Ovaries
Dr.Roaa S.MahdiPolycystic Ovarian syndrome (Stein-Leventhal syndrome)
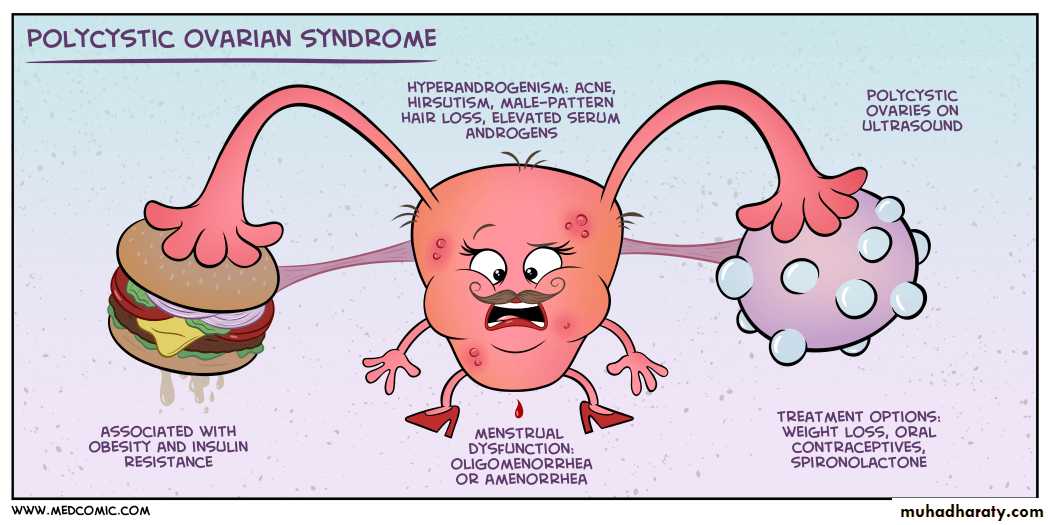
Oligomenorrhea, hirsutism, infertility, and sometimes obesity may appear in young women secondary to excessive production of androgens by multiple cystic follicles in the ovaries.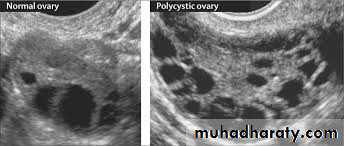

The ovaries are usually twice the normal size, gray-white with a smooth outer surface,& studded with subcortical cysts 0.5 to 1.5 cm in diameter.
Microscopically, there is a thickened, fibrotic tunica with underlying follicular cysts. Stigmata of previous ovulation are usually absent (corpora lutea or albicans).

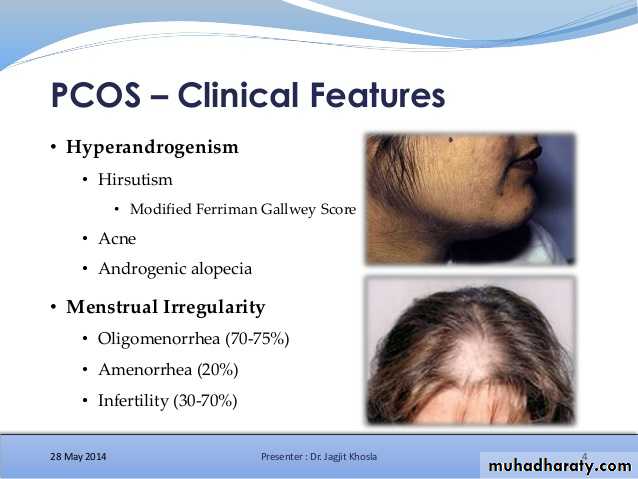
In most patients there are excessive production of androgens, high concentrations of luteinizing hormone, and low concentrations of follicle-stimulating hormone.
