Babylon University Stage Fourth
College of Medicine Lecture 3Dr. Athraa Falah
THE HEPATIC PATHOLOGY
CIRRHOSISCirrhosis is the twelfth most common cause of death in the United States, accounting for most liver-related deaths.
Classification of cirrhosis:
Primary(Cryptogenic Cirrhosis) 10%.
Secondary due to:
1-Alcohol abuse.
2-Chronic viral hepatitis.
3-Non-alcoholic steatohepatitis(NASH)
4-Biliary disease.
5-Iron overload
Cirrhosis is defined by three main morphologic characteristics:
•
Bridging fibrous septa in the form of delicate bands or broad scars linking portal tracts with one another and portal tracts with terminal hepatic veins.•
Parenchymal nodules containing hepatocytes encircled by fibrosis, with diameters varying from very small (<3 mm, micronodules) to large (several centimeters, macronodules). Nodularity results from cycles of hepatocyte regeneration and scarring.
•
Disruption of the architecture of the entire liver.
Pathogenesis.
The central pathogenic processes in cirrhosis are death of hepatocytes, extracellular matrix (ECM) deposition, and vascular reorganization.
-Activated kupffer cells lead to death and destruction of hepatocyte .
-Types I and III collagen are deposited in the space of Disse, creating fibrotic septal tracts.
-The vascular architecture of the liver is disrupted by the parenchymal damage and scarring, with the formation of new vascular channels in the fibrotic septa that connect the vessels in the portal region (hepatic arteries and portal veins) to terminal hepatic veins, shunting blood from the parenchyma.
The predominant mechanism of fibrosis is the proliferation of hepatic stellate cells and their activation into highly fibrogenic cells.
As they are converted into myofibroblasts, the cells release chemotactic and vasoactive factors, cytokines, and growth factors. Myofibroblasts are contractile cells, capable of constricting sinusoidal vascular channels and increasing vascular resistance within the liver parenchyma.
The stimuli for stellate cell activation may originate from several sources :
(a) Chronic inflammation, with production of inflammatory cytokines such as tumor necrosis factor (TNF), lymphotoxin, and interleukin 1β (IL-1β), and lipid peroxidation products;
(b) Cytokine and chemokine production by Kupffer cells, endothelial cells and hepatocytes
(c) Direct stimulation of stellate cells by toxins.
Throughout the process of liver damage and fibrosis, the surviving hepatocytes are stimulated to regenerate and proliferate as spherical nodules within the confines of the fibrous septa. The net outcome is a fibrotic, nodular liver in which delivery of blood to hepatocytes and the ability of hepatocytes to secrete substances into plasma are severely compromised. Disruption of the interface between the parenchyma and portal tracts may also obliterate biliary channels, leading to the development of jaundice.
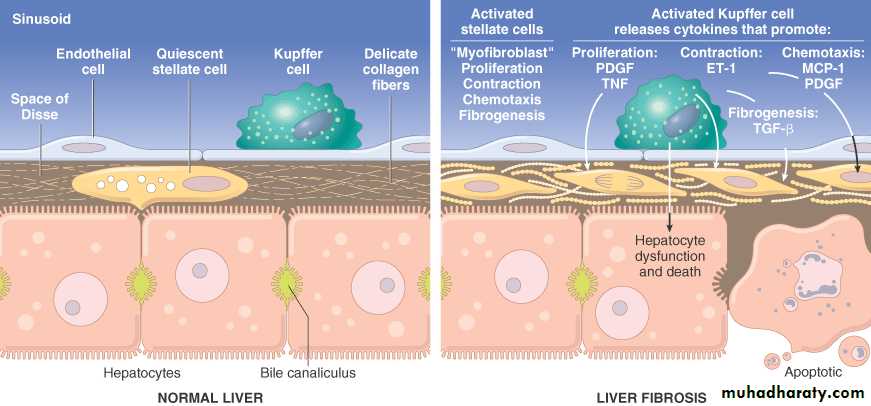
Schematic of Stellate cell activation and liver fibrosis. Kupffer cell activation leads to secretion of multiple cytokines. Platelet-derived growth factor (PDGF) and tumor necrosis factor (TNF) activate stellate cells, and contraction of the activated stellate cells is stimulated by endothelin-1 (ET-1). Fibrogenesis is stimulated by transforming growth factor β (TGF-β). Chemotaxis of activated stellate cells to areas of injury is promoted by PDGF and monocyte chemotactic protein-1 (MCP-1).
