
.
CONGENITAL ABNORMALITIES OF THE SPLEEN
Splenic agenesis is rare, but is present in 10 per cent of children with congenital
heart disease. Polysplenia is a rare condition resulting from failure of splenic
fusion.
Splenunculi are single or multiple accessory spleens that are found in
approximately 10–30 per cent of the population.They are located near the hilum
of the spleen in 50 per cent of cases and are related to the splenic vessels or
behind the tail of the pancreas in 30 per cent. The remainder are located in the
mesocolon or the splenic ligaments. Their significance lies in the fact that failure
to identify and remove these at the time of splenectomy may give rise to
persistent disease.
Hamartomas are rarely found in life and vary in size from 1 cm in diameter to
masses large enough to produce an abdominal swelling.
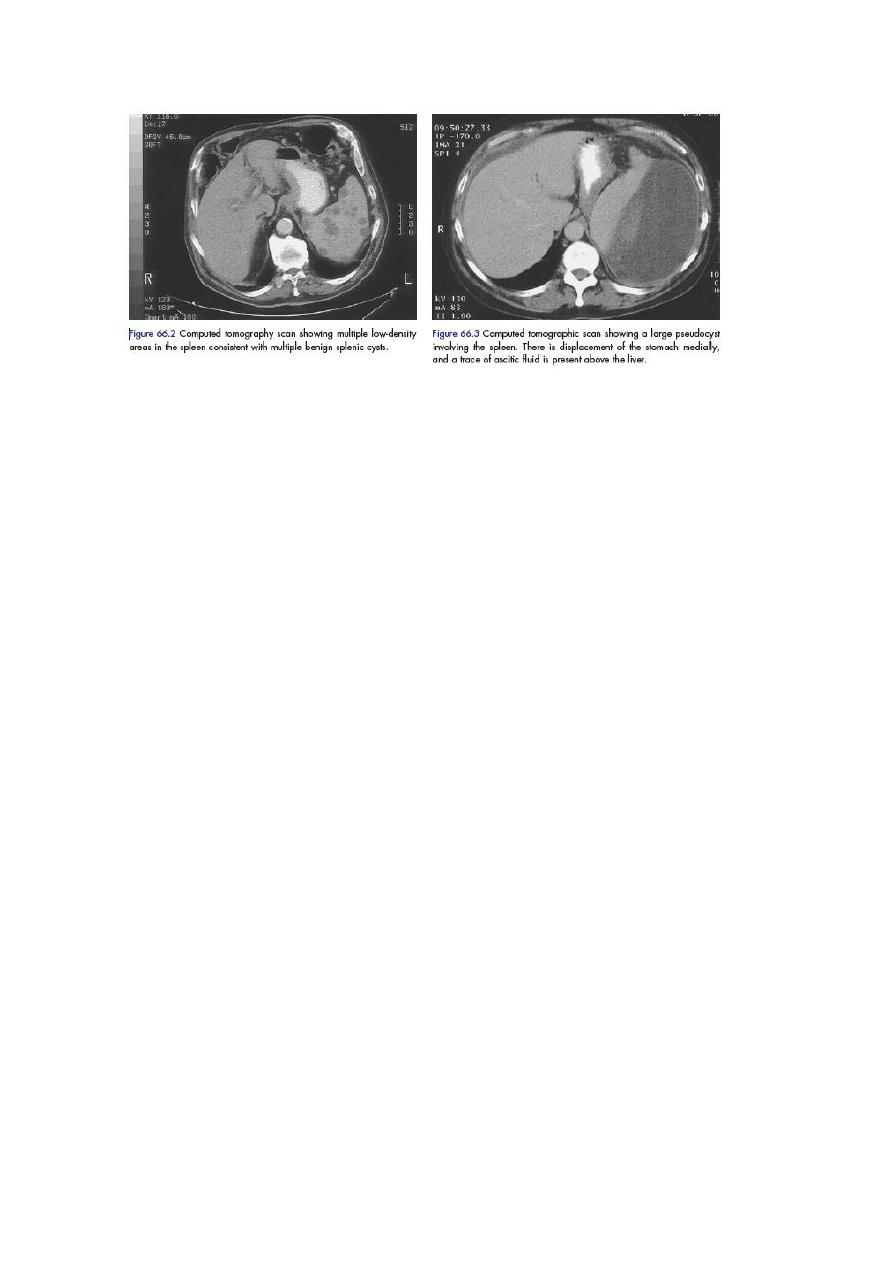
Non-parasitic splenic cysts are rare. Splenic cysts are classified as primary cysts
(true) or pseudocysts (secondary) on the basis of the presence or absence of
lining epithelium. True cysts form from embryonal rests and include dermoid
and mesenchymal inclusion cysts. True cysts of the spleen are very rare and are
frequently classified as cystic hemangiomas, and epidermoid and dermoid cysts.
