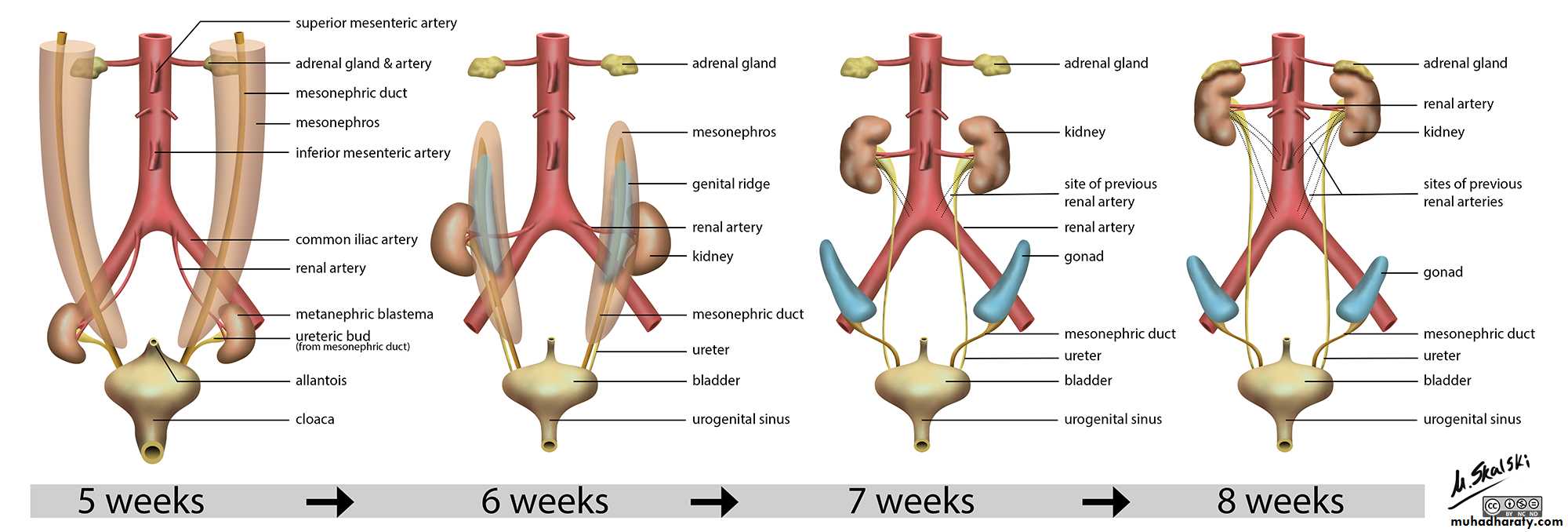
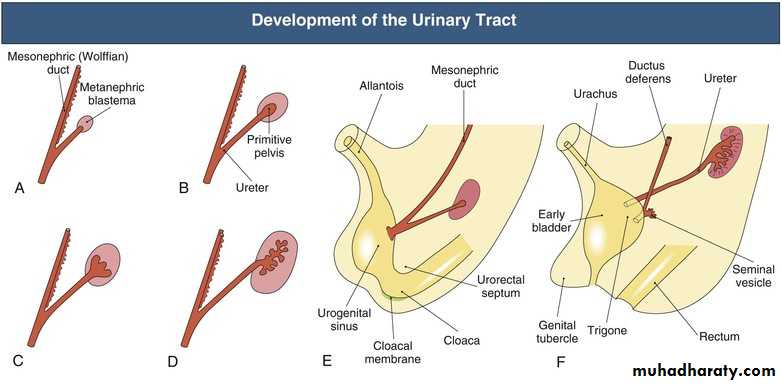
Congenital anomalies of the kidney and ureter
EMAD HASAN MAHMOODPROFESSOR OF UROLOGY
Learning objectives
1-enlist congenital abnormalities of the kidney and ureter2-describe clinical significance of these abnormalities what are symptoms and complications
3-enlist diagnostic investigations plan
4-suggest treatment plan
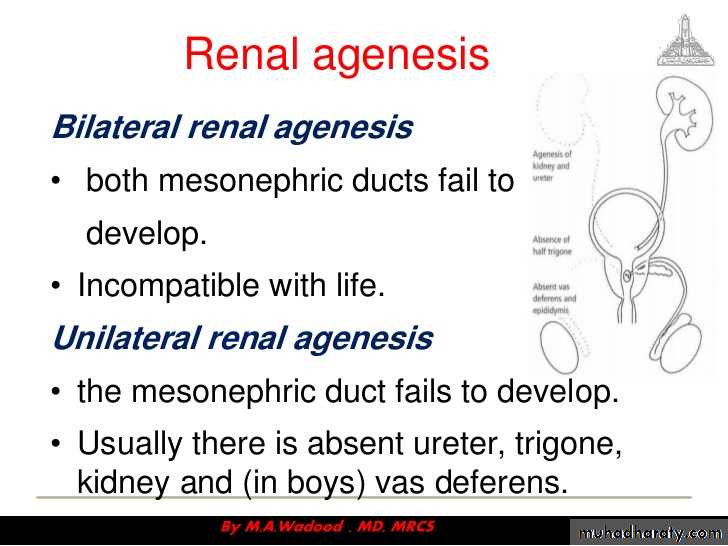
Types of renal abnormalities
1-number2-size
