Breast
Learning objectivesTo understand:
• Applied anatomy
• Breast anomalies and the complexity of benign breast disease
• To know how to undertake a detailed history and physical examination of a patient presenting with a breast problem
• To be able to develop a differential diagnosis for a breast mass and describe the characteristics of both malignant and benign lesions
• To be able to describe the components of the ‘triple test’
• To understand the various supportive diagnostic tools, which include imaging modalities and techniques for tissue diagnosis
Q.1
The ‘triple test’ does not include which of the following?:a History and physical examination
b Tissue diagnosis
c Genetic testing
d Radiological studies
Q.2
Commonly employed imaging modalities used to evaluate patients presenting with breast lesions include all the following except:
a Mammography
b MRI
c Ultrasound
d Positron emission tomography scanning
For each of the following descriptions, select the most likely matches for the presentations given below. Each option may be used once, more than once or not at all:
• Simple cyst
• Fibroadenoma
• Fat necrosis
• Galactocele
• Mammary fistula
• Gynaecomastia
• Subareolar abscess
Q.3 Often results from trauma to the breast and can be confused with breast cancer on imaging
Q.4 Most commonly seen during lactation and is the result of ductal obstruction
Breasts are modified sweat glands.Embryology
The breasts develop along the milk-line that extends between the limb buds from the axilla to the inguinal region distally.
Location
The breasts are located within the superficial fascia of the anterior chest wall.Extent