FSH
LH
Androgens
Insulin
TUMORS OF THE OVARY
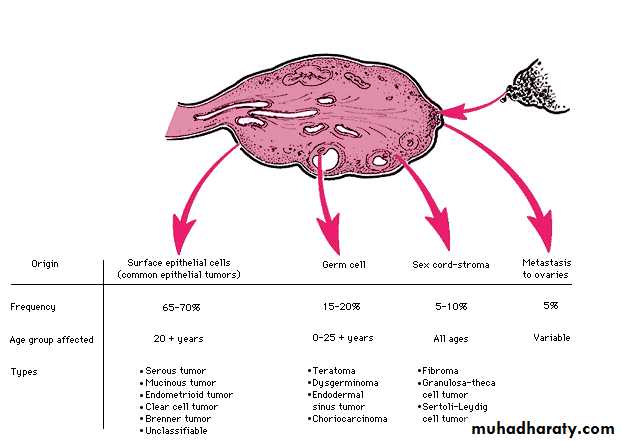
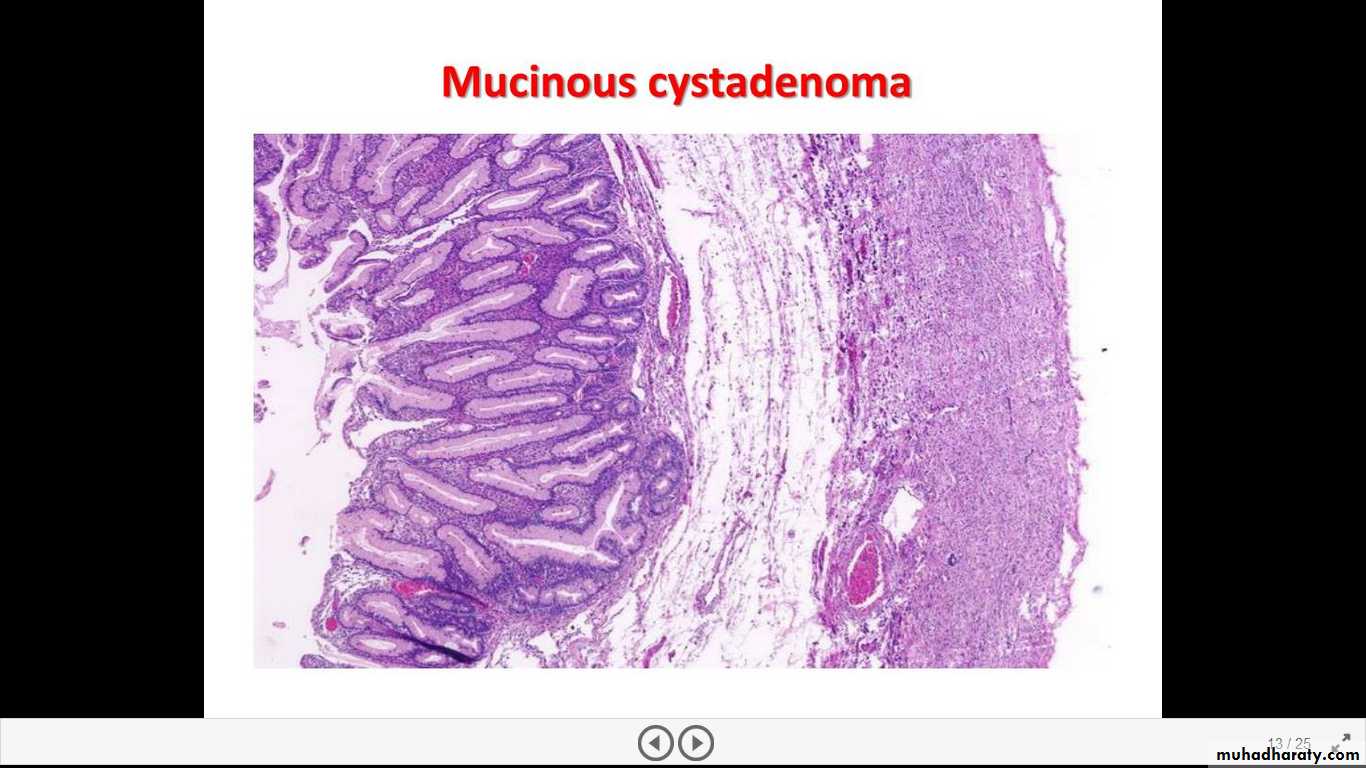
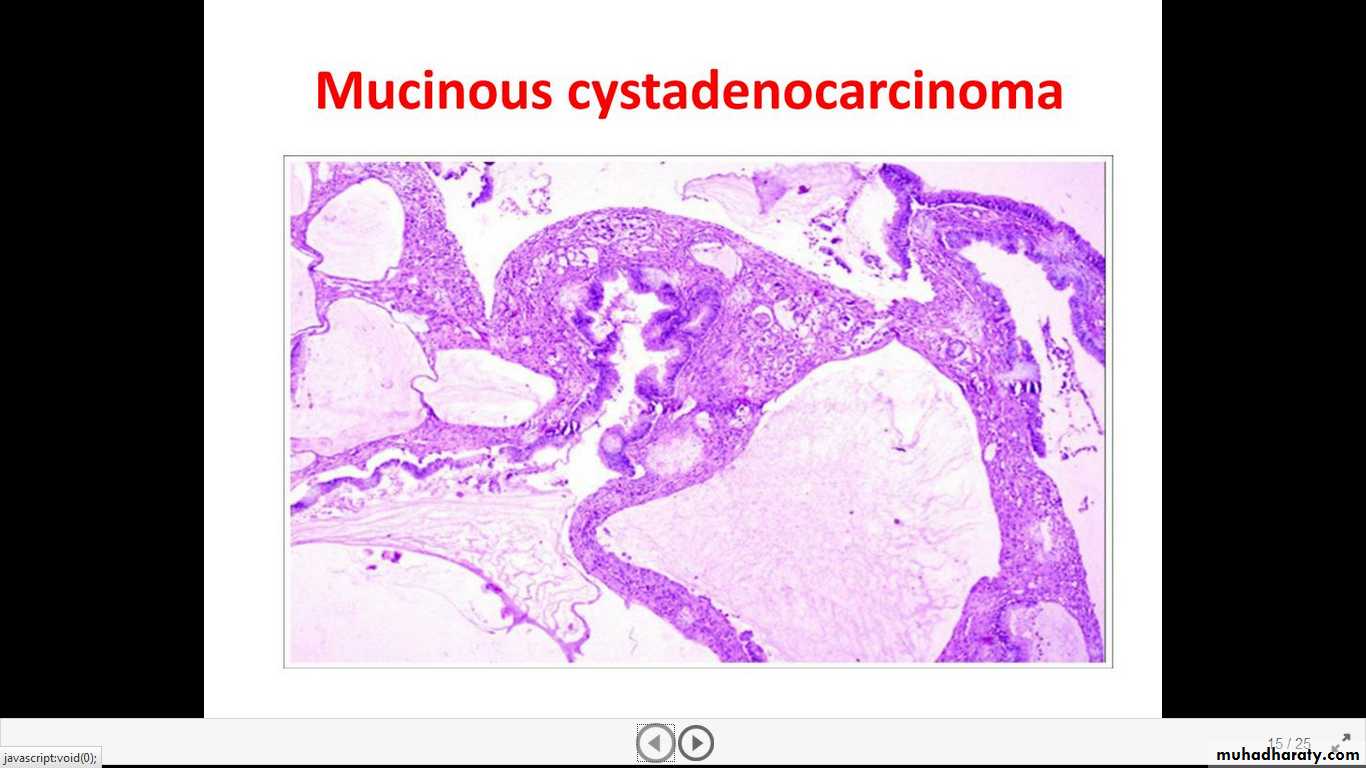
Ovarian cancer is the fifth leading cause of cancer death in women. Tumors of the ovary are diverse and this diversity is attributable to the three cell types that make up the normal ovary:
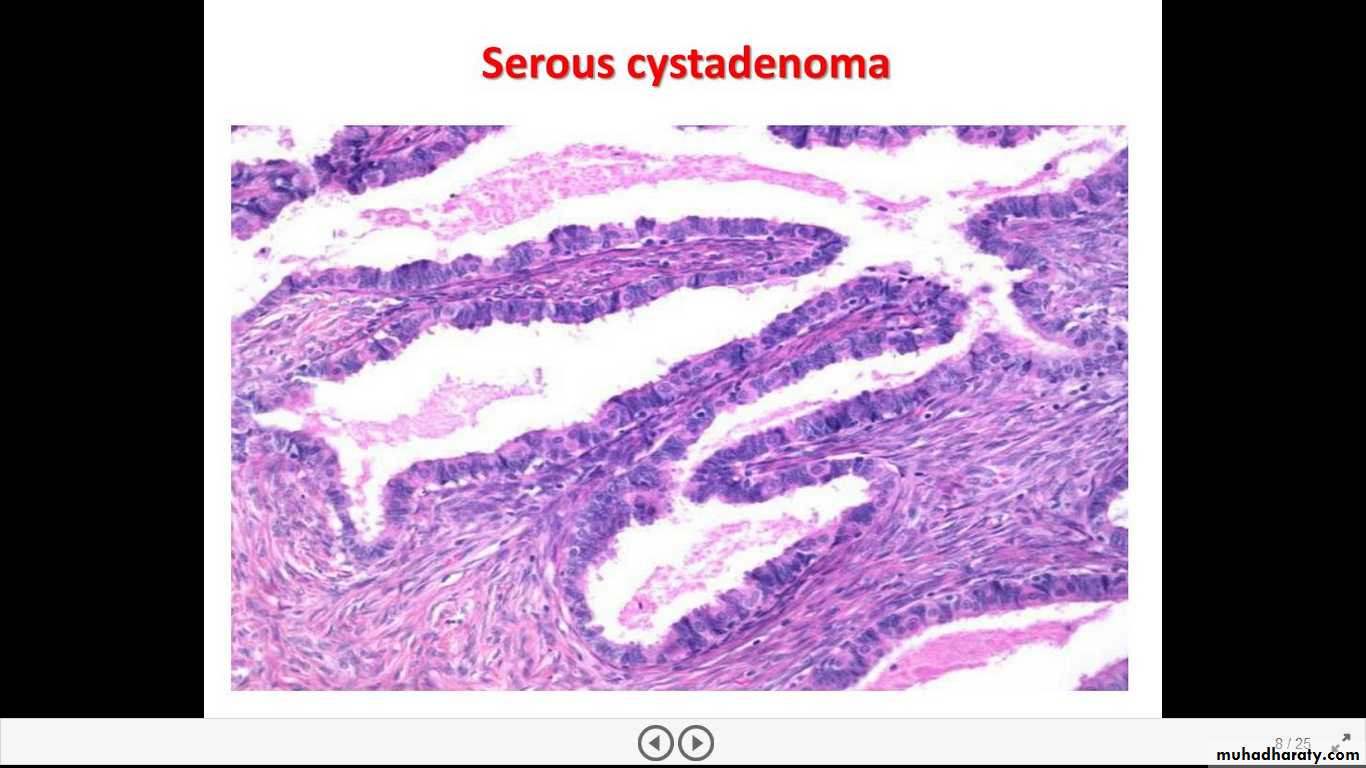
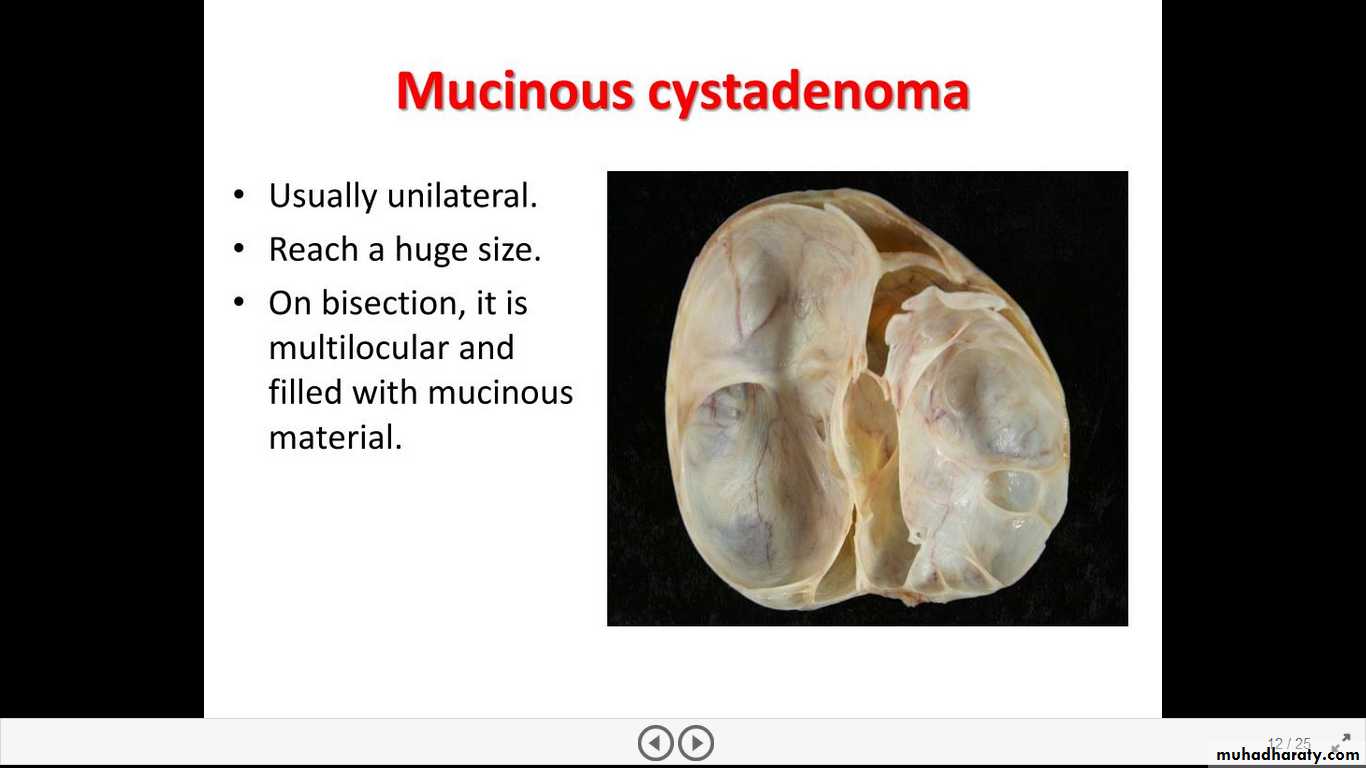
1. The surface (coelomic) covering epithelium
2. The germ cells
3. The sex cord/stromal cells.
Pathogenesis
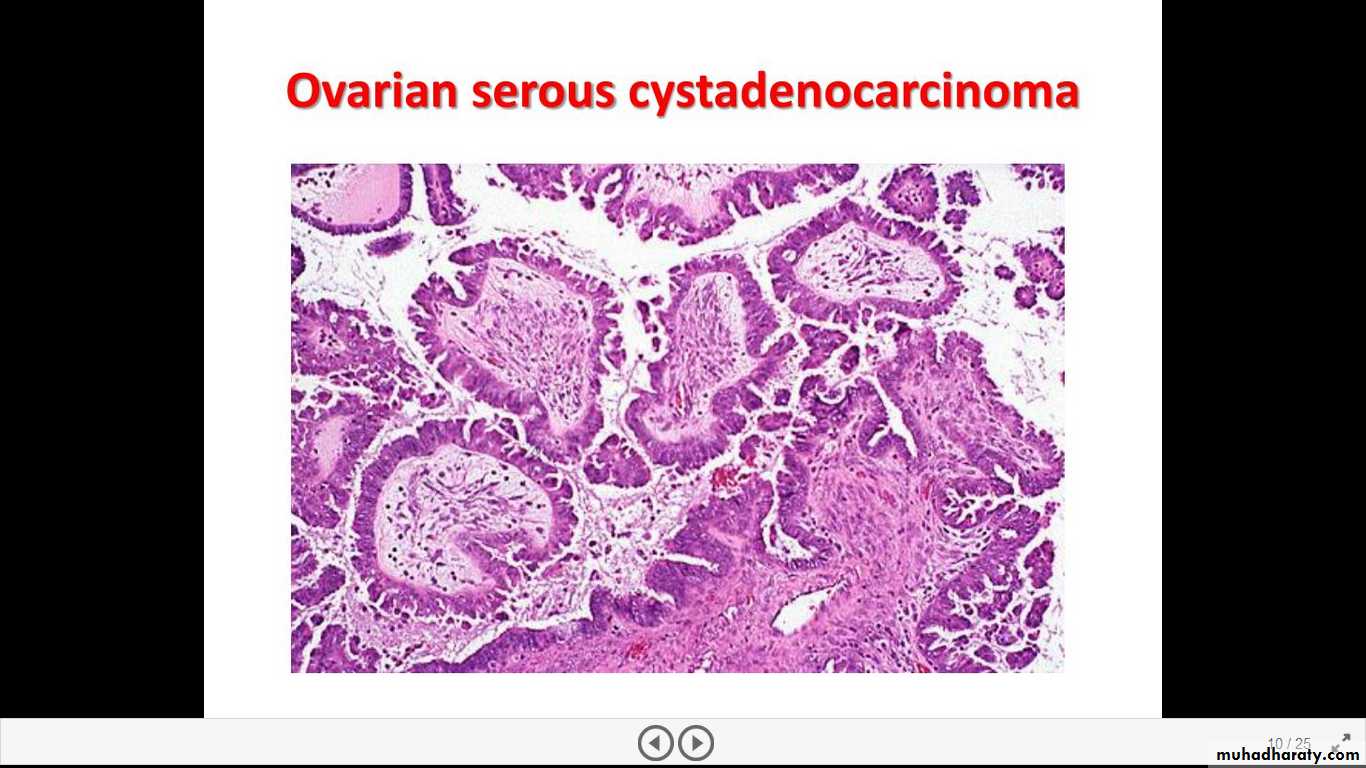
Nulliparity and family history are the two most important risk factors of epithelial ovarian cancers. There is a higher incidence of carcinoma in unmarried women and married women with low parity. Up to10% of ovarian cancers are familial; the majority of these hereditary cancers seem to be caused by mutations in BRCA1 