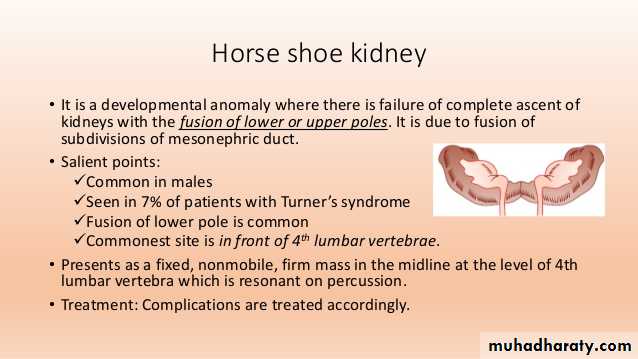
3-position
4-rotation
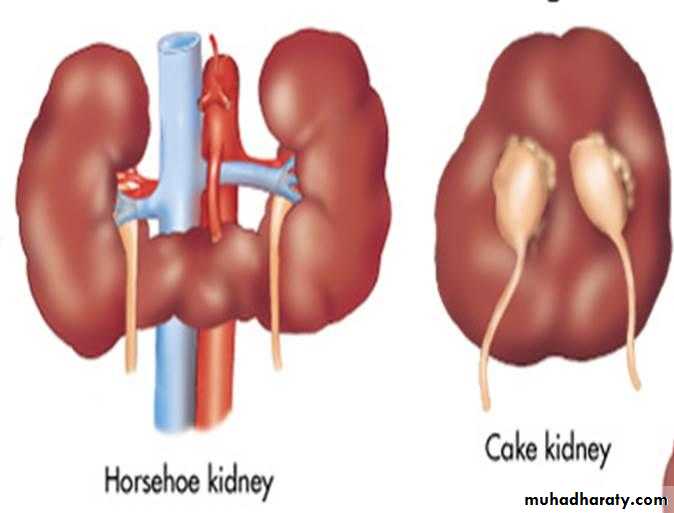
5-fusion
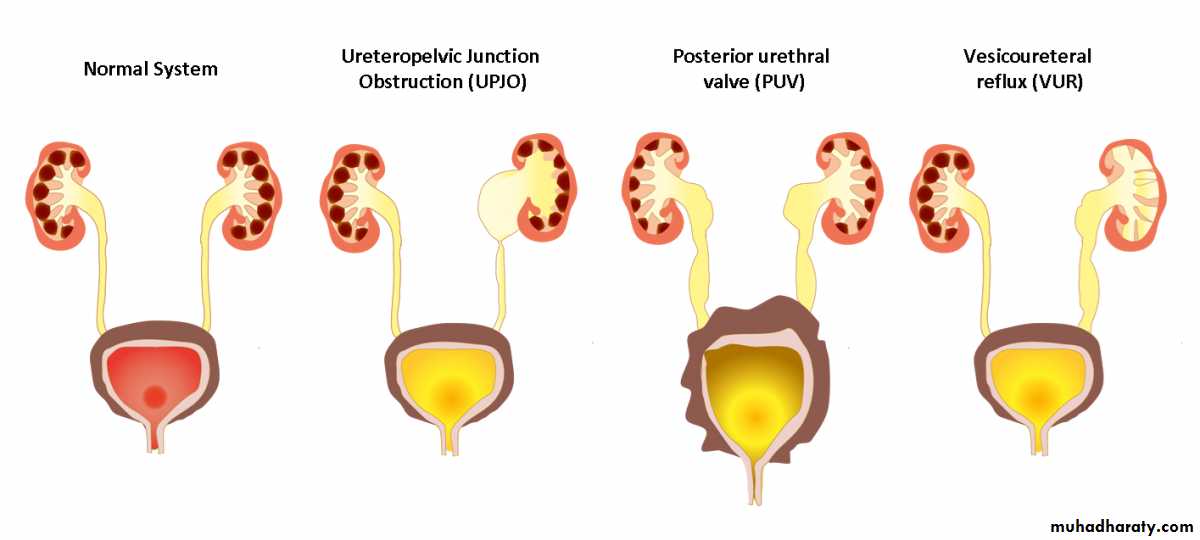
Congenital abnormalities of renal pelvis and ureter
1-pelviureteric junction obstruction2-ureteric duplications
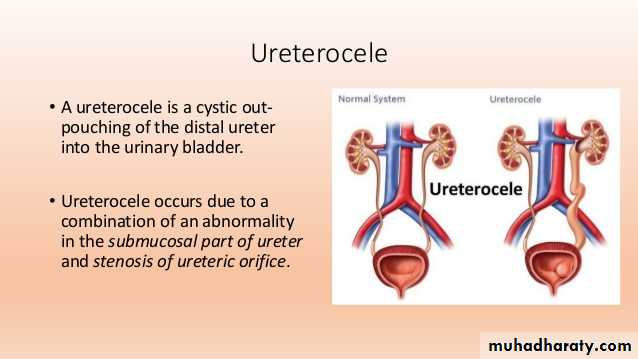
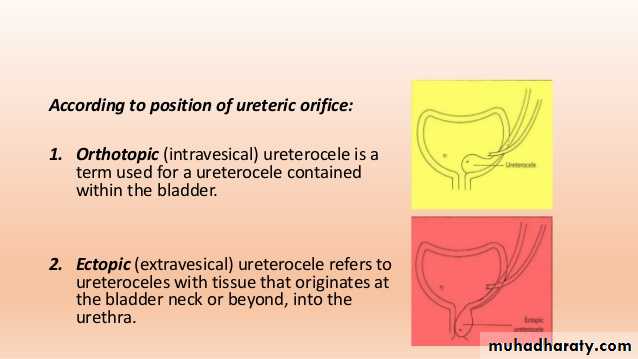
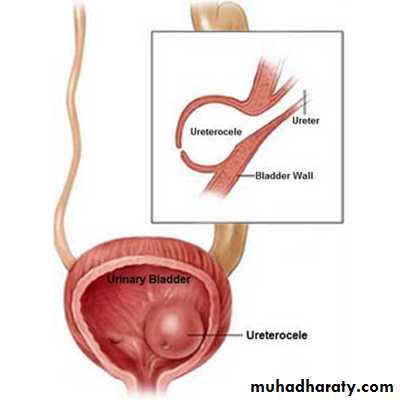
3-ureterocele
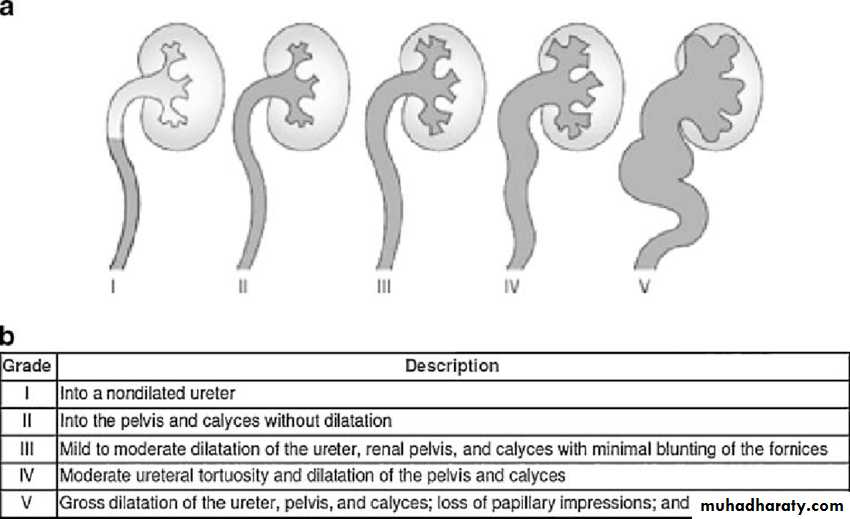
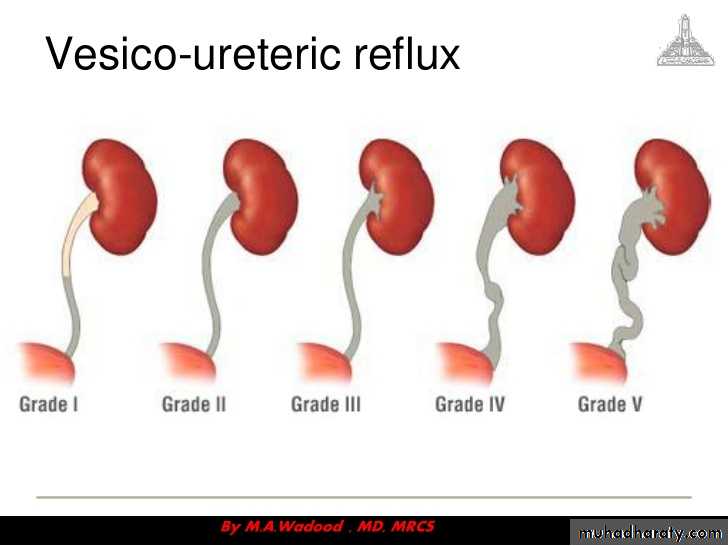
