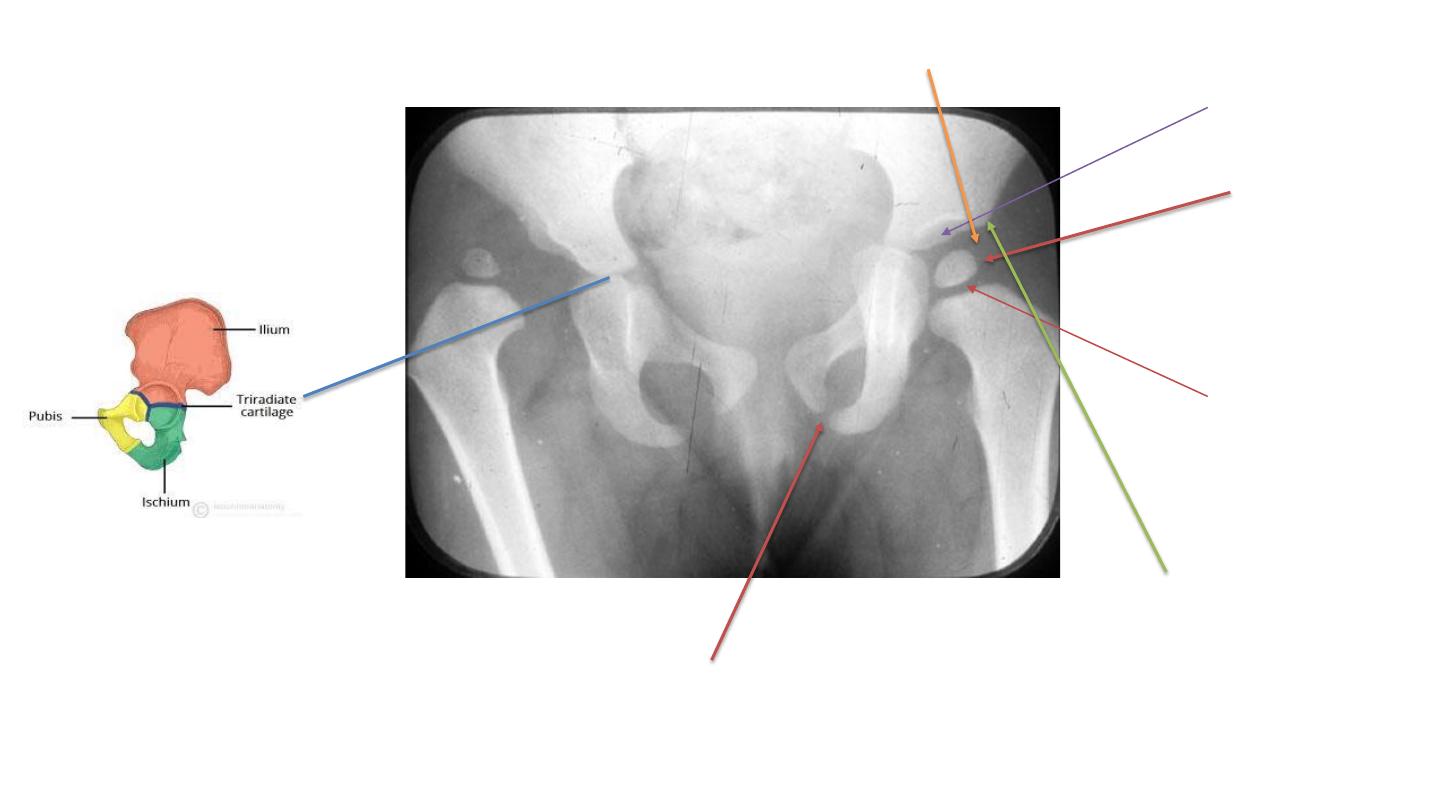
Ossification
Center, which
Can not be seen
Below 4 months
So, do ultrasound
To confirm dx.
Growth plate
Of neck
Cartilage of
Acetabulum
And femoral head
Cartilage of acetabulum
femoral head is radiolucent
Growth plate of pubis
Lateral margin
Of acetabulum

Epidemiology
• incidence
– most common orthopedic disorder in newborns
– dysplasia is 1:100
– dislocation is 1:1000
• location
– left hips / females
– bilateral 20%
• risk factors
– first born female
– female 6:1 males
– family history
– Fetal malposition/breech/oligohydramnios (abnormal strain of joint with intrauterine life)
Pathophysiology
• Instability caused by
1.
maternal hormones
relaxin (secreted by placenta in last trimester relaxing the birth
canal>> relaxation of joint capsule)
2.
genetic laxity (family history) .
3.