• Superiorly second or third rib.• Inferiorly the inframammary fold that is located at the level of the sixth or seventh rib.
• Medially the lateral border of the sternum.
• Laterally to the anterior or midaxillary line.
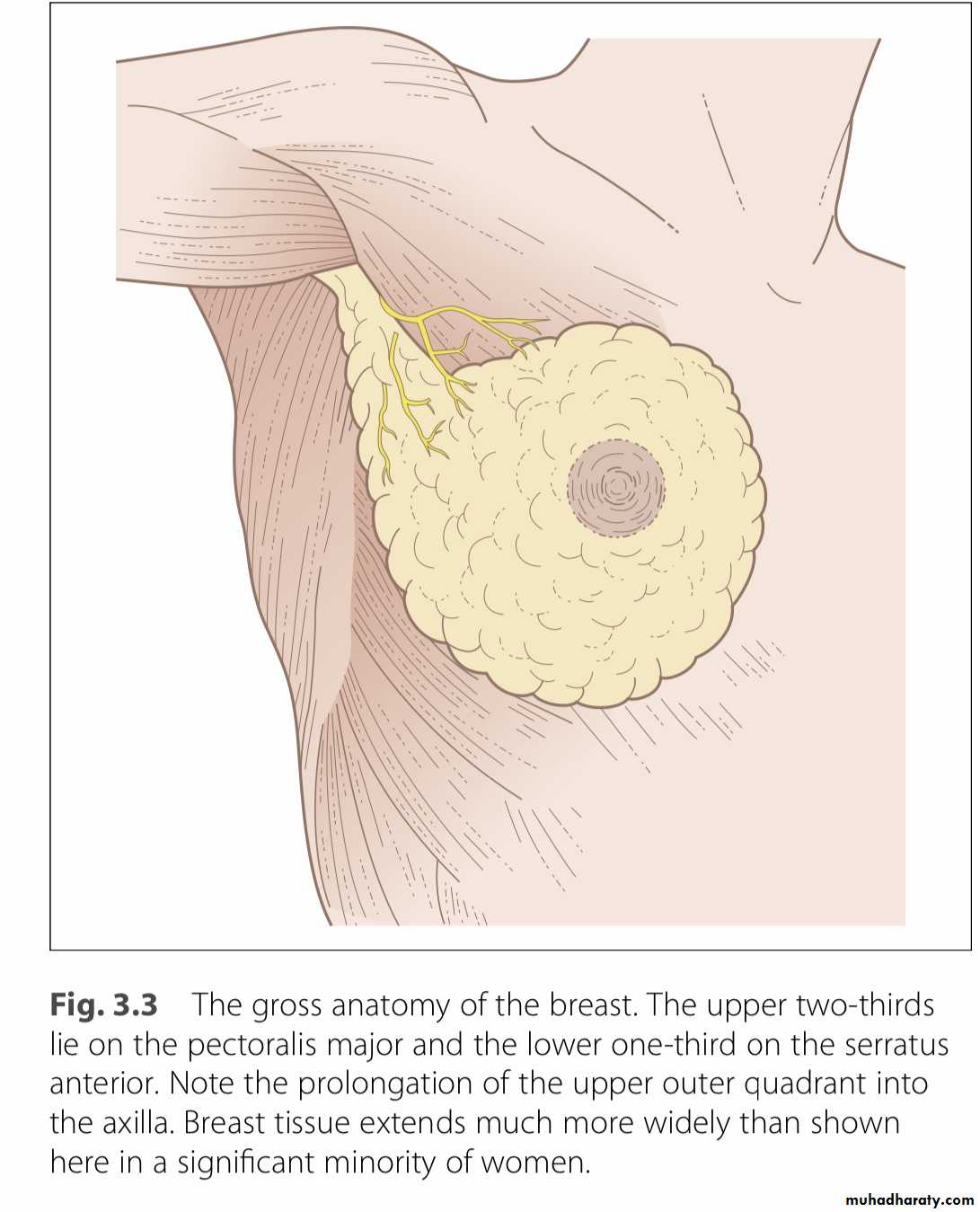
The posterior or deep surfaces of the breast rest upon portions of the fasciae of the pectoralis major, serratus anterior, external oblique muscles and upper portions of the anterior rectus sheath.
Breast tissue extends commonly into the anterior axillary fold as the axillary tail of Spence.
The upper half of the breast, particularly the upper outer quadrant, contains the greater volume of glandular tissue than the remainder of the breast.
This fact is important when performing a
mastectomy, the aim of which is to remove thewhole breast.
Structure
• 15 to 20 lobes of tubuloalveolar glandular tissue,• Fibrous connective tissue that supports its lobes, and
• Adipose tissue that resides in parenchyma between the lobes.
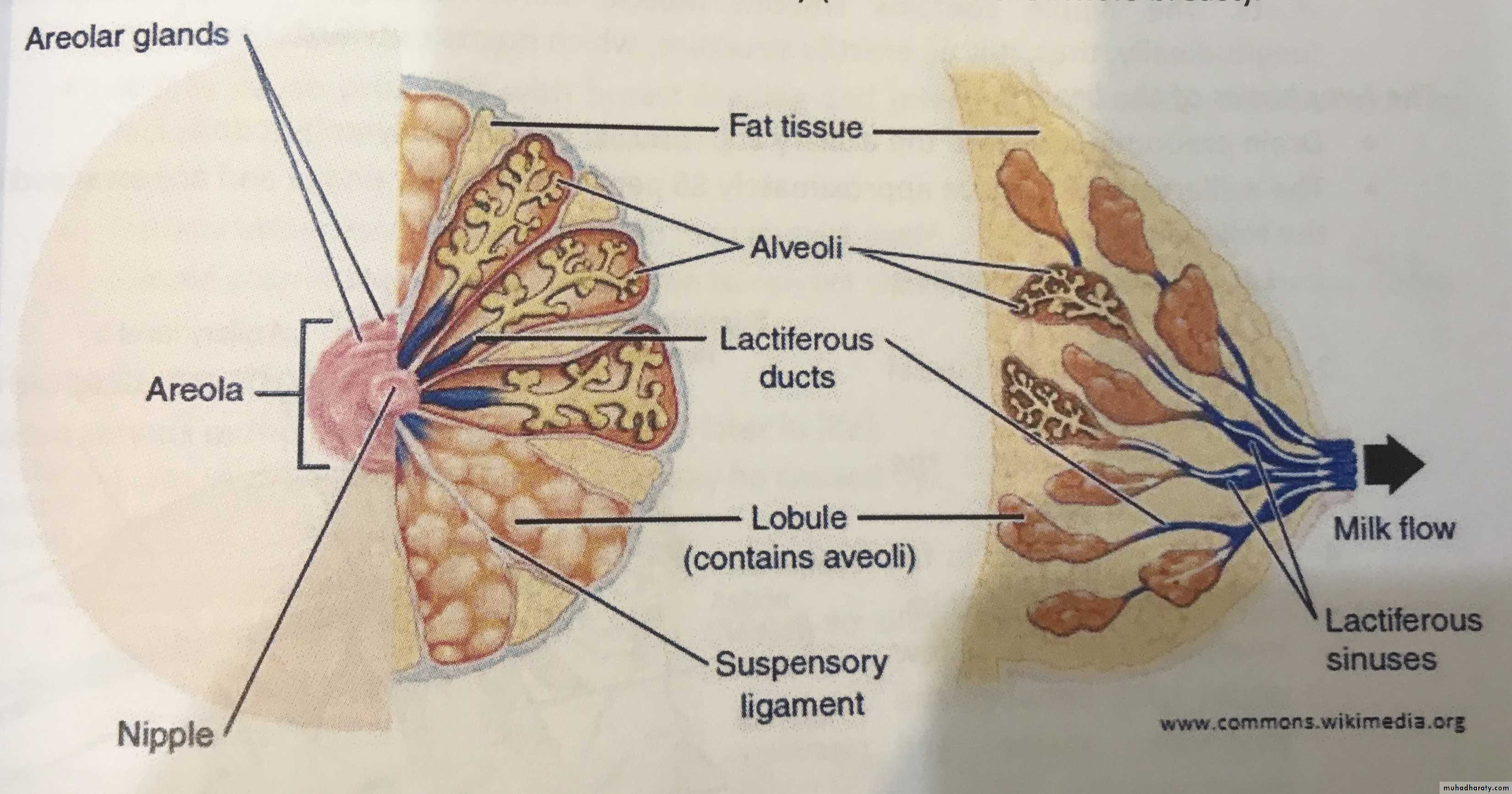
• The nipple is covered by thick skin with corrugations .
• Near its apex lie the orifiices of the lactiferous ducts .The nipple contain smooth muscle fibers arranged concentrically and longitudinally , thus , its an erectile structure , which points outwards.
Lymphatics
Lymph nodes groups– Anterior group (external mammary or pectoral group)—along the lateral thoracic vessels
– Posterior group (subscapular or scapular group)
– Lateral group (axillary vein group).
These three groups comprise the level 1 nodes and they all drain into central group in the center of axilla.