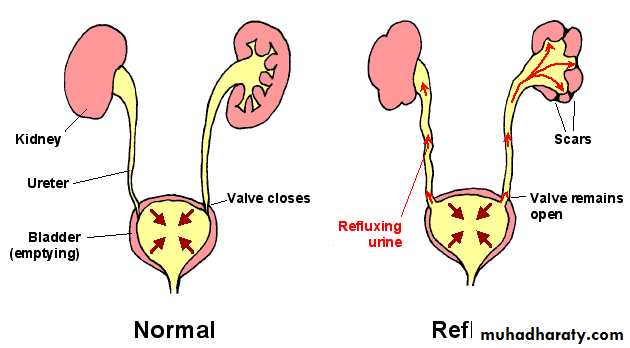
4-congenital vesicoureteric reflux
5-megaureter
6-retrocaval ureter
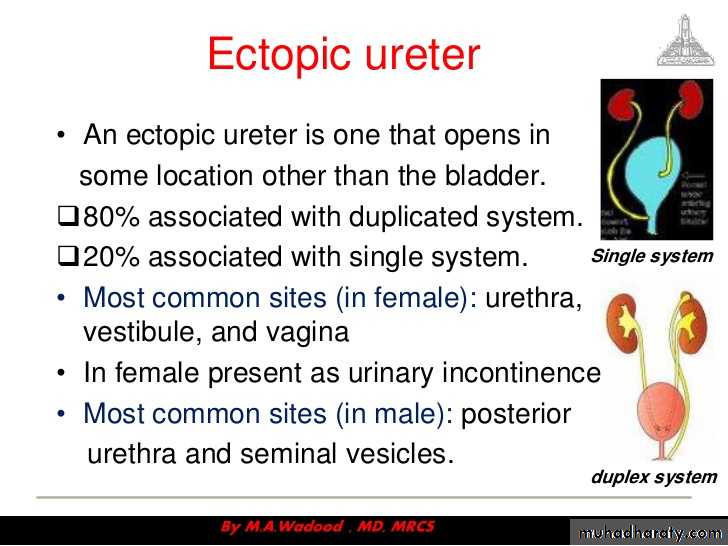
7-ectopic ureter
diagnosis
A-antenatal U/S ( 18-20 )include following severity , unilateral versus bilateral , renal parenchyma thin, bladder abnormalities , amniotic fluidB-postnatal physical examination , palpable bladder
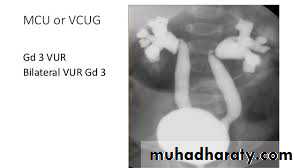
USG , IVU , MCU , DIURETIC ISOTOPES
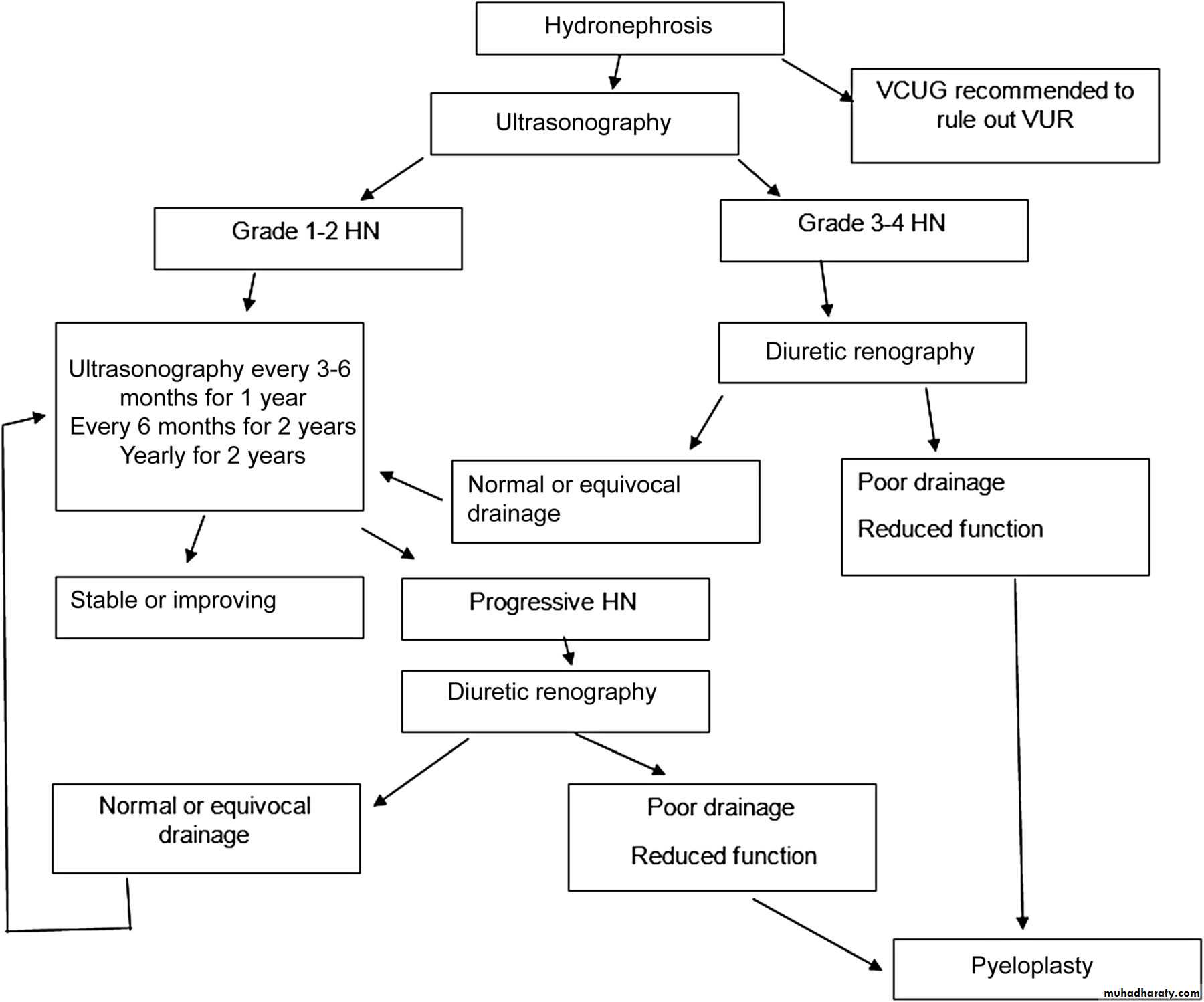