intrauterine and postnatal mispositioning( breech presentation مهاد الطفل و> exacerbate
dysplasia )
– instability dysplasia dislocation

Presentation
< 3 months of age
• hip subluxation/dislocation palpable on exam
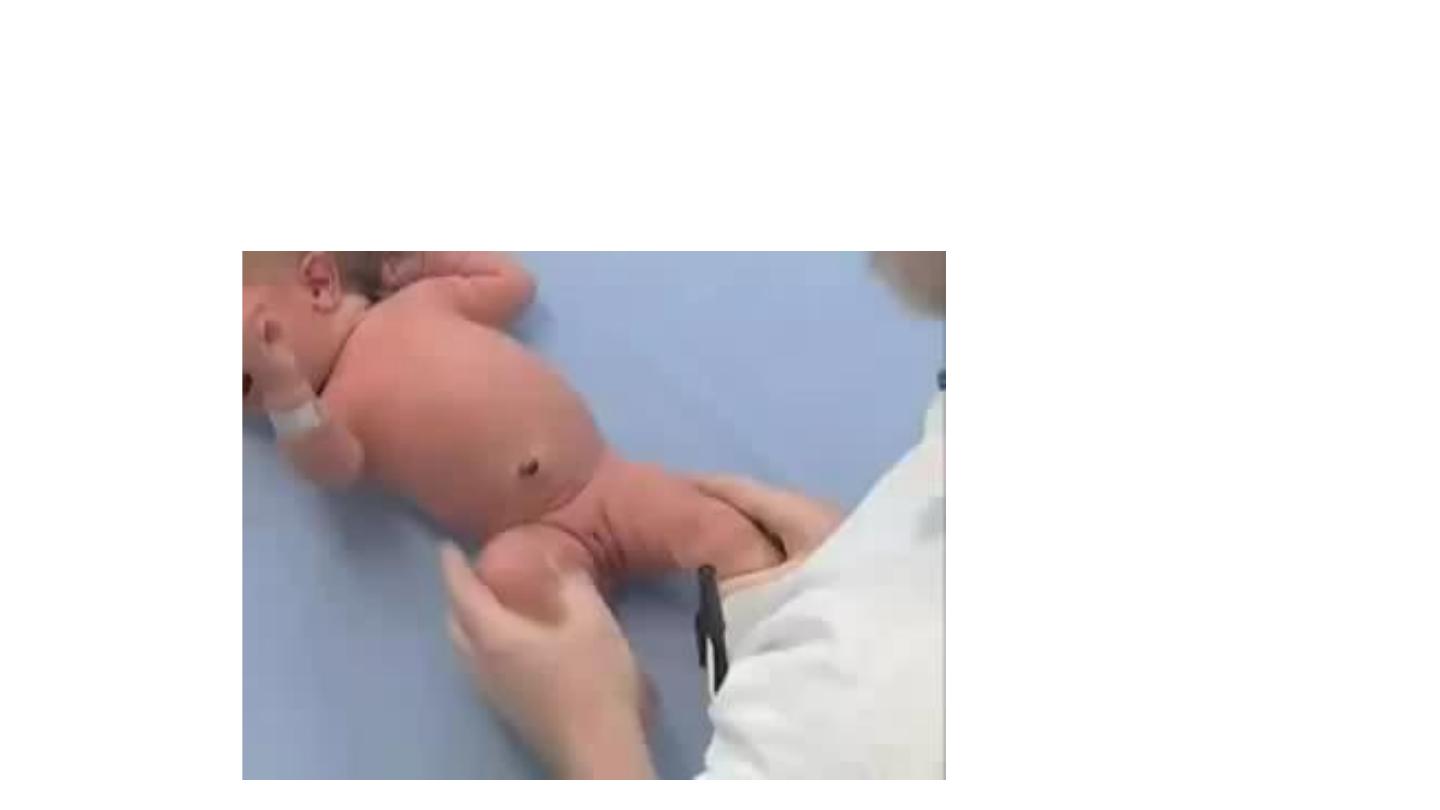
• Barlow test
..
dislocates a dislocatable hip by adduction and depression of
the flexed femur
• Ortolani test
..
reduces a dislocated hip by elevation and abduction of the
flexed femur
• Galeazzi
..
limb length discrepancy with hip and knee flexed at 90 degrees
• Barlow and Ortolani a rarely positive after 3 months of
age

we inducing dislocation – it is impossible to do dislocate normal hip – so this test used to see if
the hip stable(impossible to dislocated) or unstable (will dislocated) by certain maneuver
(flexion of both hips in 90 degree > force addaction ; both knees meet together in the midline
then we push backward) ,, two posabilities:
Either (+) when dislocation occur , feel or hear click
Or (-) when nothing occur .
Barlow test
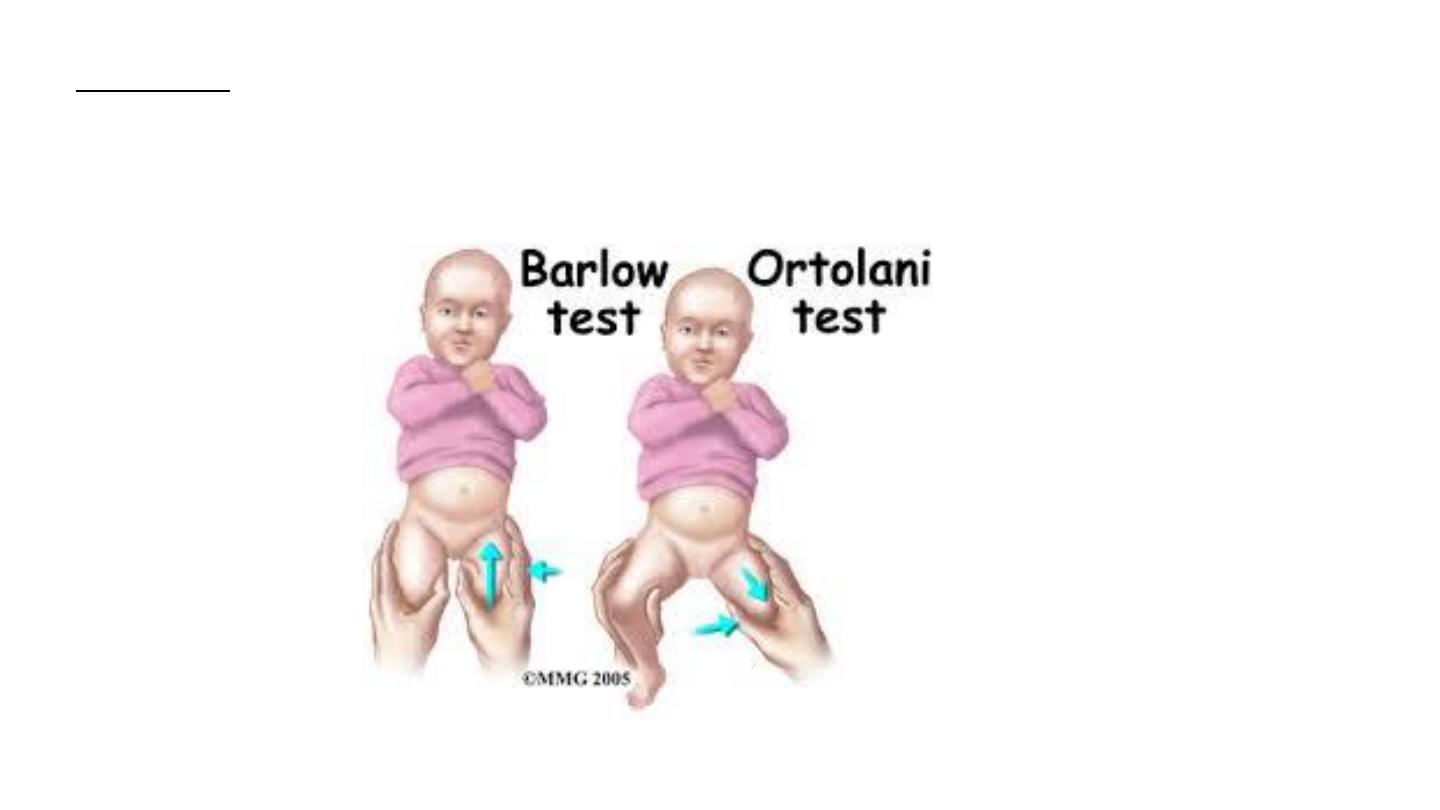
