By
Dr.Salah Aljanaby
Ass. Prof
General and Laparoscopic Surgeon
Lecture 1
thyroid gland
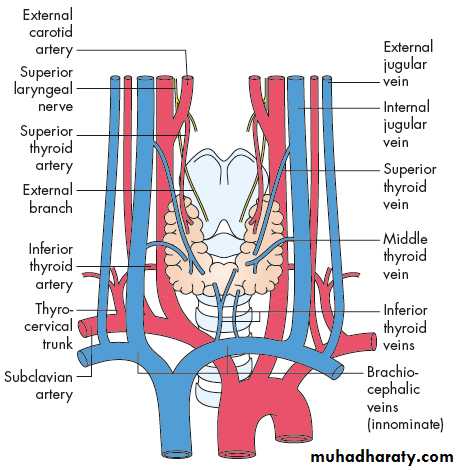
SURGICAL ANATOMY
The normal thyroid gland weighs 20–25 g.The arterial supply is rich, and extensive anastomoses occur between the main thyroid arteries and branches of the tracheal and esophageal arteries
There is an extensive lymphatic network within the gland. Although some lymph channels pass directly to the deep cervical nodes, the subcapsular plexus drains principally to the central compartment juxtathyroid – ‘Delphian’– and paratracheal nodes and nodes on the superior and inferior thyroid veins (level VI), and from there to the deep cervical (levels II, III, IV and V) and mediastinal groups of nodes (level VII)
The normal parathyroid gland weighs up to 50 mg
orange/brown colour
Most adults have four parathyroid glands
• PHYSIOLOGY
ThyroxineThe hormones tri-iodothyronine (T3) and l-thyroxine (T4) are bound to thyroglobulin within the colloid. Synthesis within the thyroglobulin complexis controlled by several enzymes, in distinct steps:
• trapping of inorganic iodide from the blood;
• oxidation of iodide to iodine;
• binding of iodine with tyrosine to form iodotyrosines;
• coupling of monoiodotyrosines and di-iodotyrosines to form T3 and T4.
When hormones are required, the complex is resorbed into the cell and thyroglobulin is broken down. T3 and T4 are liberated and enter the blood, where they are bound to serum proteins: albumin, thyroxine-binding globulin (TBG) and thyroxinebinding prealbumin (TBPA). The small amount of hormone that remains free in the serum is biologically active.
The metabolic effects of the thyroid hormones are due to unbound free T4 and T3 (0.03 and 0.3 per cent of the total circulating hormones, respectively). T3 is the more important physiological hormone and is also produced in the periphery by conversion from T4. T3 is quick acting (within a few hours),
whereas T4 acts more slowly (4–14 days).
Parathormone
The parathyroid glands secrete the 84-amino acid peptide parathyroidhormone (PTH), which controls the level of serum calcium in extracellular fluid
PTH is released in response to a low serum calcium or high serum magnesium level. PTH activates osteoclasts to resorb bone, and increases calcium reabsorption from urine and renal activation of vitamin D with subsequent increased gut absorption of calcium. Renal excretion of phosphate is also increased.
Calcitonin
The parafollicular C cells of the thyroid are of neuroendocrine origin and arrive in the thyroid via the ultimobranchial bodyThey produce calcitonin which is a serum marker for recurrence of medullary thyroid cancer.
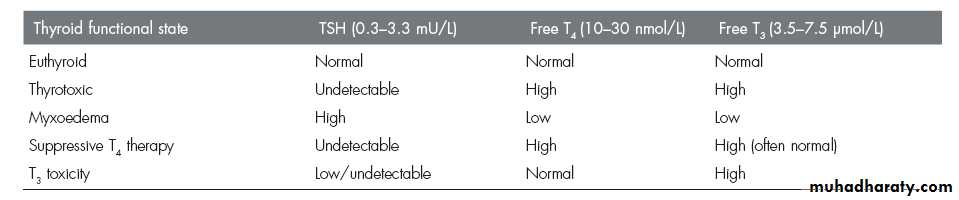
The pituitary–thyroid axis
Synthesis and liberation of thyroid hormones from the thyroid is controlled by thyroid-stimulating hormone (TSH) from the anterior pituitary.
Secretion of TSH depends upon the level of circulating thyroid hormones and is modified in a classic negative feedback manner.
In hyperthyroidism, when hormone levels in the blood are high, TSH production is suppressed whereas in hypothyroidism it is stimulated. Regulation of TSH secretion
also results from the action of thyrotrophin-releasing hormone (TRH) produced in the hypothalamus.