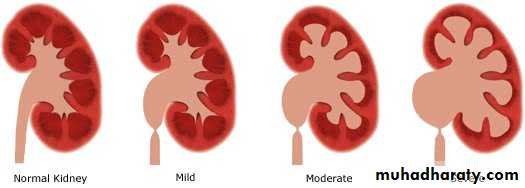
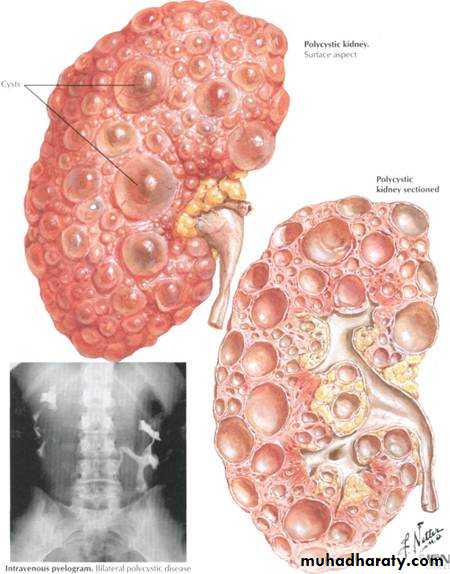
hydronephrosis
Aseptic dilatation of renal pelvis and collecting system
0.6-4.5% antenatal U/S
Several grading system (renal pelvic diameter)
Antenatal U/S
Causes
Transient , physiological , PUJ Ob. , VUR , Megaureter , Ureterocele , PUV
CONGENITAL PUJ OB
EtiologyAperistaltic segment of ureter due to absent muscle
Crossing vessel over PUJ
Valve
High insertion of ureter
Stenosis