Ortolani test we keep the hip flexed 90 degree then we do abduction and elevation of femoral head by using
The long finger over the trochanter and push forward .. 2 possibilities occur ;
+ a) either the hip is already dislocated , then we will hear or feel click of reduction.
-
b) or the hip is stable (nothing will occur)

o When barlow (-) and ortolani (-) hip is normal
o When barlow (-) but ortolani (+) hip is already dislocated
o When both are ++ ( dysplasia or sublaxation) mean that the hip
is so laxated that we can dislocate it and bring it back easily.
Ortolani and Barlow tests
Ortolani and Barlow tests
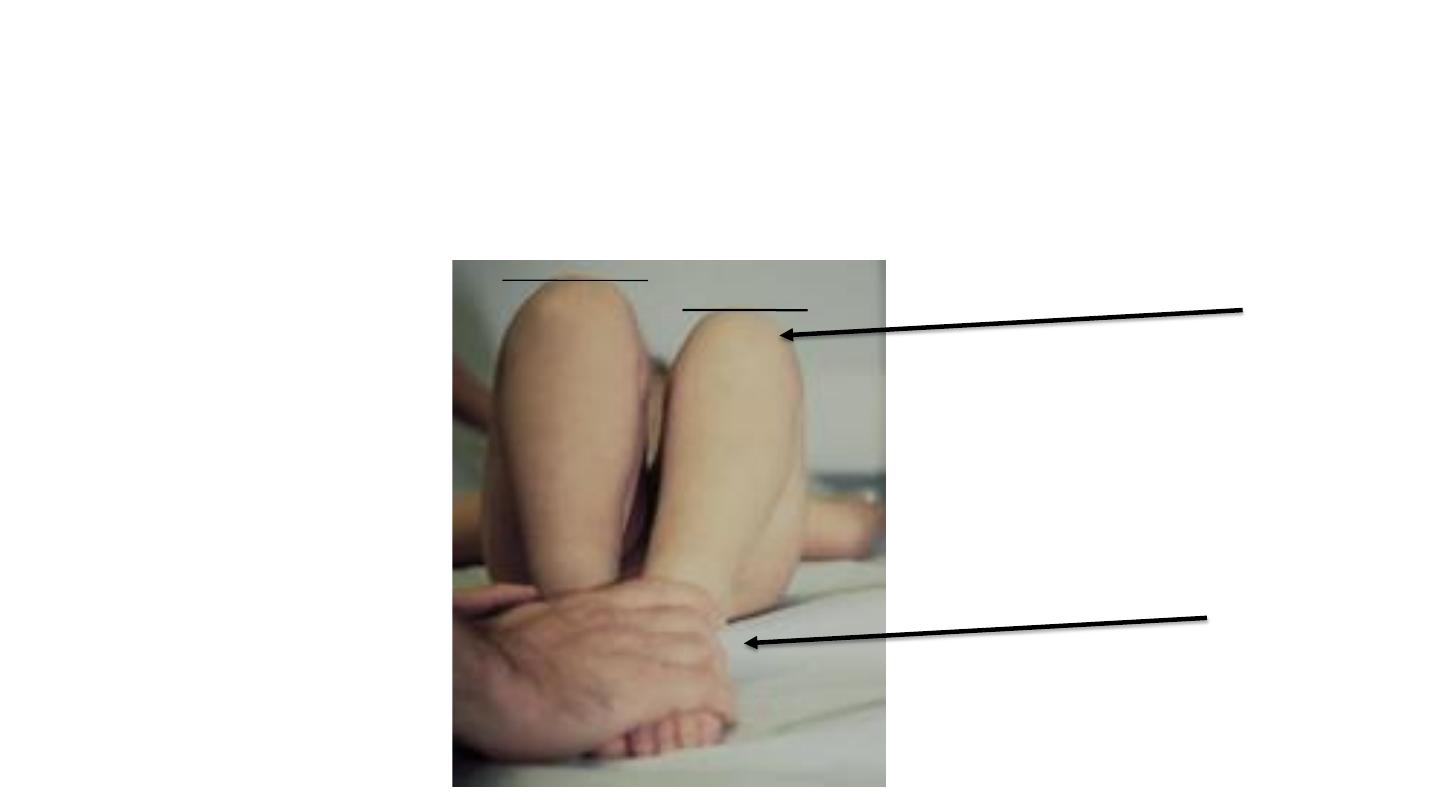
Galeazzi sign
At same level
dislocated
Benefit in unilateral dislocation
Not benefit in bilateral
Classification
1. Dislocated
– Ortolani-positive early when reducible; Ortolani-negative late when irreducible
2. Dislocatable
– Barlow-positive
Presentation
> 3 months of age (contracted capsule and muscle strong
due to long abnormal position of dislocated hip )
• limitations in hip abduction contractures begins .