Clinical Features.
About 40% of individuals with cirrhosis are asymptomatic until late in the course of the disease. When symptomatic, they present with nonspecific clinical manifestations: anorexia, weight loss, weakness, and, in advanced disease, symptoms and signs of hepatic failure .
The ultimate mechanism of deaths in most cirrhotic patients is (1) progressive liver failure, (2) a complication related to portal hypertension, or (3) the development of hepatocellular carcinoma.
Metabolic Liver Disease
A distinct group of liver diseases is attributable to disorders of metabolism, either acquired or inherited. The most common acquired metabolic disorder is non-alcoholic fatty liver disease. Among inherited metabolic diseases, hemochromatosis, Wilson disease, and α1-antitrypsin deficiency are most prominent.Nonalcoholic Fatty Liver Disease (NAFLD)
NAFLD is a group of conditions that have in common the presence of hepatic steatosis (fatty liver), in individuals who do not consume alcohol, or do so in very small quantities (less than 20 g of ethanol/week).
NAFLD includes simple hepatic steatosis, steatosis accompanied by minor, non-specific inflammation, and non-alcoholic steatohepatitis (NASH).
Steatosis with or without non-specific inflammation is generally a stable condition without significant clinical problems.
In contrast, NASH is a condition in which there is hepatocyte injury that may progress to cirrhosis in 10% to 20% of cases. The main components of NASH are hepatocyte ballooning, lobular inflammation, and steatosis. With progressive disease fibrosis occurs.
NASH affects men and women equally and the condition is strongly associated with obesity, dyslipidemia, hyperinsulinemia and insulin resistance.
Pathogenesis.
The precise mechanisms are not entirely known, but genetics and environment play a role in the pathogenesis.
A “two-hit” model of pathogenesis has been proposed, encompassing two sequential events:
(1) hepatic fat accumulation and, (2) hepatic oxidative stress.
The oxidative stress acts upon the accumulated hepatic lipids, resulting in lipid peroxidation and the release of lipid peroxides, which can produce reactive oxygen species.
Clinical Features.
Individuals with simple steatosis are generally asymptomatic.
Serum AST and ALT are elevated in about 90% of patients with NASH. Despite the enzyme elevations, patients may be asymptomatic. Others have general symptoms such as fatigue and right-sided abdominal discomfort caused by hepatomegaly.
The current management strategy seeks to correct the underlying risk factors, such as obesity and hyperlipidemia, and to treat insulin resistance.
Benign neoplasms
Hepatic Adenoma
Benign neoplasms developing from hepatocytes are called hepatic adenomas or liver cell adenomas. Hepatic adenomas most frequently occur in young women who have used oral contraceptives; tumors generally regress if contraceptive use is terminated.
Hepatic adenomas have clinical significance for three reasons:
(1) When they present as an intrahepatic mass they may be mistaken for hepatocellular carcinomas;
(2) Subcapsular adenomas have a tendency to rupture, particularly during pregnancy (under estrogen stimulation), causing life-threatening intraperitoneal hemorrhage;
(3) Rarely, they may transform into carcinomas, particularly, when the adenoma arises in an individual with glycogen storage disease, and adenomas in which mutations of the β-catenin gene are present.
Pathogenesis.
The causal events are unknown, but it may be assosciated with
-Hormonal stimulation.
-Mutations in the genes encoding the transcription factor HNF1α and β-catenin .
-Multiple hepatic adenoma (adenomatosis) syndromes can occur in individuals with maturity-onset diabetes of young (MODY3), with HNF1 mutations.
Morphology.
Liver cell adenomas are pale, yellow tan, and frequently bile-stained nodules, found anywhere in the hepatic substance but often beneath the capsule. They may reach 30 cm in diameter. Although they are usually well demarcated, encapsulation might not be present. The tumor commonly presents as a solitary lesion, but multiple lesions can occur.
Histologically, liver cell adenomas are composed of sheets and cords of cells that may resemble normal hepatocytes or have some variation in cell and nuclear size. Portal tracts are absent; instead, prominent solitary arterial vessels and draining veins are distributed through the substance of the tumor.
