Fractures Of The Femoral Neck
•Commonest site of fractures in the elderly
•The typical presentation: Caucasian women in their
seventh and eight decades
•Risk factors:
-Age\sex\race
-Osteoporosis (measure of age-related Osteoporosis)
-Bone weakening disorders (Osteomalacia, DM, Stroke,
Alcoholism, Chronic debilitating disease)
•Hip Osteoarthritis
Low incidence
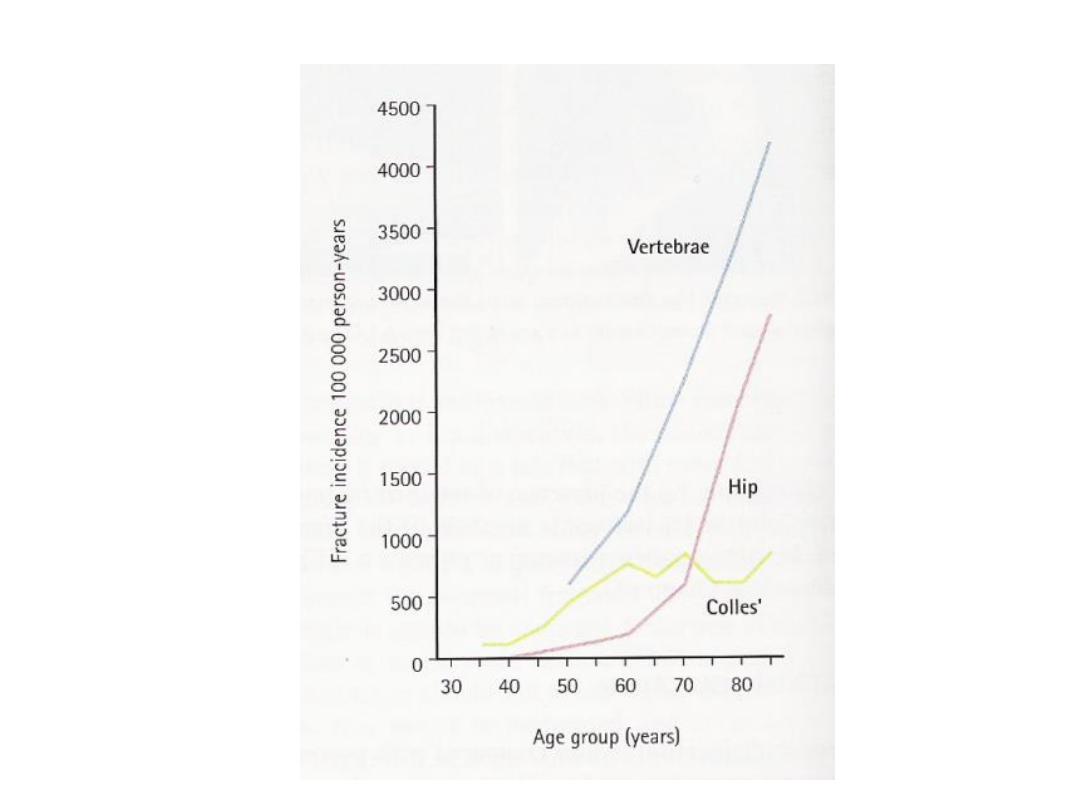
•Incidence of Osteoporotic fractures
• Mechanism of injury:
• Fall directly on the greater trochanter
• In Osteoporotic people less force is needed (catching a toe
in the carpet and twisting the hip into external rotation)
• Preceding stress fracture
• In young (Fall from a height or RTA)
• Pathological Anatomy and Classifications:
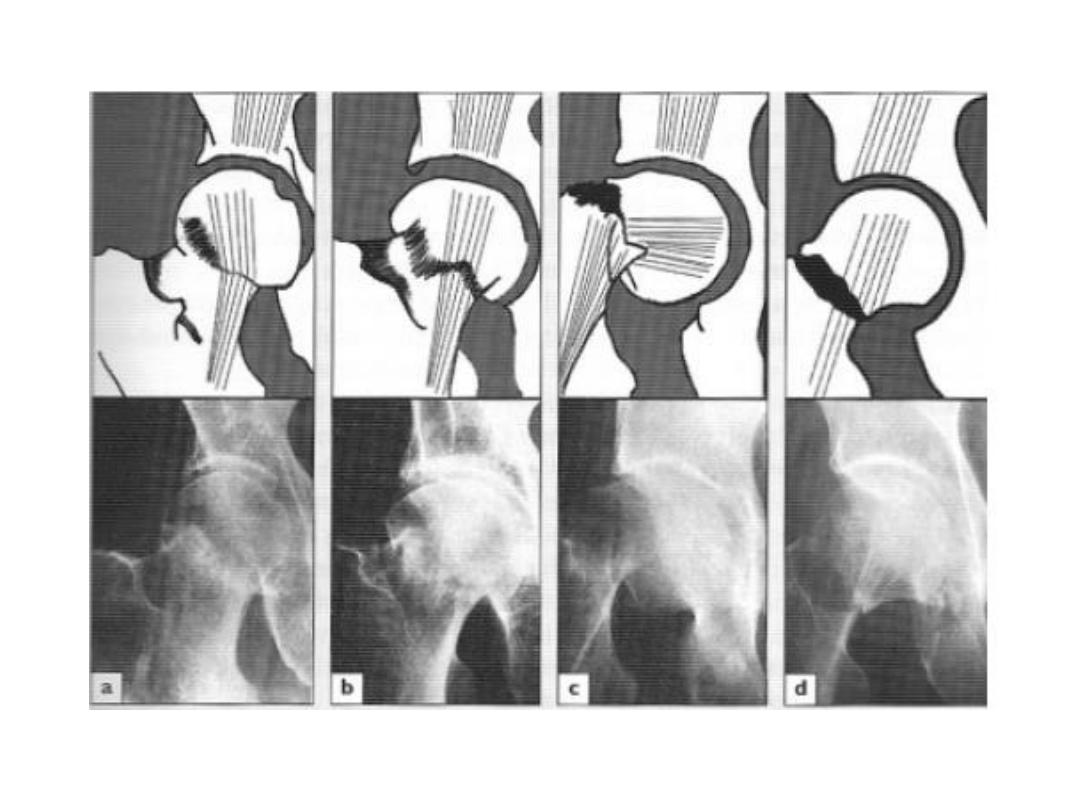
• Garden’s Classification:
• Based on the amount of displacement in the Pre-reduction
X-ray (Radiological)
• Stage І : Incomplete undisplaced Fracture (impacted or
abducted)
• Stage II : Complete undisplaced Fracture
• Stage ІІІ : Complete with moderate displacement
• Stage IV : Complete with severe Displacement
• Any downstage may progress to upstage if left untreated
• Two problems affect the healing process:
1-Bone ischemia
2-Tardy union