– Symmetrically limitation in bilateral dislocations
– Unilateral limitation in unliteral dislocation
• Galeazzi … leg length discrepancy positive in unilateral

Presentation
> 1 year - walking child
• Unilateral dislocation
– pelvic obliquity
– Trendelenburg gait ….. results from abductor insufficiency
– toe walking ….compensate for shortening of affected side
• bilateral dislocations
– lumbar lordosis and waddling gait
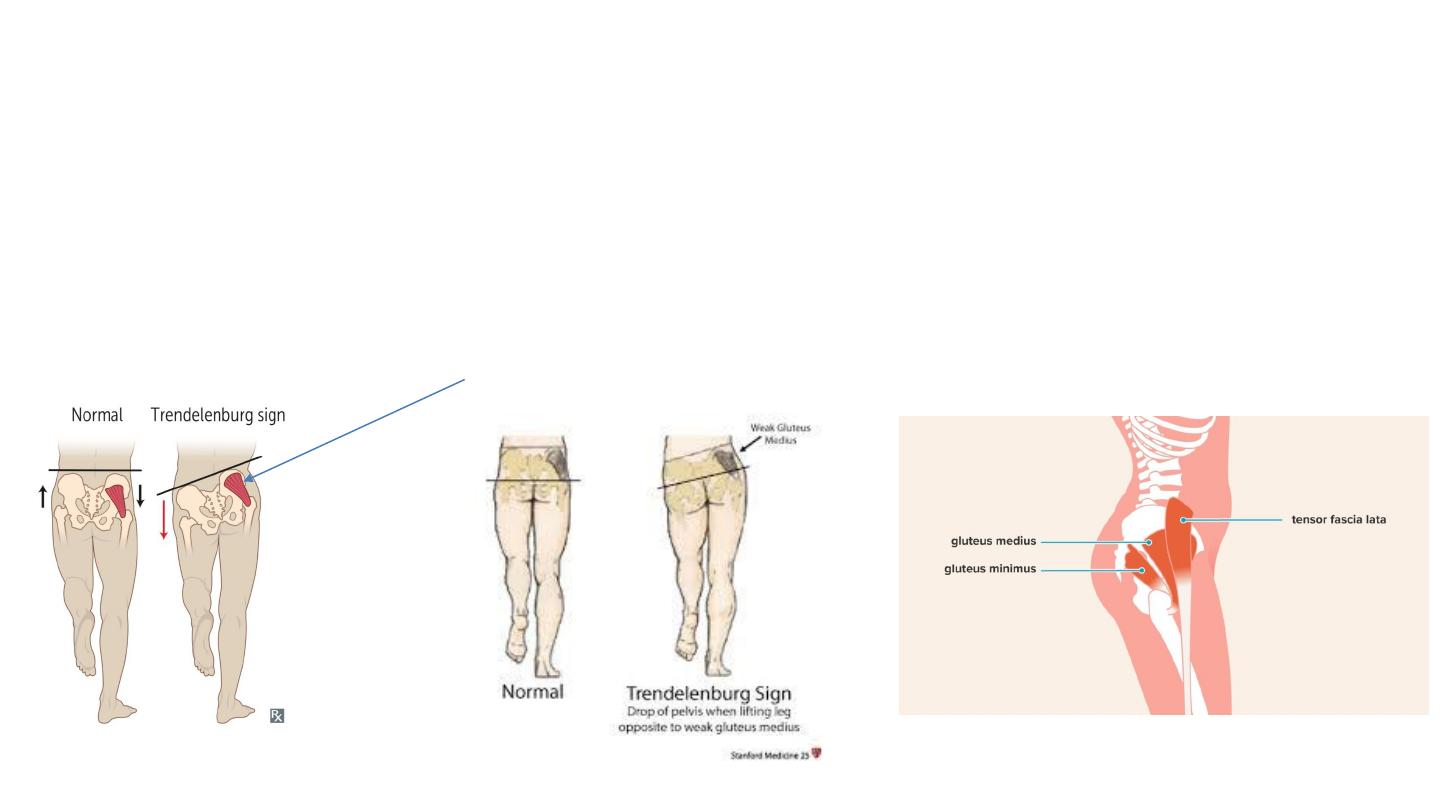
Trendelenburg gait : is an abnormal gait (as with walking) caused by weakness of the abductor muscles of the lower
limb, gluteus medius and gluteus minimus and tensor facia lata.
-in weak muscle , hip dislocation , painful hip
-Abductor muscles contracted in ipsilateral stand limb to carrying the body weight
On one limb (( when asking the patient to stand on one limb.))
- If patient stand on affected side > body fall on other normal side.