and BRCA2 genes, these are also associated with hereditary breast cancer. Indeed, with mutations in these genes there is increased risk for both ovarian and breast cancers. Mutations in BRCA genes are also present in 10% of sporadic (nonfamilial) ovarian cancers. Other molecular changes of ovarian neoplasms include HER2/NEU & K-RAS proteins over-expression and p53 mutation. The latter is present in about 50% of all ovarian cancers.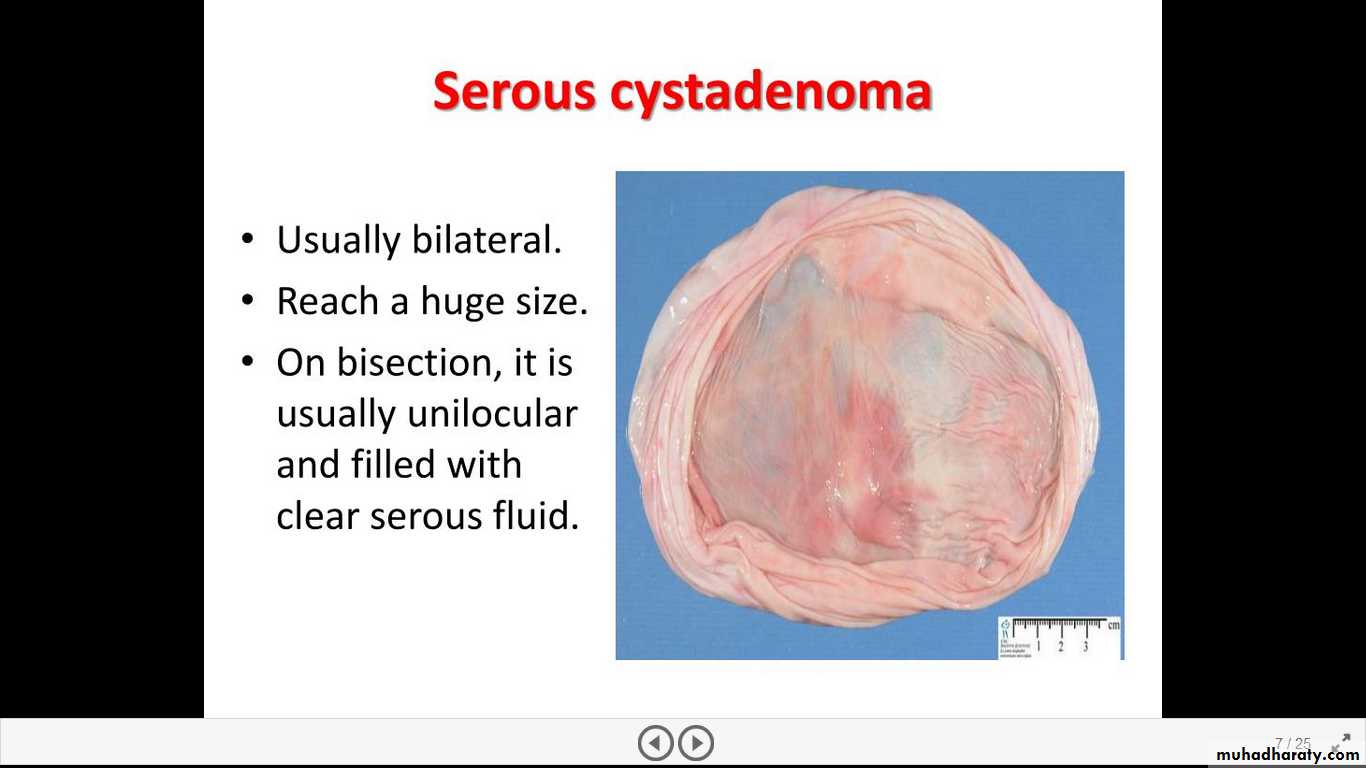

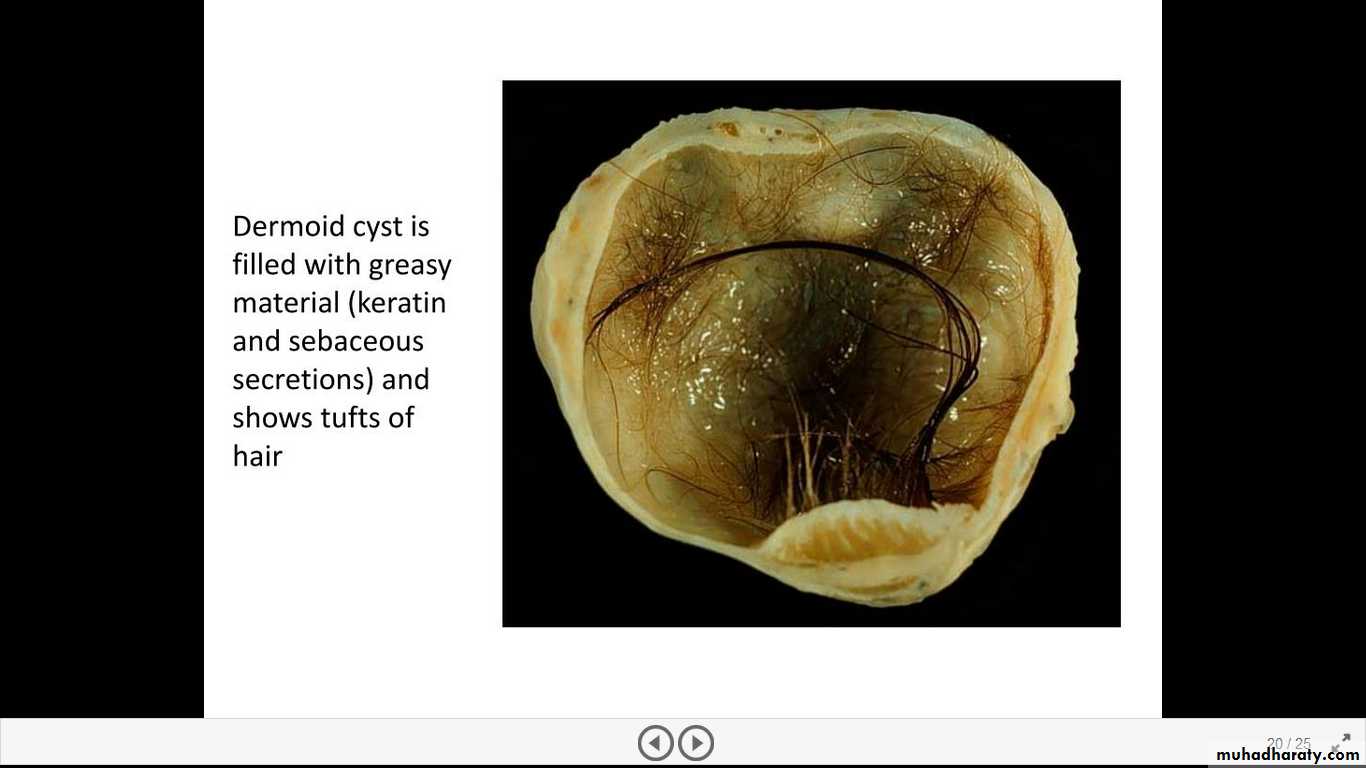
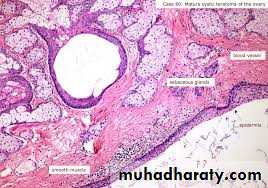