1-Bone ischemia:
-Femoral head blood supply:
a- Intramedullary vessels in the femoral neck (always
interrupted by the fracture)
b- Ascending cervical branches of the medial and lateral
circumflex anastomosis, which run within the capsular
retinaculum before entering the bone at the edge of the
femoral head (may be kinked or torn in displacement)
c-Vessels of the ligamentum teres (slight and 20% not
existent)
• Stage І & II better prognosis (Union and viability of
femoral head)
2- Tardy union:
-Intracapsular fracture
-Poor healing capacity:
A-Bone ischemia
B-Flimsy periosteum with no contact with soft tissue
C-Synovial fluid prevents clotting of hematoma
-Clinical Features:
-Hx of a fall followed by pain in the hip
-In displacement, the pt. lies with the limb in external
rotation and the legs looks short
-May not be so obvious:
*impacted one the pt may still be able to walk
*Debilitated and mentally handicapped pt. may not complain
at all
-Young adults with severe Lower limb injury should always be
examined for femoral neck fracture
• X-ray:
• Is there a fracture, and is it displaced?
• Usually Break is obvious but impacted one can be missed
• Displacement (abnormal shape of bone outline, mismatch
of the trabecular lines)
• Diagnosis:
• Straightforward or
• Four situation the fracture may be missed with bad
consequences:
1-Stress fractures:
-Should be considered in elderly pt. with unexplained hip pain
until proven otherwise.
- x-ray is normal, but Bone scan show hot lesion
2-Undisplaced fractures:
-Especially impacted one
-X-ray finding may be not obvious.
-Days later MRI and bone scan will show up the fracture
3-Painless fractures:
-Bedridden or fit patient
-If the context suggests an injury, investigate whether the pt.
complains or not
4-Multiple Fractures:
-Pelvis must be x-rayed
• Treatment
:
• Initial treatment: Pain relieving and simple splintage
• Operative treatment is almost mandatory, why?
1-Displaced fractures will not unite without internal fixation
2- It is safer to internally fixate Undisplaced fracture

Because there is always a risk to become displaced even while
lying in the bed
3-Old pts should be mobilized ASAP to prevent bedsores and
pulmonary complications
One exception is impacted fracture of old injury (walking for
weeks without deleterious effect)
• When should the operation be performed?
-In young: the op. is urgent (irreversible cellular changes after
12 hrs of ischemia)
-In elderly: The speed is tempered by the need for adequate
preparation, but the longer the delay the greater the risk of
complications

• What if the op. is considered too dangerous?
-The pt least fit for op. may need it most !!
• Despite the advancement of joint replacement, for most
pts the principles of treatment are as of old: accurate
reduction, secure internal fixation and early activity.
1- Reduction of displaced fractures:
• Under GA, closed reduction is done by applying traction
with the hip held in 45 of flexion and slight abduction; the
limb is then slowly brought into extension and finally
internally rotated; as traction is released, the fracture
reimpacts in the reduced position.
• The reduction is assessed by x-ray
• The stress trabeculae should be aligned to their nearly
normal position in both AP and Lateral views (acceptable
reduction is within 20 )
• If closed reduction failed:
<60 years: open reduction is advisable (Anterolat.
Approach).
>70 years: prosthetic replacement is preferable.
2-Fixation:
• The fracture is held with cannulated or a sliding screw and
a side-plate which attaches to the femoral shaft.
• Lateral incision is used

3-Early activity:
-From the first day, the pt should sit up in bed or in a chair and
encouraged to start walking using crutches or walker.
*Prosthetic replacement:
• The policy is to attempt reduction and fixation in all pts
aged under 75 years of age and to reserve replacement in
(1) Very old pts (2)pts in whom closed reductions fails
(3)pathological fractures
• Two types:
A- Uncemented femoral prosthesis or bipolar:
Least traumatic with post. approach
B-THR: preferable if:

1-Treatment has been delayed for some weeks and acetabular
damage is suspected
2-Metastatic disease or Paget’s disease
• Post-op early mobilization is important
• Speed of recovery depends largely on how active the pt
was before the fracture
• After 2-4 months, further improvement is unlikely.
• Complications:
• General:
• Mostly elderly
• Prone to DVT, PE, pneumonia and bedsores
• Aggravation of preexisting Disorders which causes death in
substantial proportion.
• Despite the advances in perioperative care the mortality
rate in elderly pts may be as high as 20% at 4 months after
injury
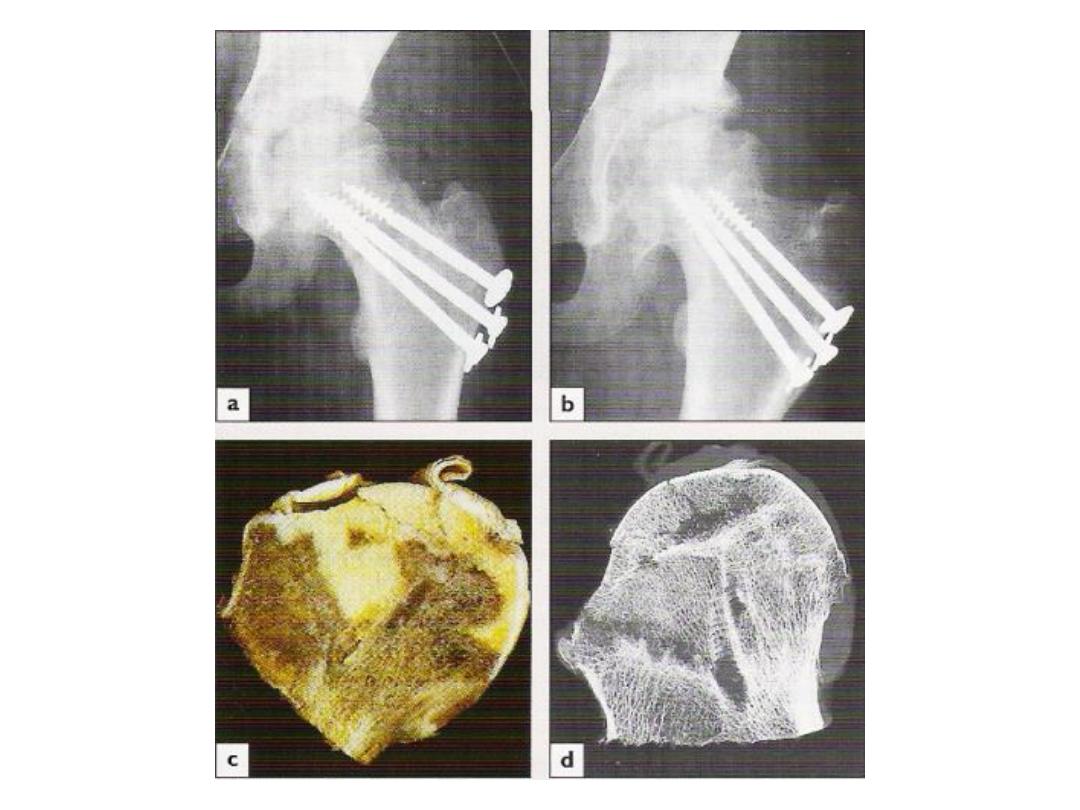
• Avascular necrosis (AVN):
• Necrosis of the femoral head:
-Displaced # 30%
-Undisplaced # 10%
• Occurs early at the time of injury, but the presentation is
late
• Collapse of the femoral head will cause pain and
progressive loss of function whether the # unites or not
• X-ray changes may not become apparent for months or
even years
• By using a nanocolloid scan, diminished vascularity may be
shown few weeks after injury
• Treatment:
• Older than 45 yrs
THR
• Younger Controversy
-Small necrotic segment Realignment/rotational
osteotomy
-Joint replacement (Hemi- or total) may be justified even in
this age group
• Osteoarthritis:
• AVN and femoral head collapse may lead ,after several
years, to secondary hip osteoarthritis
• THR is indicated when there is severe Loss of function
• Non-union:
• 30% of all femoral neck #
• High risk in severe displacement
• Causes:
-Poor blood supply
-Imperfect reduction
-Inadequate fixation -Tardy healing
• Treatment: depends on the cause of non union and the age
• Young:
(1) # unduly vertical + head alive subtrochantric
osteotomy + nail plate fixation changes # line to horizontal
(2)If reduction or fixation was faulty + No necrosis
REreduce and REfixate + bone graft across the fracture
(fibula or muscle pedicle graft)
(3)AVN Partial or THR according to the joint
• Elderly:
(1)If pain is condiderable Femoral head removal. And
if pt is fit THR is done
(2)If pain is bearable raising heel + stick and crutch
• Combined fractures of neck and shaft:
• High energy fractures in young people mostly
• Both # must be fixed
• Method of choice is to reduce and pin the femoral neck #
as usual and then fix the shaft with a plate and screws