- If bilateral weakness in abductor (waddling gait)
Abductor weakness
تكع على الجهة الطبيعية
Trendelenburg gait
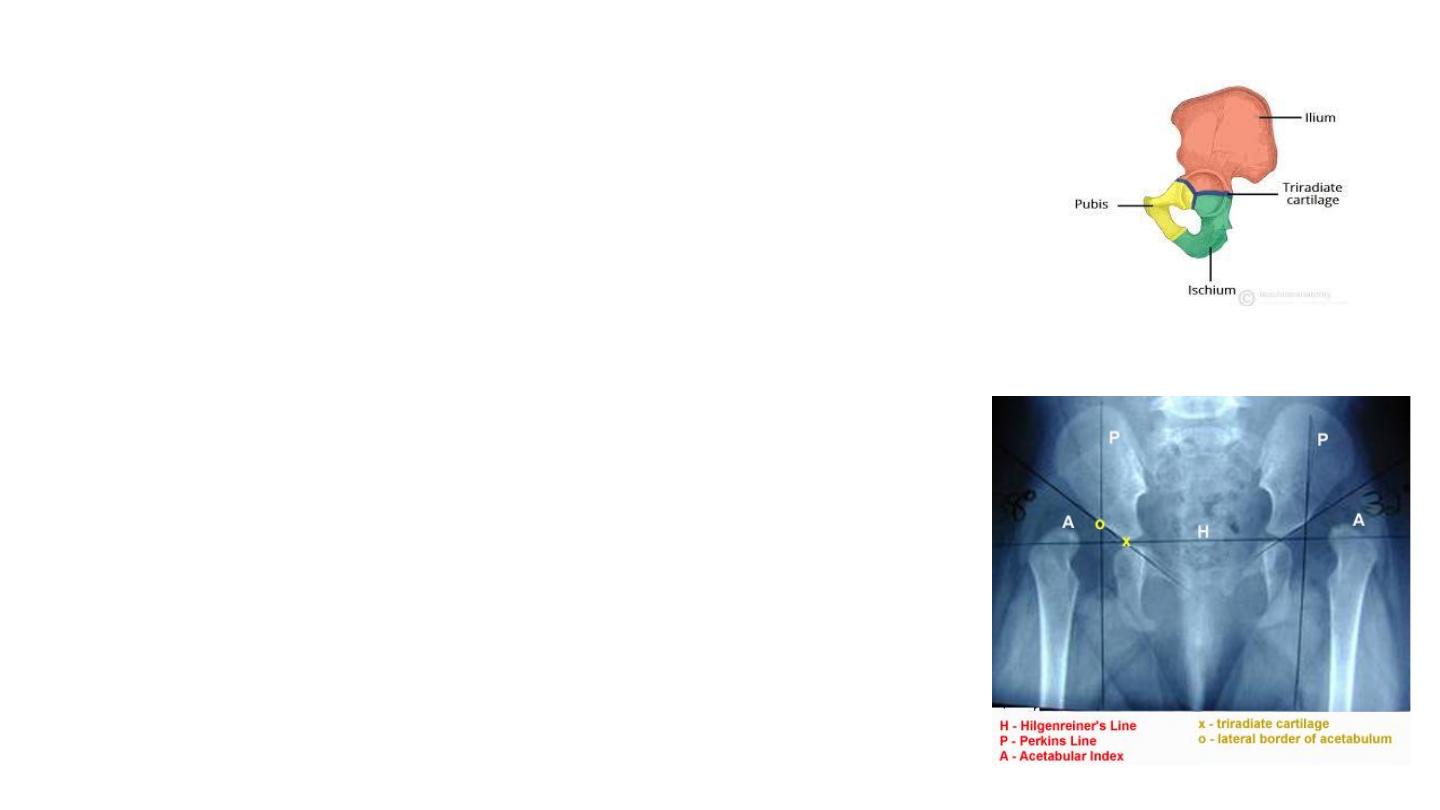
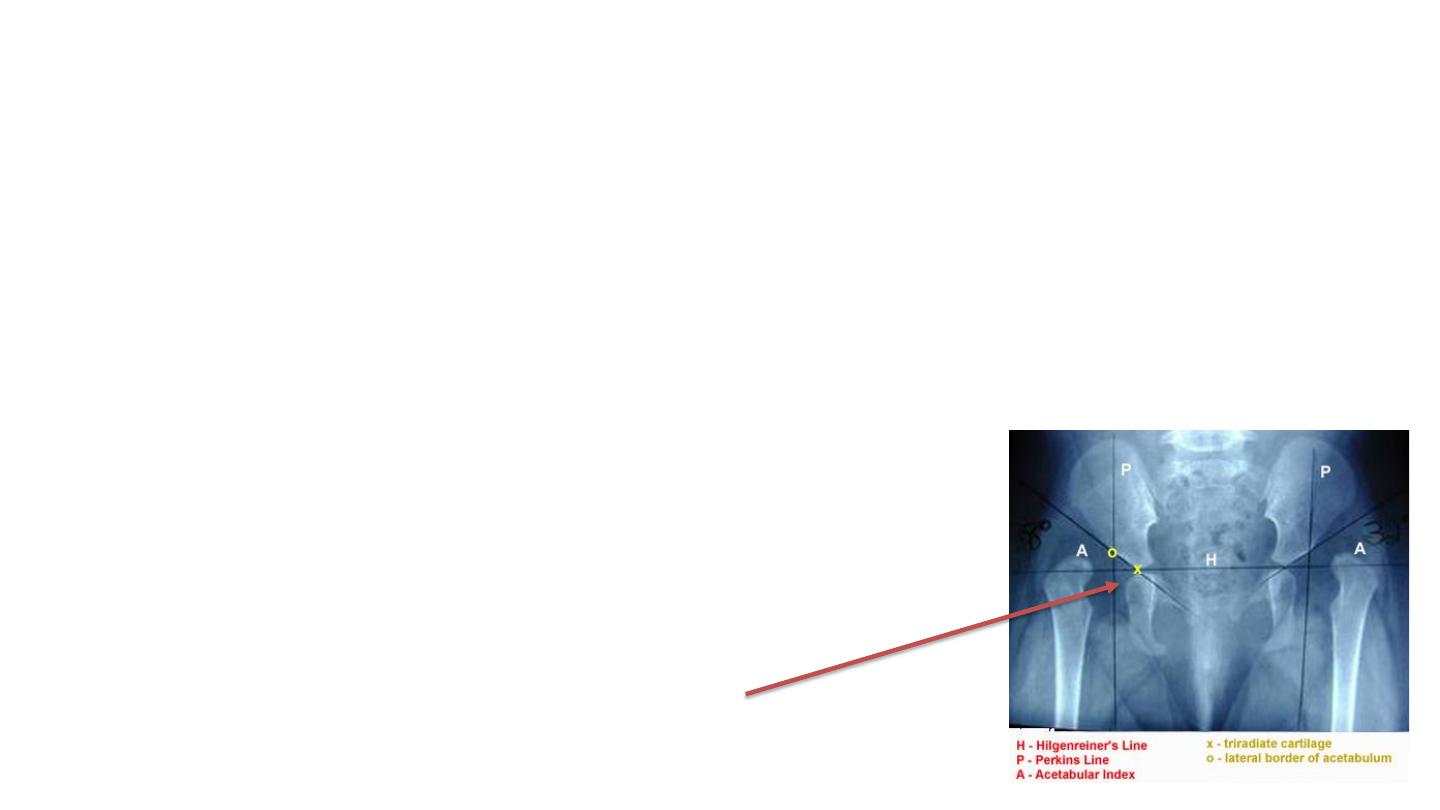
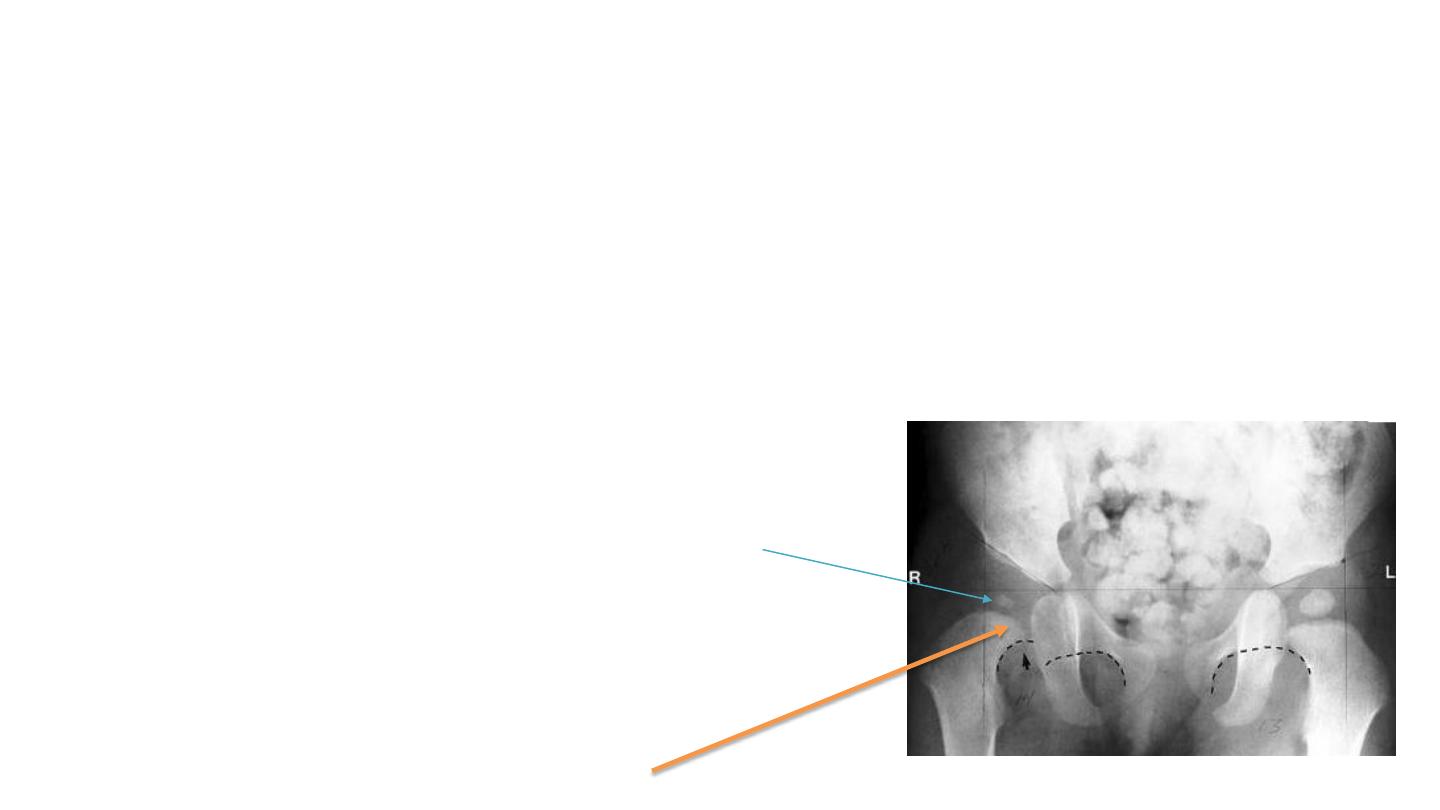
Radiological features in DDH
1- Hilgenreiner's line
• horizontal line through right and left triradiate cartilage
• femoral head ossification center should be inferior to this line
• Dislocated hip if its located above this line
Ossification center not obvious (it is below 4months)
Here it is bilateral dislocation
Head above hilgenreiner’s line
Radiological features in DDH
2- Perkin's line
• line perpendicular line to Hilgenreiner's through a point at
lateral margin of acetabulum