stricture
INCIDENCEMOST COMMON KIDNEY OBSTRUCTION IN CHILDRENOCCUR IN 1 IN 500 TO 1 IN 1250
Management of UPJ obstruction
Radiological DiagnosisAbdominal U/S show various degree of hydronephrosis and ureter not dilated and evaluate parenchymal thickness
IVU same finding of U/S in addition evaluate function of the kidney
Abdominal CT with contrast same finding of IVU in addition if kidney not visualized by IVU can bee seen by CT
Radioisotopes scan ( MAG 3 ) evaluate the degree of obstruction in addition the split functio of the kidney
Urinanalysis may show RBC, WBC
Serum urea and creatinine to evaluate renal function especially in bilateral obstructionTreatment is surgical PYELOPLASTY either dimembered example (Anderson-Hynes ) OR non dismembered example vertical flap (Culp- Scardino ) OR spiral flap
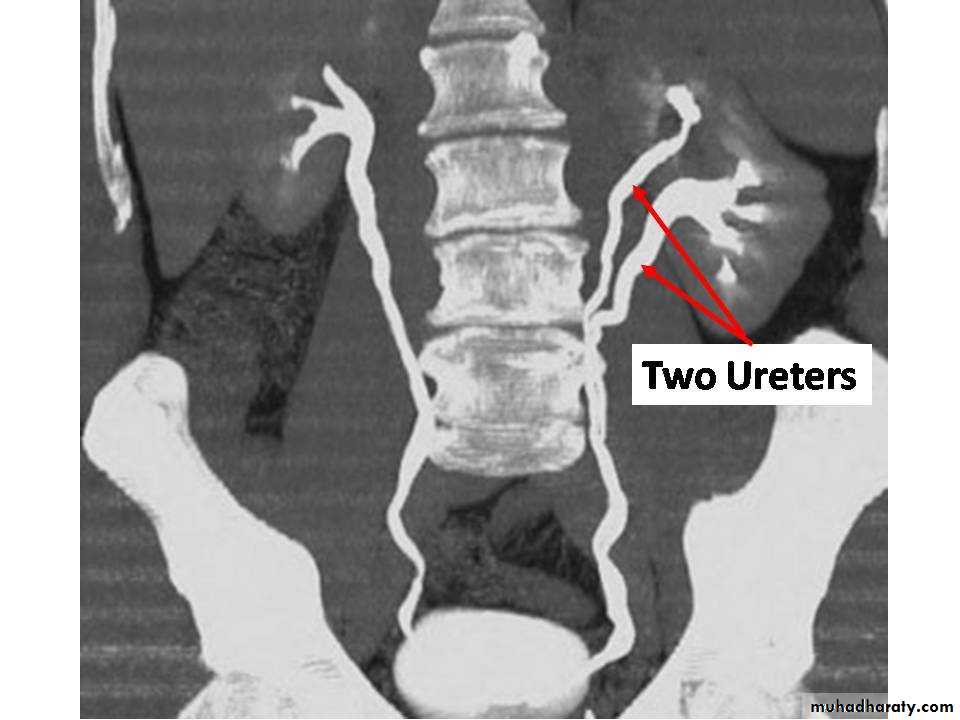
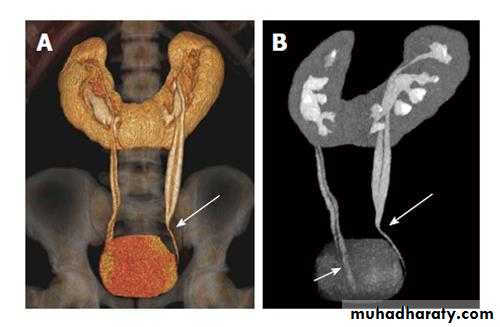
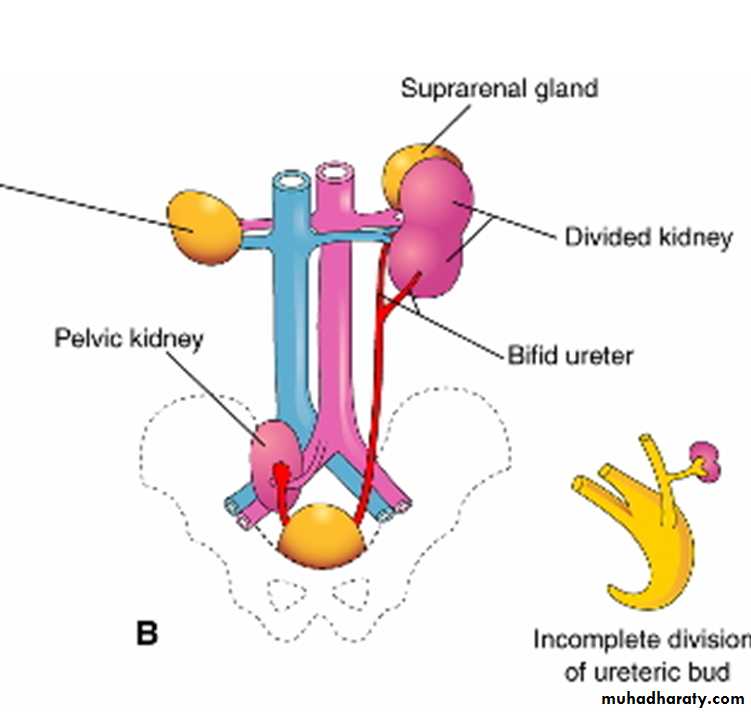
DUPLICATIONS