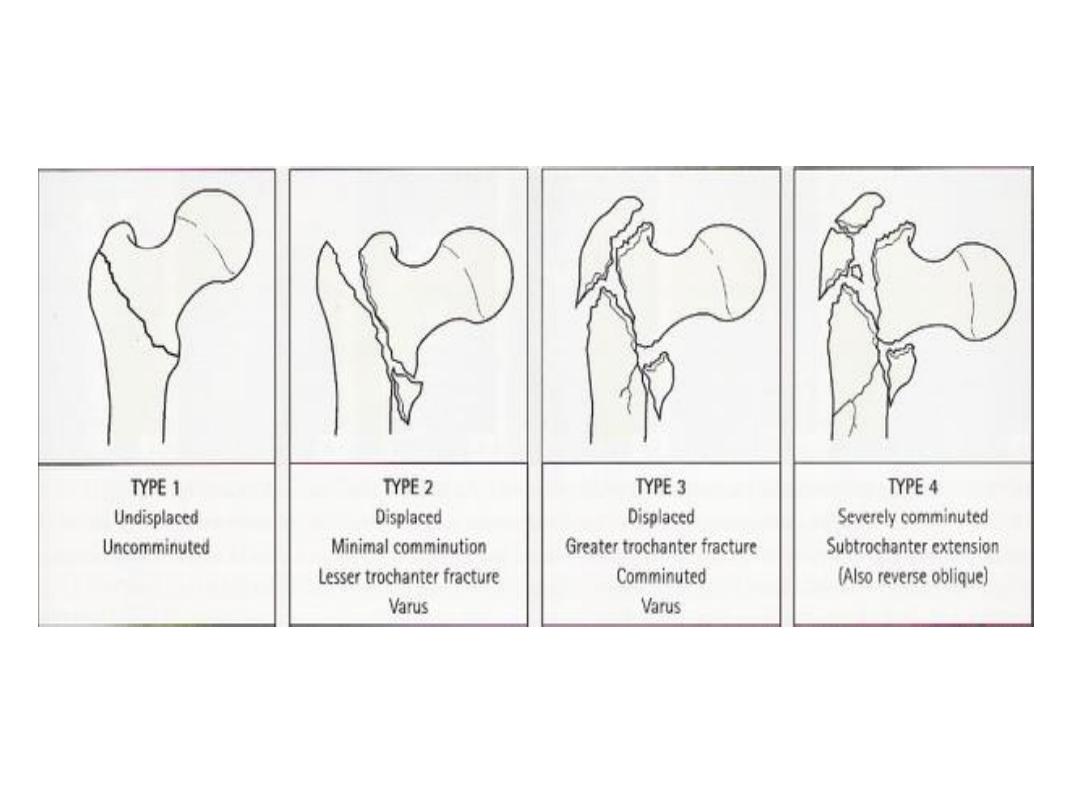
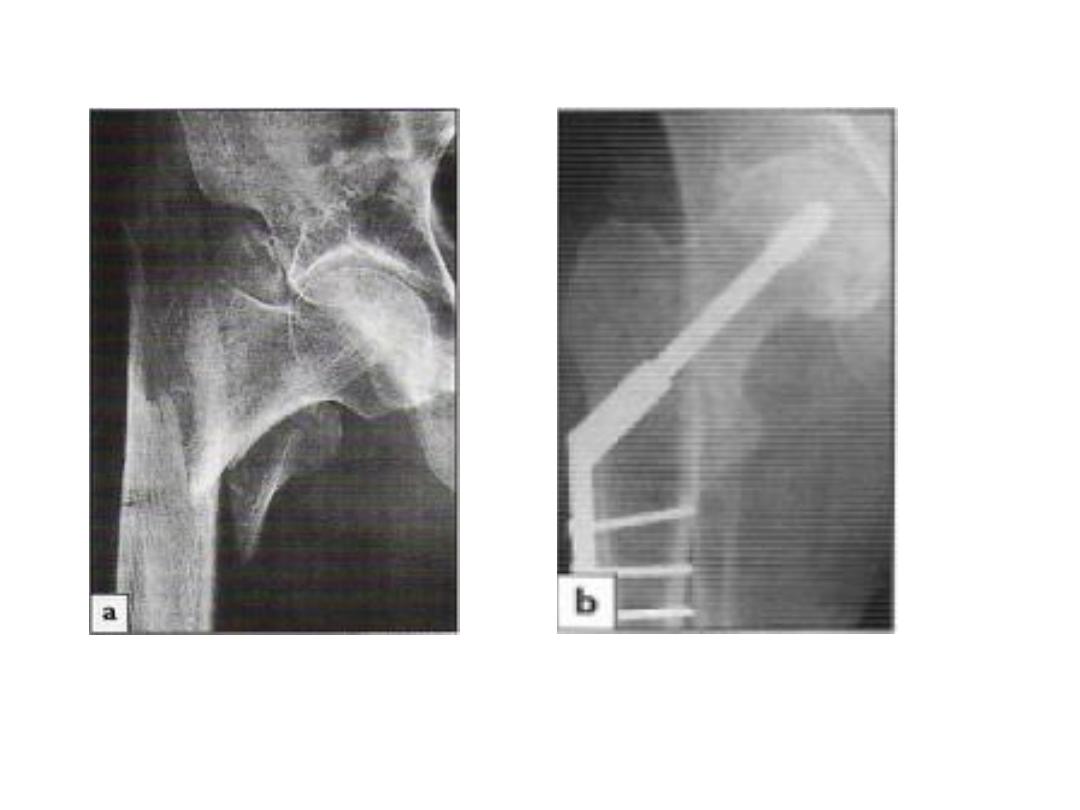
Intertrochantric fractures
• Extracapsular
• Same risk factors of the femoral neck fracture
• This fracture unites quite easily and seldom cause AVN
• Mechanism of injury:
• Fall directly into the greater trochanter or by indirect
twisting
• The proximal segment tends to displace in varus
• Pathological anatomy:
• Stable vs. unstable (contact between the fracture
segments, comminution and displacement by weight
bearing force)
• Kyle classification (increasing instability and difficulty of
reduction and fixation)
• Clinical features:
• Pain follow a fall, the pt. is unable to stand
• The leg is shorter and more externally rotated than femoral
neck #
• X-ray:
• The fracture usually runs diagonally from the greater to the
lesser trochanter
• It may be comminuted and severely displaced, but in some
cases the crack can hardly be seen
• Treatment:
• These fractures almost always treated by early internal
fixation although they unite quiet easily by conservative
treatment. That is to
1- Obtain the best possible position
2- Get the pt. up and walking ASAP and thereby reduce the
complications associated with prolonged recumbency
• Minimally displaced fractures are reduced by slight traction
and internal rotation, then confirmed by x-ray
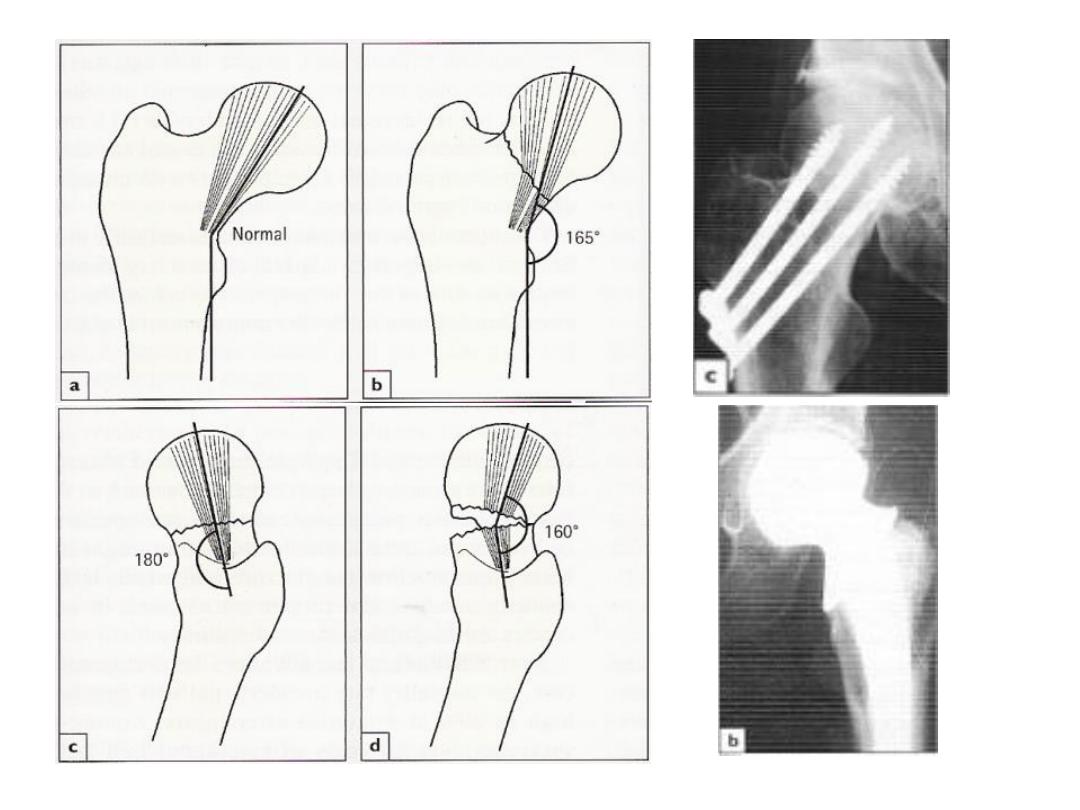
• The # Fixed with an angled device “sliding nail or screw”
that grips the femoral head and neck and is fixed to the
shaft with screws (making high angle 150)
Yet allows the bone fragments to impact during weight
bearing.
• With less common ‘Reversed oblique’ # 95 device or
intramedullary device gives more stable fixation
• Early activity (the day post-op), and partial weight bearing
ASAP
• Complications:
• Early:
• Late:
• Failed fixation:
• Screw may cut out of the osteoporotic bone if reduction is
poor.
• If union is delayed, the implant itself may break
• In either, reduction and fixation may have to be redone