• femoral head ossification should be medial to this line
• If femoral head located lateral to this line its
dislocated
If we divide the side into
Four quadrants:
Head of femur should be in
The infermoedial quadrant
Radiological features in DDH
3- Shenton's line
•
arc along inferior border of femoral neck and superior margin of
obturator foramen
• arc line should be continuous
• If its broken then the hip dislocated
4-
delayed ossification of femoral head
.. is seen in cases of dislocation
This head of femur
Is in inferomedial
Quadrant but it has
Broken shenton’s line
So it is sublaxated
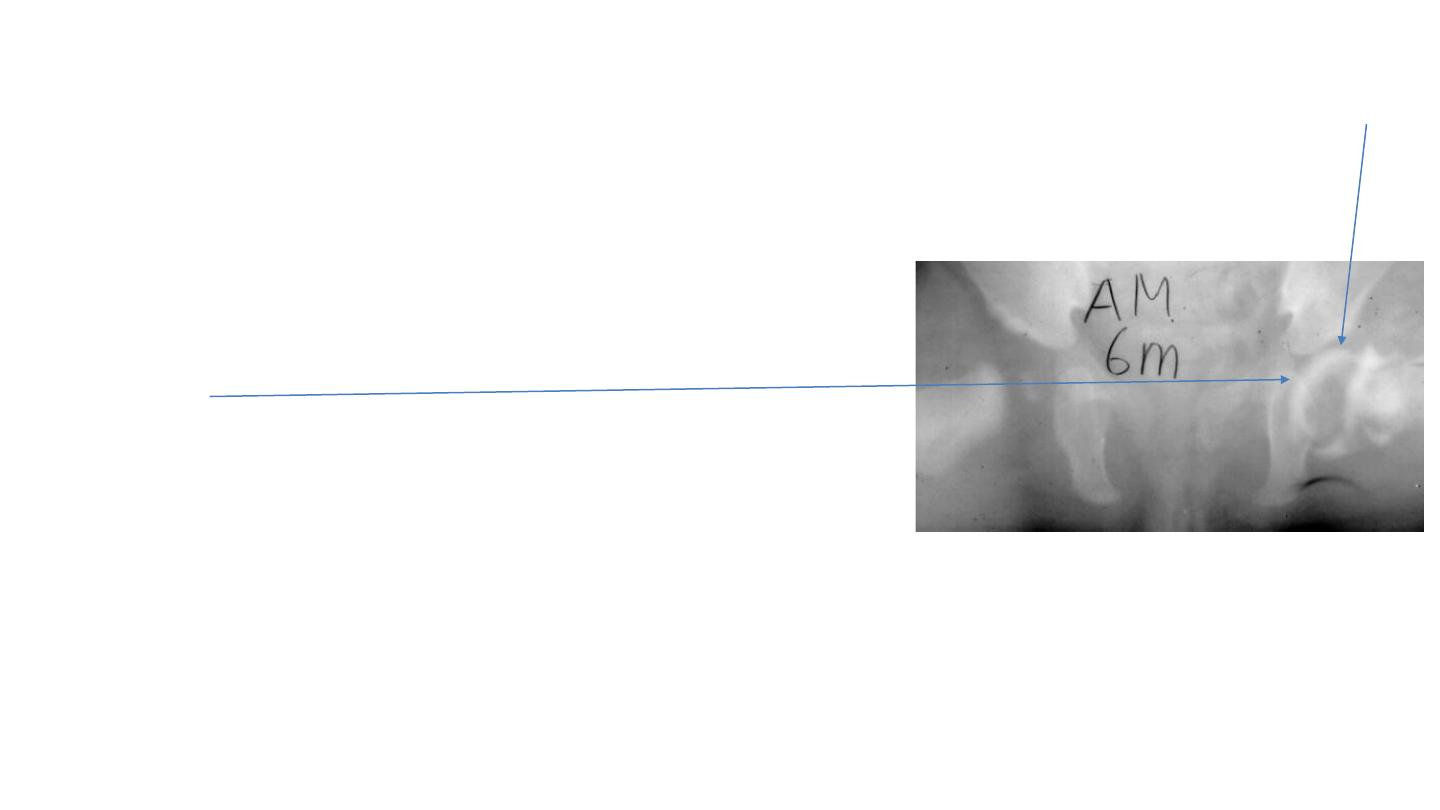
Other imaging in DDH
Ultrasound
• useful before femoral head ossification <4-6 months
• not cost effective for routine screening
Arthrogram
used to confirm reduction during closed reduction under anesthesia
Injection of radio-opaque material on joint (cartilage head)
CT:
study of choice to evaluate reduction of the hip after closed reduction and spica casting
Synovial space

Management of DDH < 6 months of age
By abduction splinting/bracing (Pavlik harness )
• a dynamic splint … requires muscle function for successful outcomes
• Pavlik harness success rate of 90%
• Bracing position is 90° flexion (by anterior straps) and abduction of 45° (by posterior
straps) preventing the baby from doing unwanted extension or adduction
like مهادso , it limit the movement partially leaving the bone in favorable position.