Thyroid-stimulating antibodies
A family of IgG immunoglobulins bind with TSH receptor sites (TRAbs) and activate TSH receptors on the follicular cell membrane.They have a more protracted action than TSH (16–24 versus 1.5–3 hours) and are responsible for virtually all cases of thyrotoxicosis not due to autonomous toxic nodules. Serum concentrations are very low but their measurement is not essential
to make the diagnosis
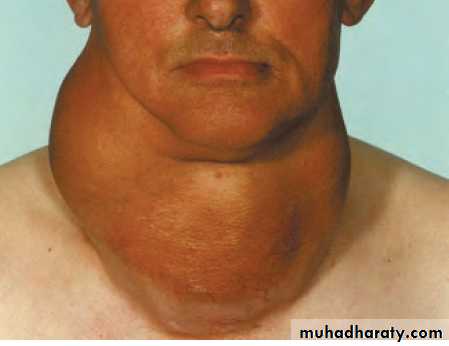
THYROID ENLARGEMENT
The normal thyroid gland is impalpable.Goitre is generalised enlargement of the thyroid gland
Isolated (solitary )swelling is discrete swelling (nodule) in one lobe with no palpable abnormality elsewhere
Dominant swelling is discrete swellings with evidence of abnormality elsewhere in the gland
Classification of thyroid swellings
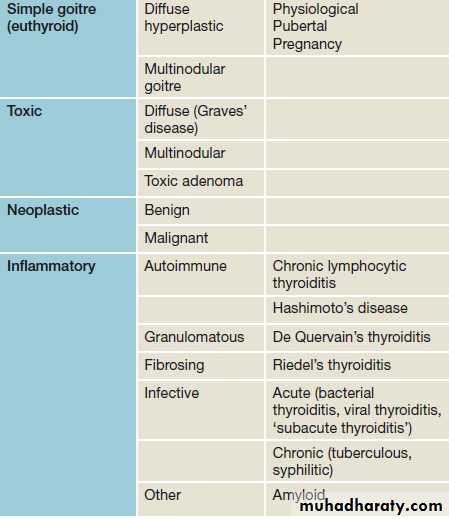
Simple goitre
Aetiologystimulation of the thyroid gland by TSH,
inappropriate secretion from a microadenoma in the anterior pituitary (which is rare),
chronically low level of circulating thyroid hormones.
The most important factor in endemic goitre is dietary deficiency of iodine
defective hormone synthesis probably accounts for many sporadic goitres
The natural history of simple goitre
Stages in goitre formation are:●● Persistent growth stimulation causes diffuse hyperplasia; all lobules are composed of active follicles and iodine uptake is uniform. This is a diffuse hyperplastic goitre, which may persist for a long time but is reversible if stimulation ceases.
●● Later, as a result of fluctuating stimulation, a mixed pattern develops with areas of active lobules and areas of inactive lobules.
●● Active lobules become more vascular and hyperplastic until haemorrhage occurs, causing central necrosis and leaving only a surrounding rind of active follicles.
●● Necrotic lobules coalesce to form nodules filled either with iodine-free colloid or a mass of new but inactive follicles.
●● Continual repetition of this process results in a nodular goitre. Most nodules are inactive, and active follicles are present only in the internodular tissue.
Diagnosis
The patient is euthyroid,The nodules are palpable and often visible; they are smooth, usually firm and not hard
Goitre is painless and moves freely on swallowing.
Hardness and irregularity, due to calcification, may simulate carcinoma.
A painful nodule, sudden appearance or rapid enlargement of a nodule raises suspicion of carcinoma but is usually due to haemorrhage into a simple nodule.
Differential diagnosis from autoimmune thyroiditis may be difficult and the two conditions frequently coexist.
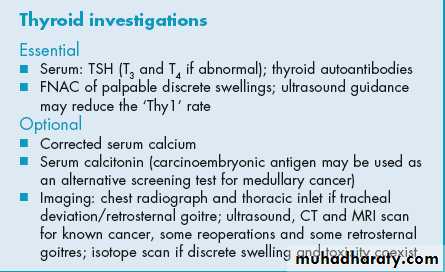
Investigations
Thyroid function should be assessed to exclude mild hyperthyroidism,
Thyroid antibodies tested to differentiate from autoimmune thyroiditis.