MALIGNANT TUMORS
Malignant tumors occurring in the liver can be primary or metastatic. Primary carcinomas of the liver are relatively uncommon in North America and western Europe (0.5% to 2% of all cancers) but represent 20% to 40% of cancers in many other countries. Most primary liver cancers arise from hepatocytes and are termed hepatocellular carcinoma (HCC).
Hepatocellular Carcinoma (HCC)
It is the third most frequent cause of cancer deaths. About 82% of HCC cases occur in developing countries with high rates of chronic HBV infection, such as in southeast Asian and African countries; 52% of all HCC cases occur in China. There is a clear predominance of males.Pathogenesis.
Four major etiologic factors associated with HCC have been established:
-Chronic viral infection (HBV, HCV),
-Chronic alcoholism,
-Non-alcoholic steatohepatitis (NASH), and
-Food contaminants (primarily aflatoxins).
Other conditions include tyrosinemia, glycogen storage disease, hereditary hemochromatosis, non-alcoholic fatty liver disease, and α1-antitrypsin deficiency.
Many factors, including genetic factors, age, gender, chemicals, hormones, and nutrition, interact in the development of HCC.
The pathogenesis of HCC may be different in high-incidence, HBV-prevalent populations versus low-incidence Western populations, in which other chronic liver diseases such as alcoholism, non-alcoholic steatohepatitis, chronic HCV infection, and hemochromatosis are more common.
In .high-prevalence regions the HBV infection begins in infancy by the vertical transmission of virus from infected mothers, which confers a 200-fold increased risk for HCC development by adulthood. Cirrhosis may be absent in as many as half of these patients, and the cancer often occurs between 20 and 40 years of age.
In the Western world where HBV is not prevalent, cirrhosis is present in 75% to 90% of cases of HCC, usually in the setting of other chronic liver diseases. Thus, cirrhosis seems to be a prerequisite contributor to the emergence of HCC in Western countries but may have a different role in HCC that develops in endemic areas.
In China and southern Africa, where HBV is endemic, there may also be exposure to aflatoxin, a toxin produced by the fungus Aspergillus flavus, which contaminates peanuts and grains. Aflatoxin can bind covalently with cellular DNA and cause a specific mutation in codon 249 of p53 .
Although the precise mechanisms of carcinogenesis are unknown, several events have been implicated.
-Repeated cycles of cell death and regeneration, as occurs in chronic hepatitis lead to the accumulation of mutations during continuous cycles of cell division which may damage DNA repair mechanisms and eventually transform hepatocytes.
-Progression to HCC might result from point mutations in selected cellular genes such as KRAS and p53, and others .
-A subgroup of tumors expresses a high proportion of genes present in fetal liver and liver progenitor cells, suggesting that at least some HCCs may be generated from liver stem cells.
Universal vaccination of children against HBV in endemic areas can dramatically decrease the incidence of HBV infection, and most likely, the incidence of HCC.
Morphology.
HCC may appear grossly as (1) a unifocal (usually large) mass ; (2) multifocal, widely distributed nodules of variable size; or (3) a diffusely infiltrative cancer, permeating widely and sometimes involving the entire liver.
HCCs are usually paler than the surrounding liver, and sometimes take on a green colour when composed of well-differentiated hepatocytes capable of secreting bile. All patterns of HCCs have a strong propensity for invasion of vascular structures. HCC spreads extensively within the liver by obvious contiguous growth and by the development of satellite nodules.
Histologically HCCs range from well-differentiated to highly anaplastic undifferentiated lesions. In well-differentiated and moderately differentiated tumors, cells that are recognizable as hepatocytic in origin are disposed either in a trabecular pattern(cord like) or in an acinar, pseudoglandular pattern, sometimes with a central lumen.
In poorly differentiated forms, tumor cells can take on a pleomorphic appearance with numerous anaplastic giant cells, can be small and completely undifferentiated.
Clinical Features.
Most patients have ill-defined upper abdominal pain, malaise, fatigue, weight loss, and sometimes awareness of an abdominal mass or abdominal fullness. In many cases the enlarged liver can be felt on palpation, with sufficient irregularity or nodularity to permit differentiation from cirrhosis. Jaundice, fever, and gastrointestinal or esophageal variceal bleeding are inconstant findings.
Laboratory finding: Elevated levels of serum α-fetoprotein are found in 50% of persons with HCC.