•
Malunion
•
Varus and external rotation deformities are common
•
Fortunately, they are rarely severe and seldom interfere
with function
•
Non-union
•
If healing is delayed (beyond 6 months), mostly further
operation is advisable.
•
Pathological fracture:
•
Internal fixation is done in addition to cement packed in
the defect to improve stability.
•
If femoral neck involved, bone replacement with
cemented prosthesis may be preferable

Proximal Femoral Fractures In Children
• Hip fractures rarely occur in children
• They are potentially serious
• Due to high velocity trauma (falling, RTA)
• Pathological fractures sometimes occur through a bone
cyst or benign tumor
• Under 2 years, the probability of child abuse should be
considered
• The area between capital epiphysis and greater trochanter
is unusually vulnerable to injury
• Between 4 &8 years the ligamentum teres contribute very
little to the blood supply
• Delbet Classifications:
• Type І: is a fracture-separation of the epiphysis; sometimes
the epiphyseal fragment is dislocated from the acetabulum
• Type II: a transcervical fracture of the femoral neck, the
commonest (50%)
• Type III : is a basal (cervical-trochantric) #, the second
most common injury
• Type IV: Intertrochantric fracture.
• Treatment:
• These # should be treated as a matter of urgency, and
certainly within 24 hrs of injury
• Undisplaced fractures immobilization in a plaster
spica
• Displaced type IV closed reduction, traction and spica
immobilization.
• Type I,II and III fractures treated by closed reduction
and then internal fixation with smooth pins or cannulated
screws
• Complications:
• AVN:
• 30% of all cases
• Risk factors:
1-age more than 10 years
2-high velocity injury
3-Type I & II
4-Displacement
• Most pt. ends up with intrusive Pain and restriction of
movements
• X-ray changes usually appears within 3 months
• Arthrodesis may be advisable as late salvage procedure
• Coxa Vara:
• Femoral neck deformity may result from malunion , AVN or
premature physeal closure.
• Angle<120 then subtrochantric osteotomy will probably
needed

• Diminished growth
• Physeal damage
• Limb length equalization may later be needed