Some lymphatics drain directly from the breast into central nodes
– Rotter group (Interpectoral group or level II nodes) is located between pectoralis major and minor and also drains into the central group
– The central group as well as some branches from breast and Rotter group drain into the apical group (subclavicular group)
– The apical group finally drains into the supraclavicular group.

Common symptoms of breast problems may include a mass or lump, pain and a nipple discharge.
Women may also be referred for breast examination when a routine screening mammogram has shown an abnormality or because of a strong family history of breast cancer.
These women may be otherwise asymptomatic.
Breast history
Questions to askFor any complaint
When did it start? Has it changed?
Lump
How was it discovered?
Has there been a change in size?
Is there any associated pain or tenderness?
Does it change with menses?
Pain or tenderness
Is there an associated lump? Does it change with menses?i
Nipple discharge
Duration?
Spontaneous or elicited?
Unilateral or bilateral? Colour?
Gynaecological history
Menarche?
Number of pregnalncies?
Age at first pregnancy?
Still menstruating? Last period? Exposure to exogenous hormones?
Family history
Breast cancer (including age at diagno- sis) – bilateral?
Ovarian cancer?
Colon cancer?
Melanoma?
Other malignancies?
The breast history
Physical examination
Inspection
SymmetrySigns of retraction
Nipple retraction Skin changes
Palpation
Masses
Axillae
Triple breast assessment includes:
Clinical breast examination.Imaging (USG or mammography or MRI).