Renal pelvisCommon usually unilateral
Upper pelvis is small drain upper calyx
Treatment if Asymptomatic no treatment if one severe damage is partial nephrectomy
DUPLICATIONS
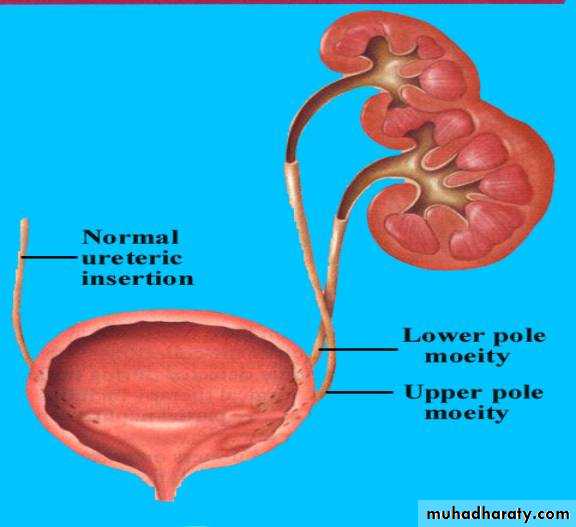
URETER
Often join together before reaching bladder or may be complete and open independently in the bladder the ureter of upper moiety opens
distal and medial to its fellow and suffer ureterocele or VUR OR ECTOPIC
COMPLICATIONS REPEATED UTI OR STONE FORMATION
TREATMENT