Subtrochanteric Fractures
• Occurs mostly with relatively trivial injury In an elderly pt.
with osteoporosis, osteomalacia or paget’s disease.
• Blood loss is greater than with femoral neck or trochanteric
# making healing slower
• Fracture healing is slow
• Clinical Features:
• Leg lies externally rotated & short
• thigh is markedly swollen.
• movement is painful
• X-ray:
• The # is through or below the lesser trochanter &
frequently comminuted.
• Treatment:
• Open reduction & internal fixation is treatment of choice
• Dynamic hip screw or intramedullary nailing
• Complications:
• Malunion
• Fairly common
• Usually in varus and external rotation
• May need operative treatment
• Non union
• 5%
• Operative treatmnet
Femoral Shaft Fractures
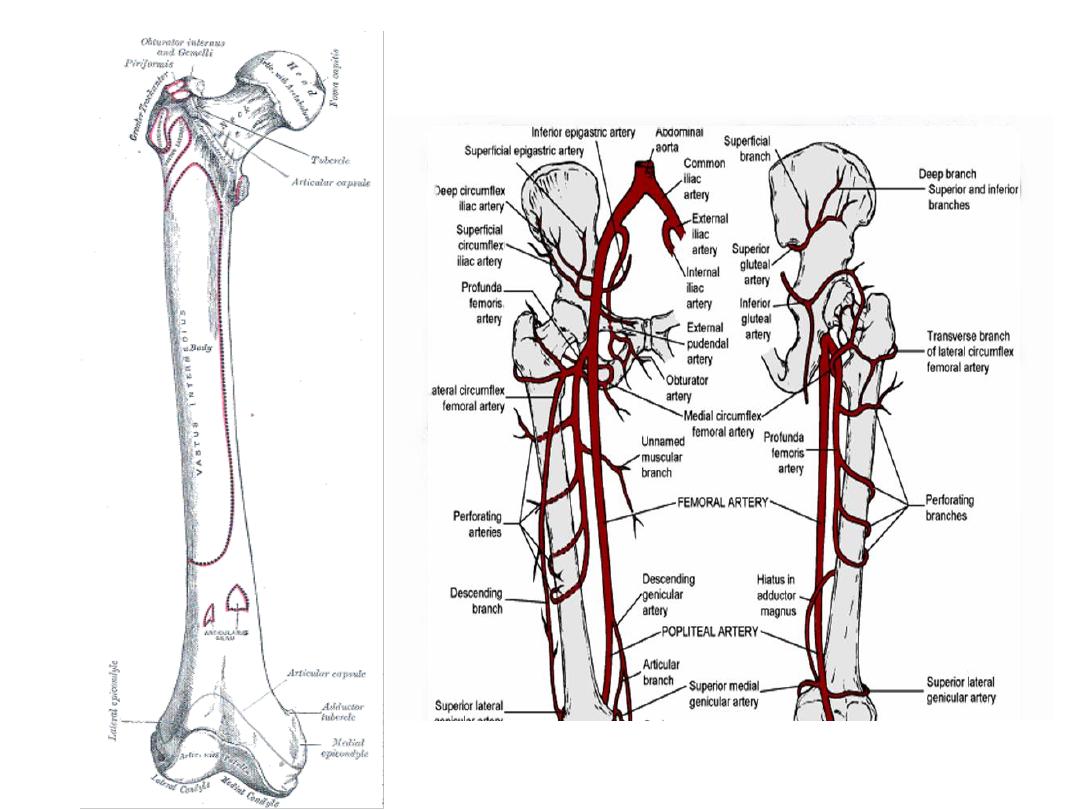
• Femoral shaft padded with powerful muscles
• Anatomy:
• Mechanism of injury:
• Young (usually) high energy injury
• Elderly pathological until proven otherwise
• Child
Keep in mind physical abuse
• Spiral (Fall)
• Transverse & oblique(angulation or direct force “RTA”)
• Comminuted & Segmental (severe violence “direct &
indirect”)
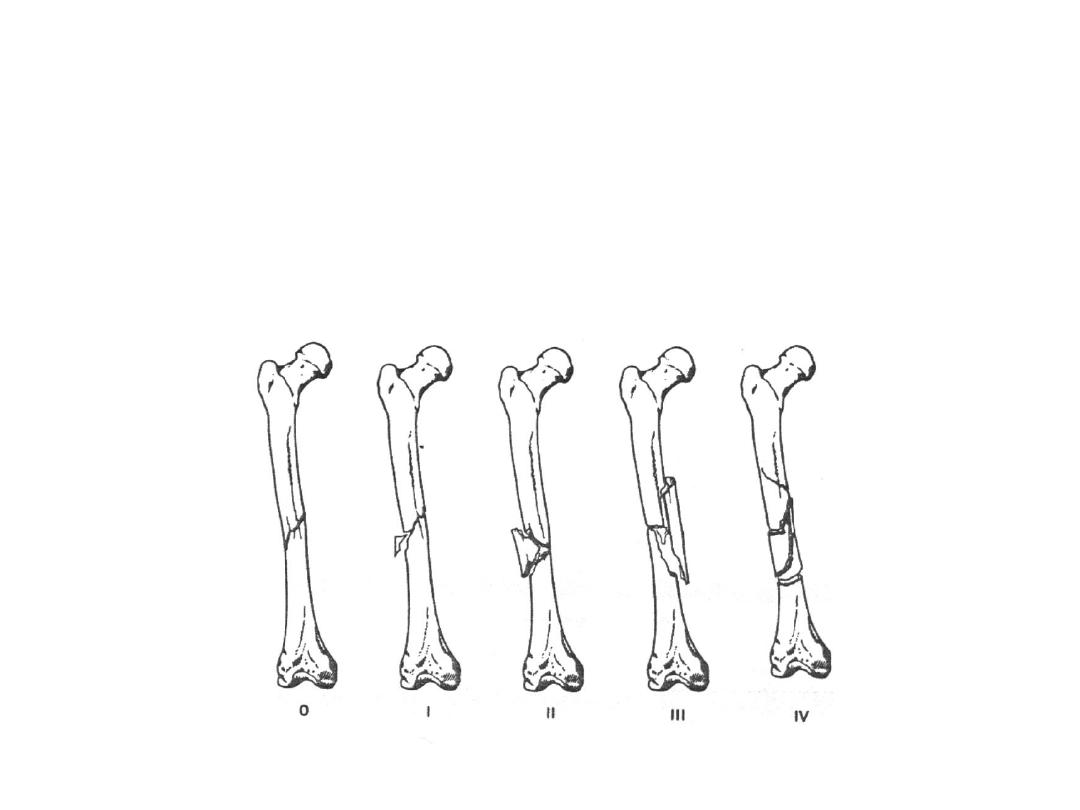
• Pathological anatomy:
• Some degree of comminution is present in most #
• Winquist classification (degree of soft tissue damage and
fracture instability increase with increasing grade of
comminution

• Displacement
1-Proximal #:
Proximal Seg. (flexion, abduction and
externally rotated) because of gluteus
medius and iliopsoas
Distal Seg (adducted)
2-Mid #:
Proximal Seg. ( flexion, external rotation, but
less abduction “mainly iliopsoas”)

3-Distal #:
Proximal Seg. (adduction)
Distal Seg, (flexion by gastrocnemius)
• Soft tissue injury is always present
• Bleeding may be severe (>1 L) from the perforater of
profunda femoris.
• Clinical features:
• Pain, Swelling & Deformity
• Neurovascular
• Other #
• Floating Knee
• X-ray:
• Never forget to x-ray the hip and Knee
• Baseline chest x-ray
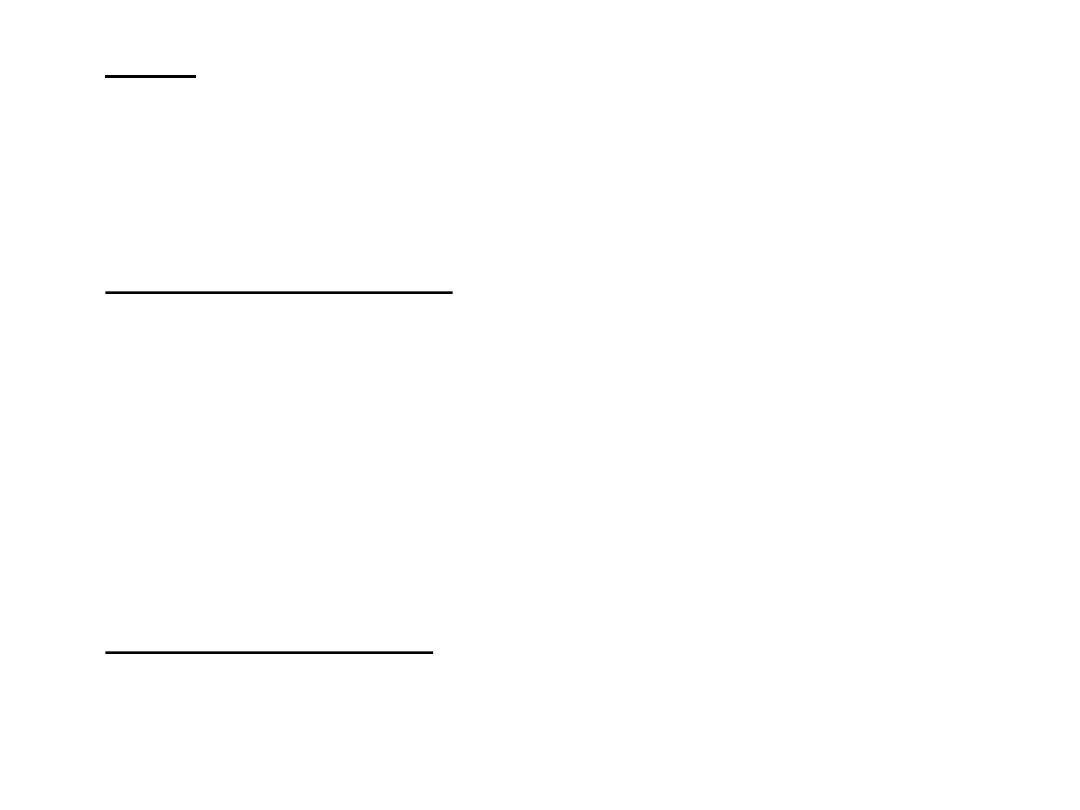
• Emergency treatment:
• Treat the shock
• Transport Splintage of # “Thomas’ splint”
• Once the pt is in the hospital, skin traction can be changed
to skeletal traction if op. treatment is to be delayed or if
non operative treatment is planned
• Definitive treatment:
• High energy trauma (fat embolism, ARDS, Multi organ
failure)
• Restore blood volume
• Stabilize the # early to decrease the systemic complications
• Most effective way is by locked intramedullary nailing
Traction & Bracing
• Can reduce and hold except the upper shaft #
• The disadvantage is the length of time spent in bed
• using plaster spica and functional bracing (Distal #) is
probable after 6-8 weeks of injury
• Main indications:
A-in children
B-Contraindication to anesthesia
C- Lack of suitable skills and facilities for fixation

• Adults: Skeletal traction through a pin or tightly strung K
wire behind the tibial tubercle. Traction (8-10 kg) is applied
over pulleys at the foot of the bed .
• Exercises are begun.
• Once the fracture was sticky (8 weeks), traction can be
discontinued and the pt. allowed to up and partial weight
bearing in a cast or a brace (distal #)
• Open reduction and plating:
• Accurate reduction & firm fixation
• High complication rate, including implant failure
• Main indication:
A-Shaft + femoral neck #
B-associated vascular injury

• Intramedullary nailing
• Method of choice for most
• External Fixation
• Advantages:
1-Union rate above 90% have been reported
2-As intramedullary nailling the fracture site is
not exposed and small amount of axial
movement can be fed to the bone by
allowing a telescoping action to occur in the
fixator body.

• Disadvantages:
1-pin site infection
2-pin loosening
3-Limitation of movements due to interference with
sliding structures if the half-pins are applied close to
the joint

• Main indications:
A-Severe open injuries
B-Multiple injuries
C-Femoral fractures in adolescence
D-Dealing with severe bone loss by bone transport
• Open fractures:
• I.V AB
• Wound cleansing and and debridement should be carried
out rapidly
• How to stabilize the fracture?
• This depends on the degree of contamination, amount of
soft tissue damaged and the length of time from the

injury to op
(1)If there is no obvious contamination, open fractures of all
degree up to IIIA (Gustilo Classification) can be treated as
closed one
(2)More severe injury should be left open and the fracture
stabilized by external fixator
• Complex injuries:
• # associated with vascular injury:
• Warning signs:
1-excessive bleeding or hematoma formation
2-Parathesia, pallor, pulselessness
• Doppler and arteriography
• The fracture should be stabilized as quickly as possible
(nailing, plating or external fixation)

• The vascular repair or bypass is then carried out
• Max 6 hrs
• # associated with knee injuries:
• Frequently the knee ligaments are injured
• As soon as the fracture is stabilized careful knee
examination and treatment should be done
• Floating knee
• # of tibia & Femur
• Fix Femur First
• # Associated with femoral neck injury
• Multiple injuries:
• Head and chest injuries take the priority
• Complications:
• Early
• Shock:
• 1-2 L of blood is lost
• Immediate transfusion
• Fat embolism and ARDS:
• Thromboembolism
• Prolonged traction in bed
• Movement and compression devices and
prophylactic anticoagulants are important for
prevention
• Infection
• Late:
• Delayed union and non-union:
• Should unite 100 days + or - 20 days
• Exchanging the nail +bone grafting
• Malunion
• Joint stiffness:
• Adhesions or injury to the joint
• Repeated evaluation & Early physiotherapy are imp.
• Refracture and implant failure
Femoral Shaft Fracture In Children
• Mechanism
• Quiet common
• Due to direct violence (RTA or fall)
• <2 years (child abuse)
• Pathological (local or diffuse bone disease)
• Treatmant:
• In young children open treatment is rarely necessary
• The choice of treatment largely depends on the age and
weight of a child