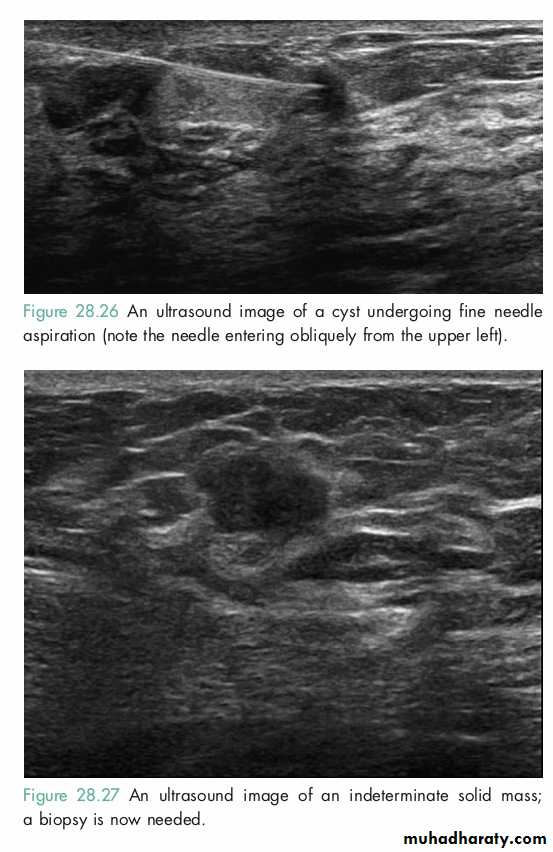
Tissue sampling (FNAC or true cut biopsy).Investigation of the breast
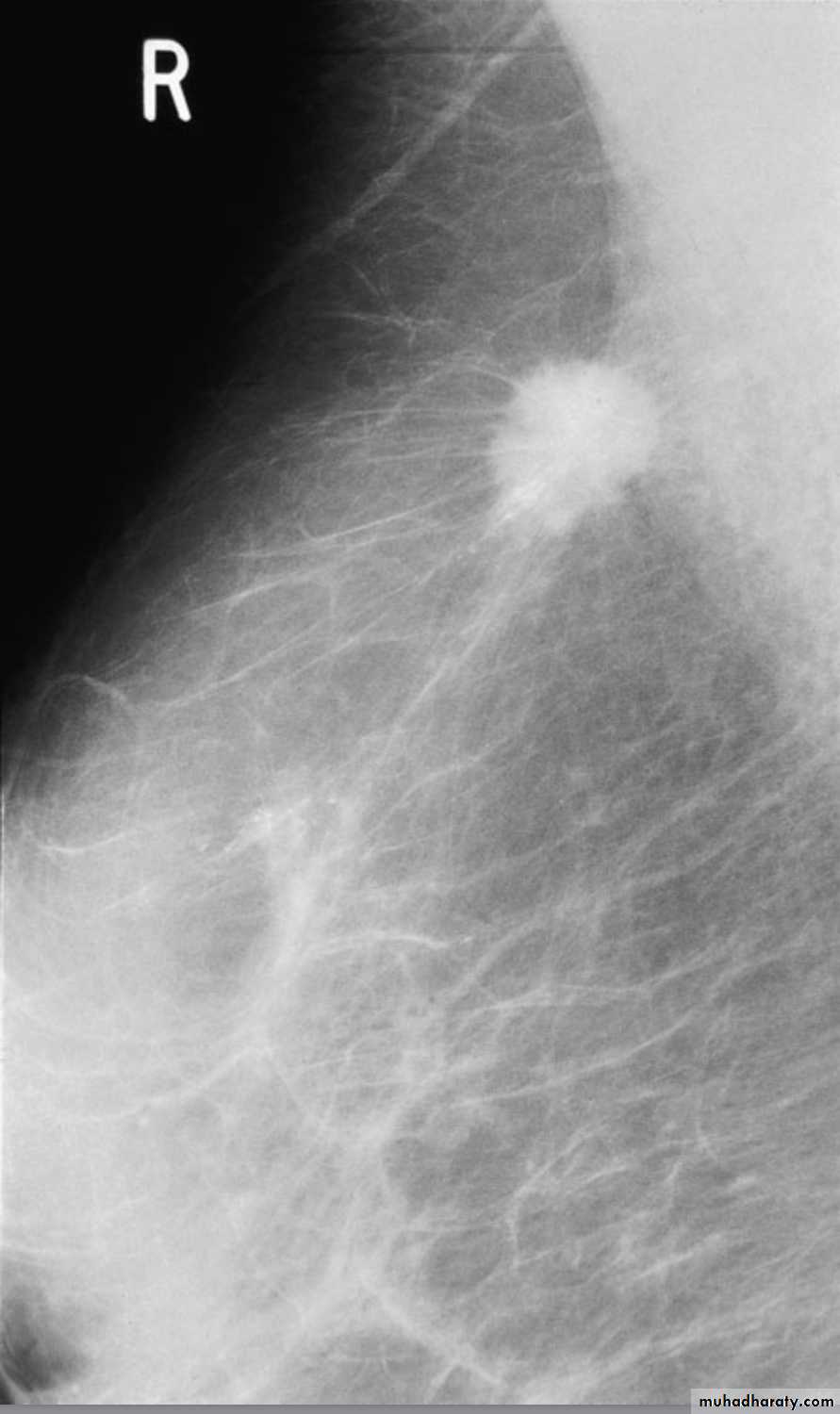
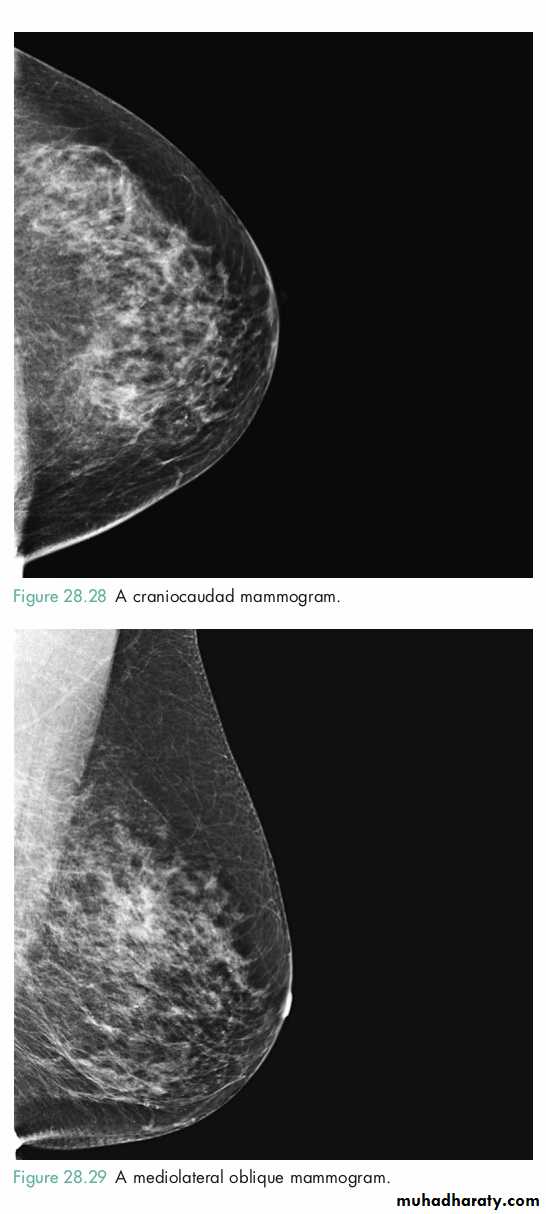
MammographySoft tissue X-rays are taken by placing the breast in direct contact with ultrasensitive film and exposing it to low-voltage, high-amperage X-rays.
The dose of radiation is approximately 0.1 Gy and therefore mammography is a very safe investigation.