Ultrasound is the gold standard assessment
FNAC is only required for a nodule within the goitre that demonstrates ultrasonic features of concern. The biopsy should be performed under ultrasonic guidance to ensure the correct nodule is sampled.
CT scan of the thoracic inlet is the best modality to assess tracheal or oesophageal compression.
Complications
Tracheal obstructionmay be due to gross lateral displacement or compression in a lateral or anteroposterior plane by retrosternal extension of the goitre
SECONDARY THYROTOXICOSIS
Transient episodes of mild hyperthyroidism are common, occurring in up to 30% of patients.CARCINOMA
An increased incidence of cancer (usually follicular) has been reported from endemic areas.
Prevention and treatment of simple goitre
In endemic areas the incidence of goitre has been strikingly reduced by the introduction of iodised salt.In the early stages, a hyperplastic goitre may regress if thyroxine is given in a dose of 0.15–0.2 mg daily for a few months.
Although the nodular stage of simple goitre is irreversible, more than half of benign nodules will regress in size over 10 years.
Most patients with multinodular goitre are asymptomatic and do not require operation.
Surgery is indicated for nodular goitres
1. features of underlying malignancy
2. swallowing symptoms i
3. cosmetic reasons i
4. tracheal compression
There is a choice of surgical treatment in multinodular goitre:
Total thyroidectomy
with immediate and lifelong replacement of thyroxine
. Subtotal thyroidectomy
partial resection of each lobe removing the bulk of the gland, leaving up to 8 g of relatively normal tissue in each remnant.
Multinodular goitre
Clinically discrete swellings
commonpalpable in 3–4% of the adult population
three to four times more frequent in women than men.
Diagnosis
. About 70% of discrete thyroid swellings are clinically isolated and about 30% are dominant.The importance of discrete swellings lies in the risk of neoplasia compared with other thyroid swellings.
15% of isolated swellings prove to be malignant and an additional 30–40% are follicular adenomas.
The remainder are non-neoplastic, largely consisting of areas of colloid degeneration, thyroiditis or cysts.
Investigation
THYROID FUNCTION
If hyperthyroidism ‘toxic adenoma’ or toxic multinodular goitre.
The combination of toxicity and nodularity is indication for isotope scanning to localise the area(s) of hyperfunction.
AUTOANTIBODY TITRES
chronic lymphocytic thyroiditis.
ISOTOPE SCAN
except when toxicity is associated with nodularity.
ULTRASONOGRAPHY
ultrasonic features in a thyroid swelling associated with thyroid neoplasia, including microcalcification and increased vascularity, but only macroscopic capsular breach and nodal involvement are diagnostic of malignancy.
FINE-NEEDLE ASPIRATION CYTOLOGY
FNAC should be used, ideally under ultrasound guidance, . FNAC is reliable in identifying papillary thyroid cancer but cannot distinguish between a benign follicular adenoma and follicular carcinoma, as this distinction is dependent not on cytology but on histological criteria, which include capsular and vascular invasion. FNAC is both highly specific and sensitive.
RADIOLOGY
Plain films have previously been used to assess tracheal compression and deviationCT scanning is also useful if ultrasound has identified metastatic disease in the neck as it can assist surgical planning and also assess the superior mediastinum and lungs
LARYNGOSCOPY
Flexible laryngoscopy has rendered indirect laryngoscopy obsolete and is widely used preoperatively to determine the mobility of the vocal cords. The presence of a unilateral cord palsy coexisting with an ipsilateral thyroid nodule of concern is usually diagnostic of malignant disease.
CORE BIOPSY
rarely indicated in thyroid massesuseful in the rapid diagnosis of widely invasive malignant disease, for example anaplastic carcinoma, or in the diagnosis of lymphadenopathy.
The main indication for operation is the risk of neoplasia, which includes follicular adenoma as well as malignant swellings.
50% of isolated swellings and 25% of dominant swellings should be removed on the grounds of neoplasia.
the age and sex of the patient and the size of the swelling may be relative indications for surgery
clinical criteria to assist in selection for operation according to the risk of neoplasia and malignancy…. hard, irregular swelling …..RLN paralysis……Deep cervical ymphadenopathy The incidence of thyroid carcinoma in women is about three times that in men, but a discrete swelling in a male is much more likely to be malignant than in a female
The risk of carcinoma is increased at either end of the age range and a discrete swelling in a teenager of either sex must be provisionally diagnosed as carcinoma. The risk
increases as age advances beyond 50 years, more so in males.