• Balanced traction and is used mostly
• Internal and external fixation is used in case of reduction
can not be achieved by traction (Older children with
multiple injuries)
• Complications:
• Shortening
• Overlapping and comminution
• Up to 1.5 cm is acceptable
• Malunion
• Angulation
• Rotation (not corrected by growth remodelling)
Supracondylar Fracture of femur
• Mechanism of injury:
• Direct violence as a result of high-energy trauma in young
• In osteoporotic elderly
• Clinical features:
• Knee is swollen & deformed, movement is painful
• You should check tibial pulse
• X-ray:
• The # is just above the femoral condyles,
but my extend
between them
• transverse or comminuted.
• The distal fragment is tilted backward thus risking injury To
the popliteal artery by the action of gastrocnemius
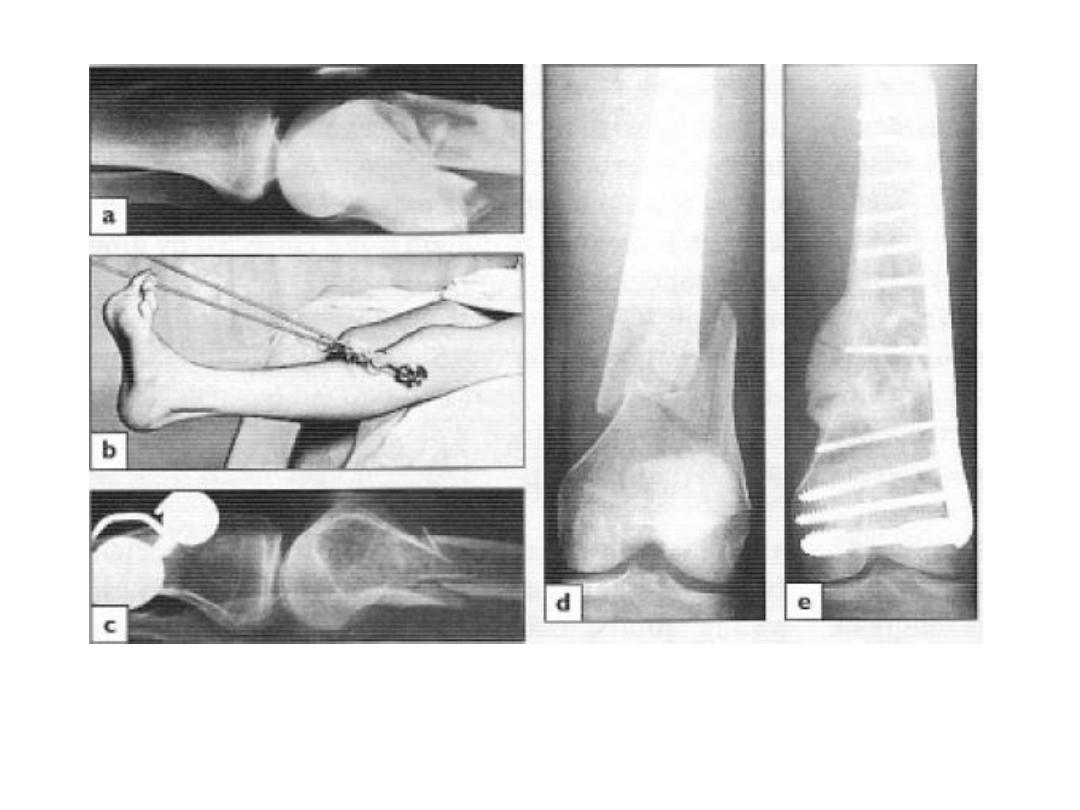
• Treatment:
• Non operative:
• If the # is only slightly displaced and exrtrarticular or if it
reduces easily with the knee in flexion, it can be treated by
traction (through tibia) & splintage
• If the distal fragment is displaced by gastrocnemius pull, a
second pin above the knee and vertical traction
will correct this.
• Operative:
• If closed reduction failed, open reduction & internal fixation
(with an angled compression device “dynamic condylar
screw and plate” or locked intramedullary nails) may be
successful
Complications
:
• Early:
• popliteal artery injury
• Small but definitive risk
• Late:
1-Knee stiffness
2-Non-union
Femoral Condyle Fracture
• Mechanism of injury:
• Ass. With supracondylar fractures
• In isolation due to direct injury Or a fall from a height may
drive the tibia upward into the intercondylar fossa
• Classification:
• Purely extra-articular (supracondylar #)
• Intra-articular # of one condyle usually the lateral
• Intra-articular bicondylar # which are effectively
supracondylar
• Clinical features:
• Knee is swollen & may be deformed, movement is painful
• There is a doughy tender feel characteristic of
haemarthrosis
• We should examine nerves and arteries
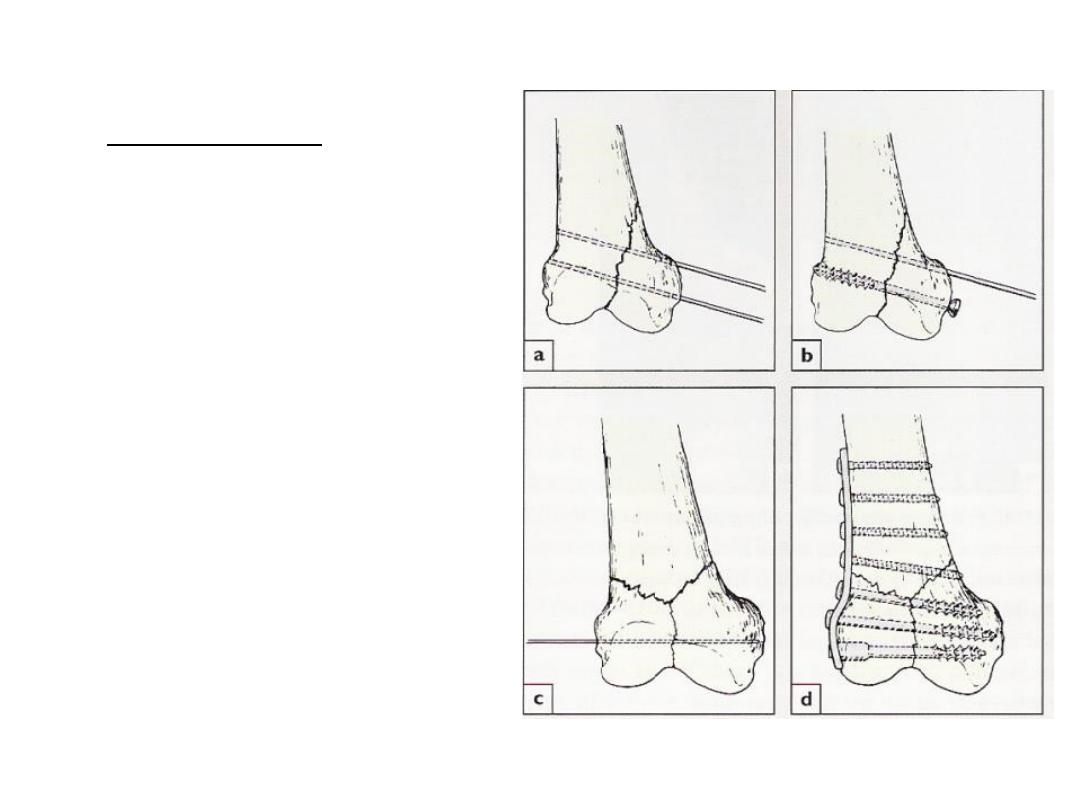
• Treatment:
• Aspirate the haemarthrosis
• Closed reduction is sometimes successful, if fails open
reduction is indicated (accurate reduction is important)
• The fragments are fixed with cannulated screws, a blade –
plate or a dynamic condylar screw and plate according to
the size of fragments
• Complication:
-Knee stiffness (common)
-Secondary OA

Thank you