Epidermoid cysts are thought to be of congenital origin and represent 10 per
cent of the splenic cysts. They are lined by flattened squamous epithelium and
are more frequent in children and young patients. Splenectomy or partial
splenectomy is usually considered for cysts larger than 5 cm in diameter. These
should be differentiated from false or secondary cysts that may result from
trauma and contain serous or haemorrhagic fluid. The walls of such degenerative
cysts may be calcified and therefore resemble the radiological appearances of a
hydatid cyst. The spleen is also a common site for pseudocyst development
following a severe attack of pancreatitis). Pseudocysts can easily be diagnosed
on scanning, and intervention is normally required for symptomatic lesions that
persist following a period of observation
.
SPLENIC ARTERY ANEURYSM, INFARCT AND RUPTURE
Splenic artery aneurysm
They are twice as common in the female and are usually situated in the main
arterial trunk. Although these are generally single, more than one aneurysm is
found in a quarter of cases. These may be a
consequence of intra-abdominal sepsis and pancreatic necrosis in particular.
They are more likely to be associated with arteriosclerosis in elderly patients.
The aneurysm is symptomless unless it
Almost half the cases of rupture occur in patients younger than 45 years of age,
and a quarter are in pregnant women, usually in the third trimester of pregnancy
or
at labour. Aneurysmal rupture carries a high mortality rate and
The treatment ligation of the proximal and distal ends of the sac to allow
thrombosis
of the aneurysm and partial or complete splenectomy if necessary.. Embolisation
or endovascular stenting following selective splenic artery angiography can be
considered
Splenic infarction
This condition commonly occurs in patients with a massively enlarged spleen
from myeloproliferative syndrome, portal hypertension or vascular occlusion
produced by pancreatic disease, splenic vein thrombosis or sickle cell disease.
The infarct may be asymptomatic or give rise to left upper quadrant and left
shoulder tip pain. A contrast-enhanced CT will show the characteristic perfusion
defect in the enlarged spleen ,
Treatment is conservative and splenectomy should be considered only when a
septic infarct causes an abscess.
Splenic rupture
Splenic rupture should be considered in any case of blunt abdominal trauma,
particularly when the injury occurs to the left upper quadrant of the abdomen.
Iatrogenic injury to the spleen remains a frequent complication of any surgical
procedure, particularly those in the left upper quadrant when adhesions are
present. Splenic injury occurs from direct blunt trauma. Most isolated splenic
injuries, especially in children, can be managed nonoperatively. However, in
adults, especially in the presence of other injury, age >55 years, or physiological
instability, splenectomy should be considered.
.
SPLENOMEGALY AND HYPERSPLENISM
Splenomegaly Few conditions that cause splenomegaly will require
splenectomy as part of treatment.
Hypersplenism is an indefinite clinical syndrome that is characterised by
splenic enlargement, any combination of anaemia, leucopenia or
thrombocytopenia, compensatory bone marrow hyperplasia and improvement
after splenectomy. Careful clinical judgement is required to balance the long-

and short-term risks of splenectomy against continued conservative
management.
Splenic abscess
Splenic abscess may arise from an infected splenic embolus or in association
with typhoid and paratyphoid fever, osteomyelitis, otitis media and puerperal
sepsis. it may be associated with pancreatic necrosis or other intraabdominal
infection. An abscess may rupture and form a left subphrenic abscess or result in
diffuse peritonitis.
Treatment involves that of the underlying cause and percutaneous drainage of
the splenic abscess under radiological guidance is normally required.
Tuberculosis
Tuberculosis of the spleen may produce portal hypertension or, rarely, cold
abscess. Treatment with anti-tuberculous drugs will normally produce
improvement. Splenectomyis not normally required and is made difficult by the
inflammatory adhesions.

Causes of splenic enlargement.
Infective Bacterial Typhoid and paratyphoid Typhus Tuberculosis
Septicaemia Splenic abscess Spirochaetal Weil’s disease Syphilis
Viral Infectious mononucleosis
HIV-related thrombocytopenia
Protozoal and parasitic Malaria Schistosomiasis Trypanosomiasis
Kala-azar Hydatid cystc
Tropical splenomegaly
Blood disease Acute leukaemia Chronic leukaemia Pernicious anaemia
Polycythaemia vera Erythroblastosis fetalis Idiopathic thrombocytopenic
purpurac Hereditary spherocytosis Autoimmune haemolytic
anaemiaThalassaemia
Sickle cell disease
Metabolic Rickets Amyloid Porphyria
Gaucher’s diseaseb
Circulatory Infarct Portal hypertension Segmental portal hypertension
(Pancreatic carcinoma, splenic vein thrombosis)
Collagen disease
Still’s disease Felty syndrome

Non-parasitic cysts Congenital Acquired
Neoplastic Angioma Primary fibrosarcoma
Hodgkin’s lymphoma
Other lymphomas Myelofibrosis
.
Leukaemia
Leukaemia should be considered in the differential diagnosis of splenomegaly
and the diagnosis is made by examining a blood or marrow film. Splenectomy is
reserved for hypersplenism that occurs during the chronic phase of chronic
granulocytic leukaemia.
Idiopathic thrombocytopenic purpura
In most cases of idiopathic thrombocytopenic purpura (ITP), the low platelet
count results from the development of antibodies to specific platelet membrane
glycoproteins that damage the patient’s own platelets. It is also known as
immune and autoimmune thrombocytopenic purpura. It is defined as isolated
thrombocytopenia with normal bone marrow and the absence of other causes of
thrombocytopenia. Two distinct clinical types are evident: the acute condition in
children and a chronic condition in adults.
Clinical features
The adult form normally affects females between the ages of 15 and 50 years,
although it can be associated with other conditions, including systemic lupus
erythematosus, chronic lymphatic leukaemia and Hodgkin’s disease. The
childhood form presents before the age of five years. Purpuric patches
(ecchymoses) occur on the skin and mucous membranes. There is a tendency to
spontaneous bleeding from mucous membranes (e.g. epistaxis); in women,
menorrhagia and the prolonged bleeding of minor wounds are common.
Although intracranial haemorrhage is also uncommon, it is the most frequent
cause of death. The diagnosis is made based upon the presence of cutaneous
ecchymoses and a positive tourniquet test. The spleen is palpable in fewer than
10 per cent of patients, and the presence of gross splenic enlargement should
raise the suspicion of an alternative diagnosis.
Investigations Coagulation studies are normal, and a bleeding time is not
helpful in diagnosis. Platelet count in the peripheral blood film is reduced
(usually <60 × 109/L). Bone marrow aspiration reveals a plentiful supply of
platelet-producing megakaryocytes.
Treatment
The course of the disease differs in children and adults. The disease regresses
spontaneously in 75 per cent of paediatric cases following the initial attack.
Short courses of corticosteroids in both adult and child are usually followed by
recovery. Prolonged steroid therapy should not be continued if this does not
produce remission. Splenectomy is usually recommended if a patient has two
relapses on steroid therapy or if the platelet count remains low. Generally, this is
indicated where the ITP has persisted for more than 6–9 months.

Haemolytic anaemias
There are four causes of haemolytic anaemia that are generally amenable to
splenectomy.
Hereditary spherocytosis
characterised by the presence of spherocytic red cells, caused by various
molecular defects in the genes that code for proteins are necessary to maintain
the normal biconcave shape of the erythrocyte. Spherocytosis arises essentially
from an increase in permeability of the red cell membranes to sodium.
The clinical presentation is generally in childhood, but may be delayed until
later life. Mild intermittent jaundice is associated with mild anaemia,
splenomegaly and gallstones.
.
All patients with hereditary spherocytosis should be treated by splenectomy but,
in juvenile cases, this is generally delayed until six years of age to minimise the
risk of post-splenectomy infection, but before gallstones have had time to form.
Ultrasonography should be performed preoperatively to determine the presence
or absence of gallstones.
Acquired autoimmune haemolytic anaemia
This condition is divided into immune and non-immune mediated forms. It may
arise following exposure to agents such as chemicals, infection or drugs, e.g.
alpha-methyldopa, or be associated with another disease (e.g. systemic lupus
erythematosus).In half the patients, the spleen is enlarged and, in 20 per cent of
cases, pigment gallstones are present.
. Splenectomy should, however, be considered if corticosteroids are ineffective,
when the patient is developing complications from long-term steroid treatment
or if corticosteroids are contraindicated. Eighty per cent of patients respond to
splenectomy.
Sickle cell disease
The diagnosis is made by the finding of characteristic sickle-shaped cells on
blood film, , haemoglobin electrophoresis.
Hypoxia that provokes a sickling crisis should be avoided and is particularly
relevant in patients undergoing general anaesthesia. Adequate hydration and
partial exchange transfusion may help in a crisis. Splenectomy is of benefit in a
few patients in whom excessive splenic sequestration of red cells aggravates the
anaemia. Chronic hypersplenism usually occurs in late childhood or
adolescence, although Streptococcus pneumoniae infection may precipitate an
acute form in the first five years of life
.
Hypersplenism due to portal hypertension
Splenomegaly is an invariable feature of portal hypertension and results in the
thrombocytopenia and granulocytopenia observed in these patients. These may
be improved if the portal hypertension is relieved by shunt surgery or liver
transplantation. Splenectomy would normally be required only in those patients

whose segmental portal hypertension has resulted in symptomatic
oesophagogastric varices.