Asymptomatic no treatment if complications treaTment is accordingly
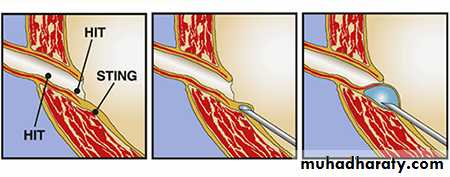
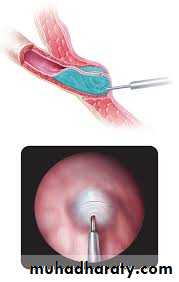
VESICOURETERIC JUNCTION OBSTRUCTION ( VUR )
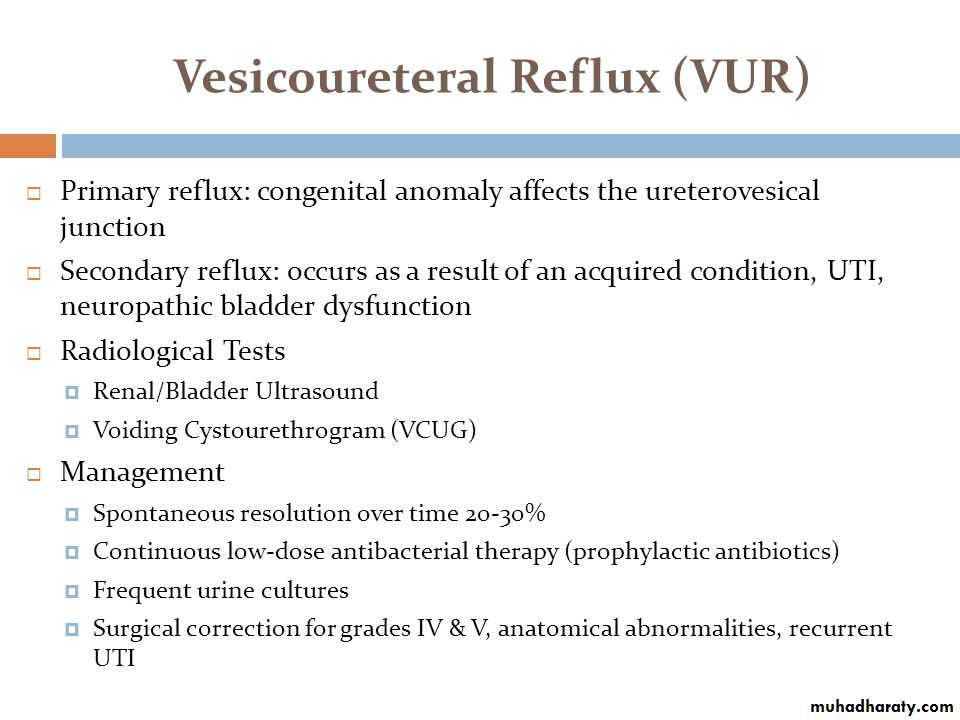
DEFLUX INJECTION THERAPY



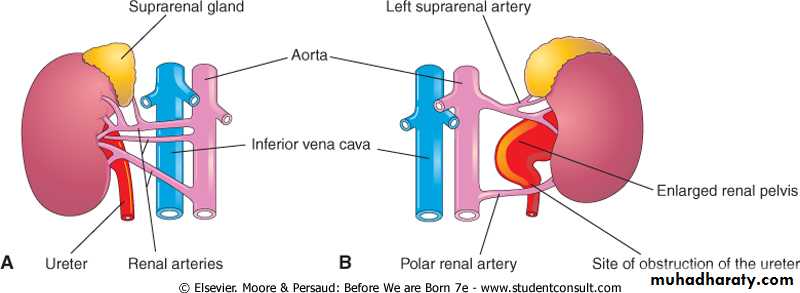
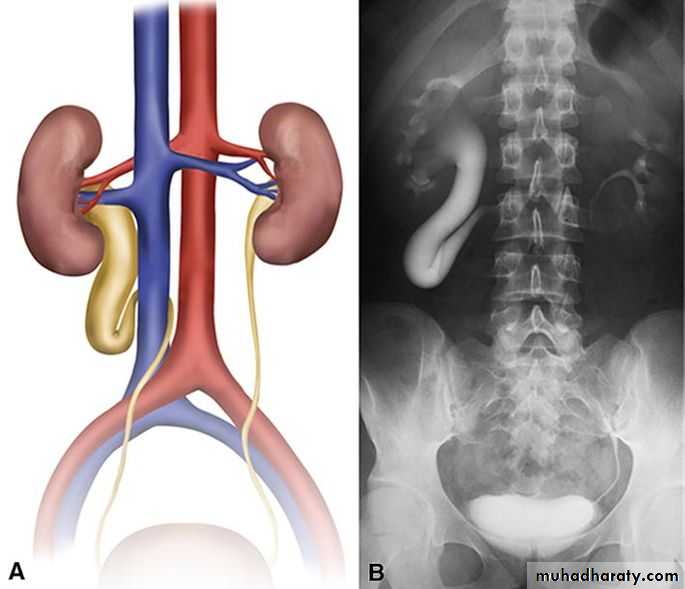
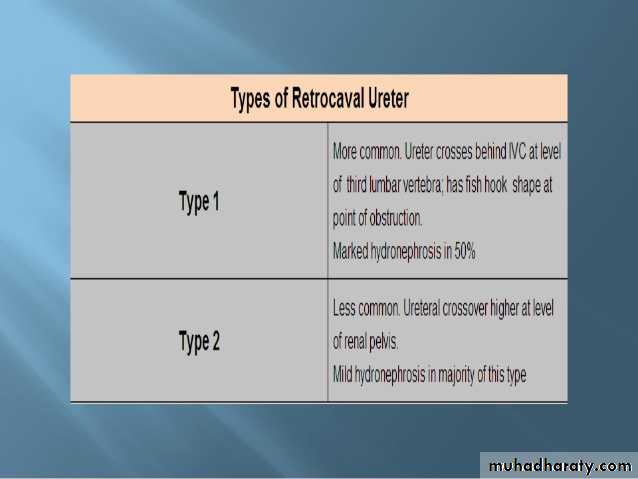
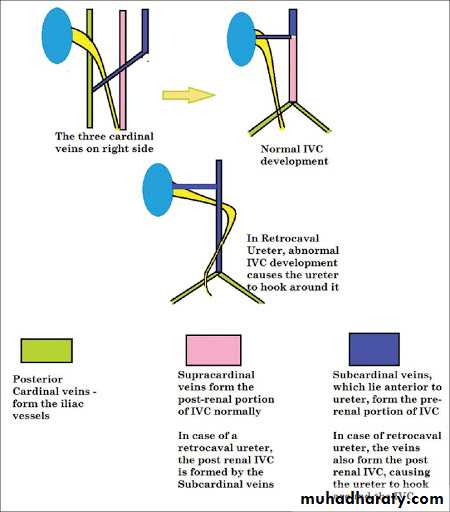
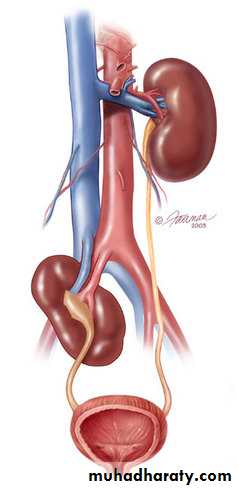
RETROCAVAL URETER

THANK YOU