• worn for 23 hours/day for 6 weeks or until hip is stable (re-assessment by
barlow\ortolani
)
• wean out over 6-8 weeks until normal anatomy develops
• Monitor with ultrasound or x-ray and every 4-6 week
• Stop pavlik harness if not successful after 3-4 weeks when re-assessment still lax.
• Use of pavlik harness if the barlaw (+) and\or Ortolani (+) but can not be used if both are
negative and Galeazzi sign (+) mean it is unreducable.
Normal position
Of newborn.

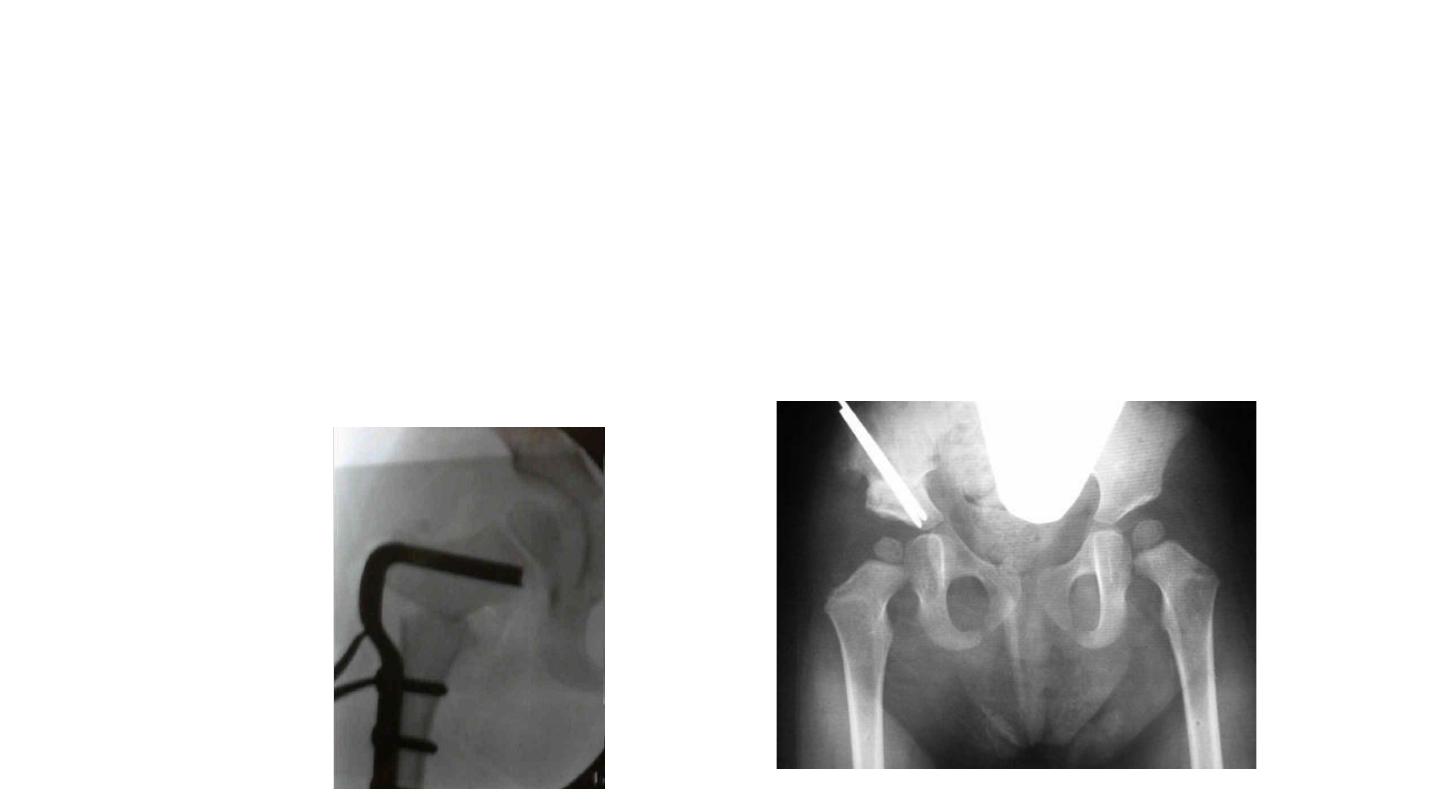
DDH in 6 - 18 months of age or failure of pavlic harness
• closed reduction and spica casting (as next modality)
• adductor tenotomy(( قصهاperformed
• Closed reduction under general anesthesia
• arthrogram to confirm reduction intraoperatively
• immobilize in a spica cast
– hip flexion of 90 deg.
– abduction of 45 deg
– neutral rotation for 3 months
• confirm reduction with CT scan in spica cast

DDH in patient >18 months of age or
failure of closed reduction
• open reduction and spica casting
–remove possible anatomic blocks to reduction
–Capsulorrhaphy ( capsule suturing)
–Spica Casting (( جبسونا اعتياديةimmobilization in functional position
of 15° of flexion, 15° of abduction and neutral rotation
DDH > 2 years
• open reduction plus femoral osteotomy
• +- Pelvic osteotomy
Complications
• Osteonecrosis : in all forms of treatment)in pavlik harness,spika ,,
– excessive or forceful abduction
– repeat surgery
• Delayed diagnosis
bilateral dislocations : patients typically functions better if hips are not reduced 6 years of age or older
unilateral dislocation better outcomes without surgical treatment if patient is 8 years of age or older
• Recurrence – 10 %
• Transient femoral nerve palsy : s
seen with excessive flexion during Pavlik bracing