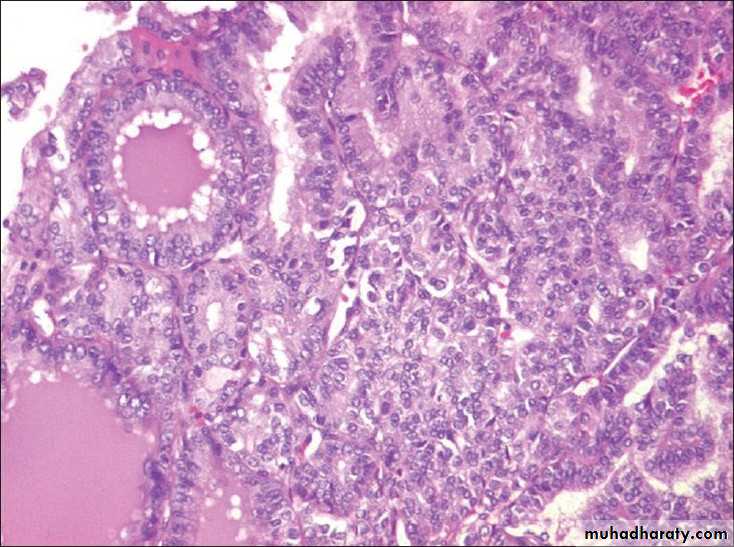
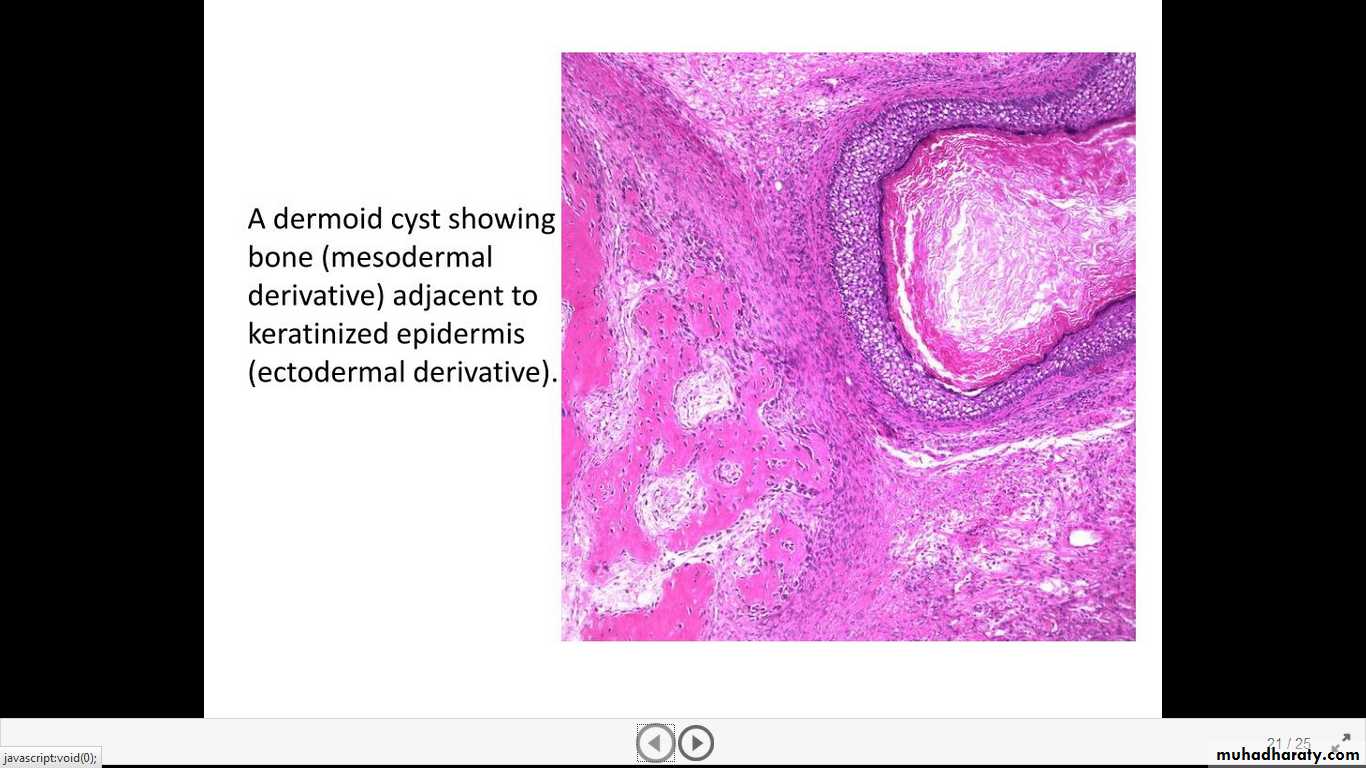
Benign (Mature) Cystic Teratomas are characterized by differentiation of totipotential germ cells into mature tissues representing all three germ cell layers: ectoderm, endoderm, and mesoderm. Usually there is the formation of a cyst lined by recognizable epidermis stuffed with adnexal appendages-hence the common designation dermoid cysts.





METASTASES TO OVARY are usually encountered in older ages. Mostly both ovaries are involved. Grossly there are solid gray-white masses as large as 20cm in diameter. Microscopically, there are malignant tumor cells arranged in cords or glands, and dispersed through a usually prominent fibroblastic background. Primaries include gastrointestinal tract, breast, and lung, & endometrium. When the infiltration is by mucin-containing signet ring cells the term Krukenberg tumor is applied. This is usually bilateral and nearly always of metastatic origin.
all ovarian neoplasms produce no symptoms or signs until they are well advanced.
local pressure symptoms (e.g., pain, gastrointestinal complaints, and urinary frequency)Larger masses, may cause an increase in abdominal girth.
Smaller masses, particularly dermoid cysts, sometimes become twisted on their pedicles (torsion), producing severe abdominal pain mimicking an "acute abdomen." Fibromas and malignant serous tumors often cause ascites
Elevations of the protein CA-125 have been reported in 75% to 90% of women with epithelial ovarian cancer. CA-125 measurements are of greatest value in monitoring response to therapy.
Clinical Correlations of ovarian cancers:
