Acute abdomen
Any sudden, spontaneous, nontraumatic disorder whose
chief manifestation is in the abdominal area and for which
urgent operation may be necessary,there is frequently a
progressive underlying intra-abdominal disorder .Early
diagnosis and treatment avoid adverse outcome.

The approach to a patient with an acute
abdomen
•
must be orderly and thorough. The history and
physical examination should suggest the
probable causes and guide the choice of initial
diagnostic studies.
The clinician must then decide if :a- in-hospital
observation is warranted, b- if additional tests
are needed,c- if early operation is indicated, or
d- if nonoperative treatment would be more
suitable.

HISTORY
•
Abdominal Pain Pain is the most common and
predominant presenting feature of an acute
abdomen. Careful consideration of the
location, the mode of onset and progression,
and the character of the pain will suggest a
preliminary list of differential diagnoses.

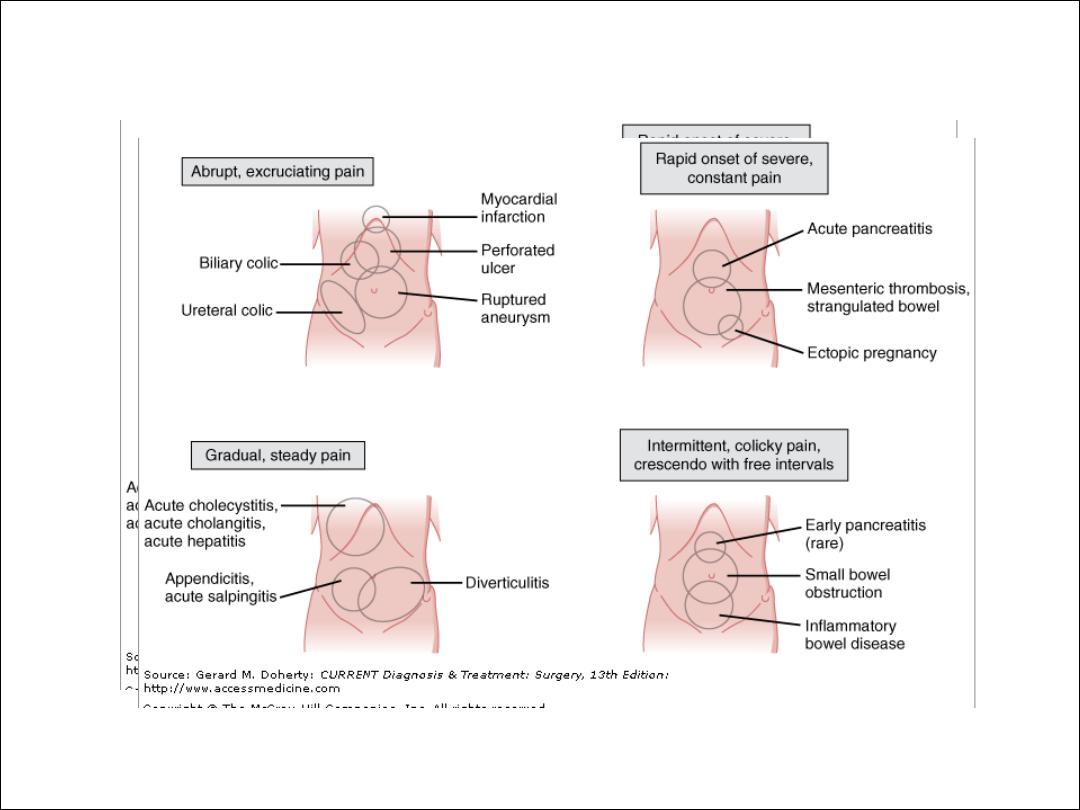
Character of pain:
The nature ,severity and periodicity of pain provide
useful clue to the underlying cause. Steady pain is most
common .sharp superficial constant pain due to sever
peritoneal irritation is typical of perforated ulcer or
rupture appendix, ovarian cyst or ectopic pregnancy.
The gripping progressing pain of small bowel obstruction
is usually intermittent, vague, deep-seated, and crescendo
at first but soon become sharper remitting and better
localized. Pain is
appropriately referred as colic if there are pain free
intervals that reflect intermittent smooth muscle
contraction

Mode of Onset and Progression of Pain
The mode of onset of pain reflects the nature and severity of
the inciting process. Onset may be explosive (within
seconds), rapidly progressive (within 1–2 hours), or gradual
(over several hours). Unheralded, excruciating generalized
pain suggests an intra-abdominal catastrophe such as a
perforated viscus or rupture of an aneurysm, ectopic
pregnancy, or abscess. Accompanying systemic signs
(tachycardia, sweating, tachypnea, shock) soon supersede
the abdominal disturbances and underscore the need for
prompt resuscitation and laparotomy.

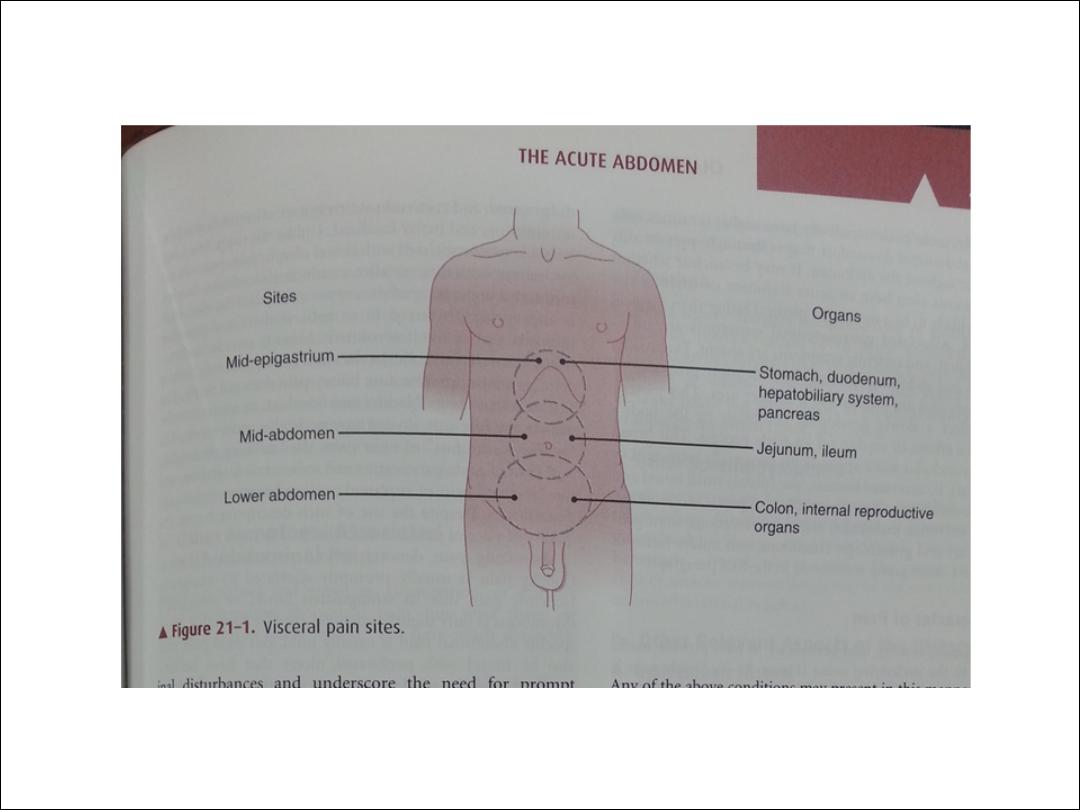
The location of the pain :
visceral pain is elicited by distention, by inflammation
or ischemia stimulating the receptor neurons, or by
direct involvement (e.g, malignant infiltration) of
sensory nerves.
parietal pain is mediated by both C and A delta nerve
fibers. Direct irritation of the somatically innervated
parietal peritoneum (especially the anterior and
upper parts) by pus, bile, urine, or gastrointestinal
secretions leads to more precisely localized pain.
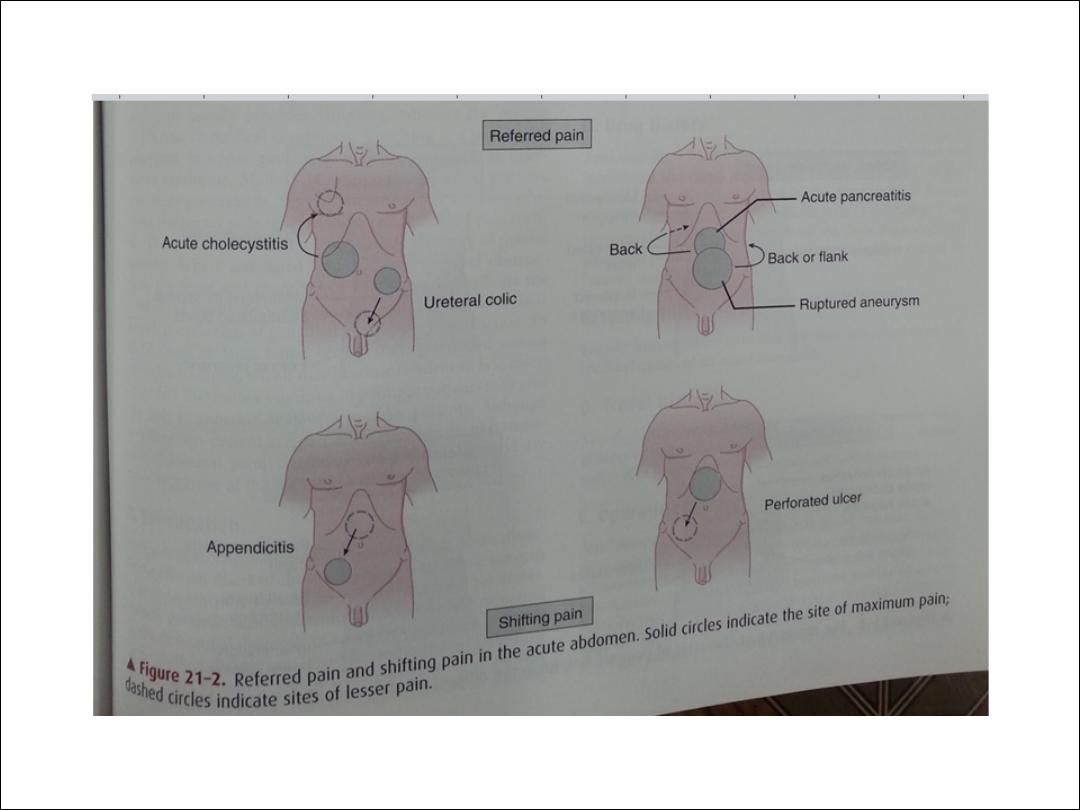
Referred pain
Abdominal pain may be referred or may shift to sites
far removed from the primarily affected organs
(Figure). Referred pain denotes noxious (usually
cutaneous) sensations perceived at a site distant from
that of a strong primary stimulus. For example, pain
due to subdiaphragmatic irritation by air, peritoneal
fluid, blood, or a mass lesion is referred to the shoulder
via the C4-mediated (phrenic) nerve. Pain may also be
referred to the shoulder from supradiaphragmatic
lesions such as pleurisy or lower lobe pneumonia,
especially in young patients.