NEOPLASMS
Haemangioma is the most common benign tumour of the spleen and may rarely
develop into a haemangiosarcoma that is managed by splenectomy. The spleen
is rarely the site of metastatic disease. Lymphoma is the
most common cause of neoplastic enlargement, and splenectomy may play a
part in its management. Splenectomy may be required to achieve a diagnosis in
the absence of palpable lymph nodes or to relieve the symptoms of gross
splenomegaly. Its use has been restricted to those patients in whom a definite
histological diagnosis of intra-abdominal disease will affect management. Thus,
selected patients with stage IA or IIA Hodgkin’s disease may be candidates for
staging laparotomy or laparoscopy. In the absence of obvious liver or intra-
abdominal nodal disease, splenectomy is an integral part of the staging
procedure to exclude splenic involvement, which would alter the method of
treatment.
SPLENECTOMY
The common indications for splenectomy are:
•
trauma resulting from an accident or during a surgical procedure, as for
example during mobilisation of the oesophagus, stomach, distal pancreas or
splenic flexure of the colon;
•
removal en bloc with the stomach as part of a radical gastrectomy or with the
pancreas as part of a distal or total pancreatectomy;
•
to reduce anaemia or thrombocytopenia in spherocytosis, idiopathic
thrombocytopenic purpura or hypersplenism;
•
in association with shunt or variceal surgery for portal hypertension
Preoperative preparation
In the presence of a bleeding tendency, transfusion of blood, fresh-frozen
plasma, cryoprecipitate or platelets may be required. Coagulation profiles should
be as near normal as possible at operation, and platelets should be available for
patients with thrombocytopenia at operation and in the early postoperative
period. Antibiotic prophylaxis appropriate to the operative procedure should be
given and consideration should be given to the risk of post-splenectomy sepsis
Technique of open splenectomy
Most surgeons use a midline or transverse left subcostal incision for open
splenectomy
.
In elective splenectomy, the gastrosplenic ligament is opened up, and the short gastric
vessels are divided. The splenic vessels at the superior border of the pancreas are suture-ligated. The posterior
surface of the spleen is exposed, the posterior leaf of the lienorenal ligament divided with long curved scissors,
and the spleen rotated medially along with the tail and body of the pancreas. The pancreas is separated from the
hilar vessels, which are ligated and divided.
Accessory splenic tissue in the splenic hilum or
omentum should be excluded by a careful search at operation
Postoperative complications
Immediate complications specific to splenectomy include haemorrhage resulting
from a slipped ligature. Haematemesis from gastric mucosal damage and gastric

dilatation is uncommon. Left basal atelectasis is common, and a pleural effusion
may be present. Adjacent structures at risk during the procedure include:
the stomach and pancreas. A fistula may result from damage to the greater
curvature of the stomach during ligation of the short gastric vessels. Damage to
the tail of the pancreas may result in pancreatitis, a localised abscess or a
pancreatic fistula.
Postoperative thrombocytosis may arise and, if the blood platelet count exceeds
1 × 10
6
/mL, prophylactic aspirin is recommended to prevent axillary or other
venous thrombosis.
Post-splenectomy septicaemia may result from Streptococcus pneumoniae,
Neisseria meningitides, Haemophilus influenzae and Escherichia coli.
The risk is greater in the young patient, in splenectomised patients treated with
chemoradiotherapy and in patients who have undergone splenectomy for
thalassaemia,, sickle cell disease and autoimmune anaemia or
thrombocytopenia.
Opportunist post-splenectomy infection (OPSI) is a major concern, most
infections after splenectomy could be avoided through offering patients
appropriate and timely immunisation, antibiotic prophylaxis, education and
prompt treatment of infection.
It is thought that children who have undergone splenectomy before the age of
five years should be treated with a daily dose of penicillin until the age of ten
years. Prophylaxis in older children should be continued at least until the age of
16 years, but its use is less well defined in adults.
As the risk of overwhelming sepsis is greatest within the first
2–3 years after splenectomy, it seems reasonable to give prophylaxis
during this time. However, all patients with compromised
immune function should receive prophylaxis. Satisfactory oral
prophylaxis can be obtained with penicillin, erythromycin or
amoxicillin, or co-amoxiclav. Suspected infection can be treated
intravenously with these same antibiotics and cefotaxime, ceftriaxone
or chloramphenicol in patients allergic to penicillin
and cephalosporins
vaccinations should be administered at least 2 weeks before elective surgery
or as soon as possible after recovery from surgery but before discharge from
hospital. Pneumococcal vaccination is recommended in those patients aged
over two years. Haemophilus influenzae type b vaccination is recommended
irrespective of age
In the trauma victim, vaccination can be given in the postoperative period,
and the resulting antibody levels will be protective in the majority of cases.