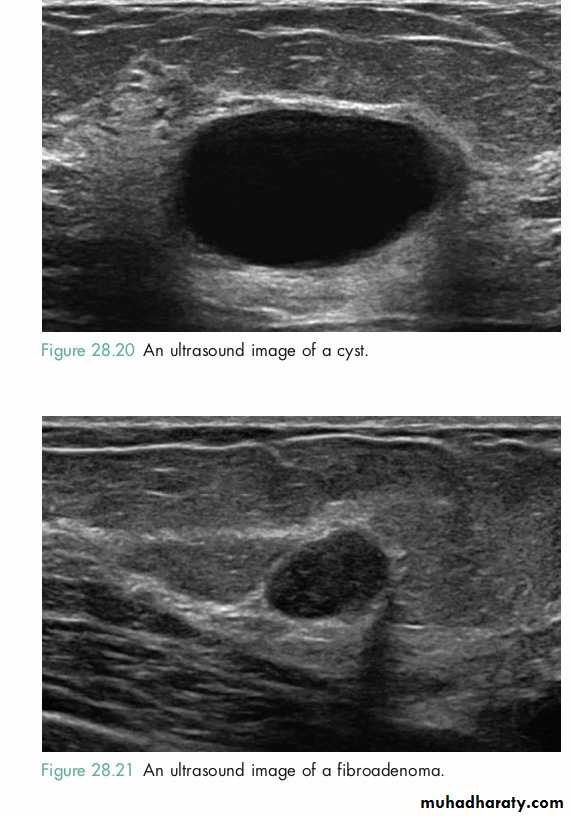
Ultrasound
Ultrasound is particularly useful in young women with dense breasts in whom mammograms are difficult to interpret, and in distinguishing cysts from solid lesions.
Magnetic resonance imaging
• it can be useful to distinguish scar from recurrence in women who have had previous breast conservation therapy for cancer (although it is not accurate within 9months of radiotherapy because of abnormal enhancement).• it is the gold standard for imaging the breasts of women with implants.
• it may prove useful as a screening tool in high-risk women.
• and it is being evaluated in the management of the axilla in both primary breast cancer and recurrent disease .
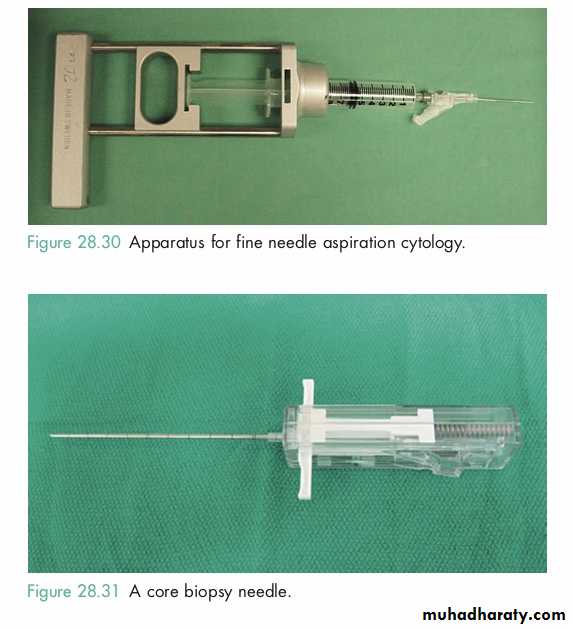
FNA
TRUE CUT BIOPSY
It is easily performed, is rapid, inexpensive, and no incision is required.
It requires a trained cytopathologist to report.
Cannot distinguish between in situ and invasive cancer.Markers (ER, PR, Her-2-neu) are not routinely available.
This also does not need any incision, and can be read by any cytopathologist with basic training.Markers can be performed on this specimen.
It reliably distinguishes in situ and invasive carcinoma.Technique of choice in patients who are planned to receive preoperative systemic therapy.
Triple assessment is the method of choice because all three together increase the diagnostic accuracy to 99.9%.
Either of them alone is not as sensitive and also has false negatives.
Thus, triple assessment is preferred.The risk of malignancy increases if there is an underlying mass.
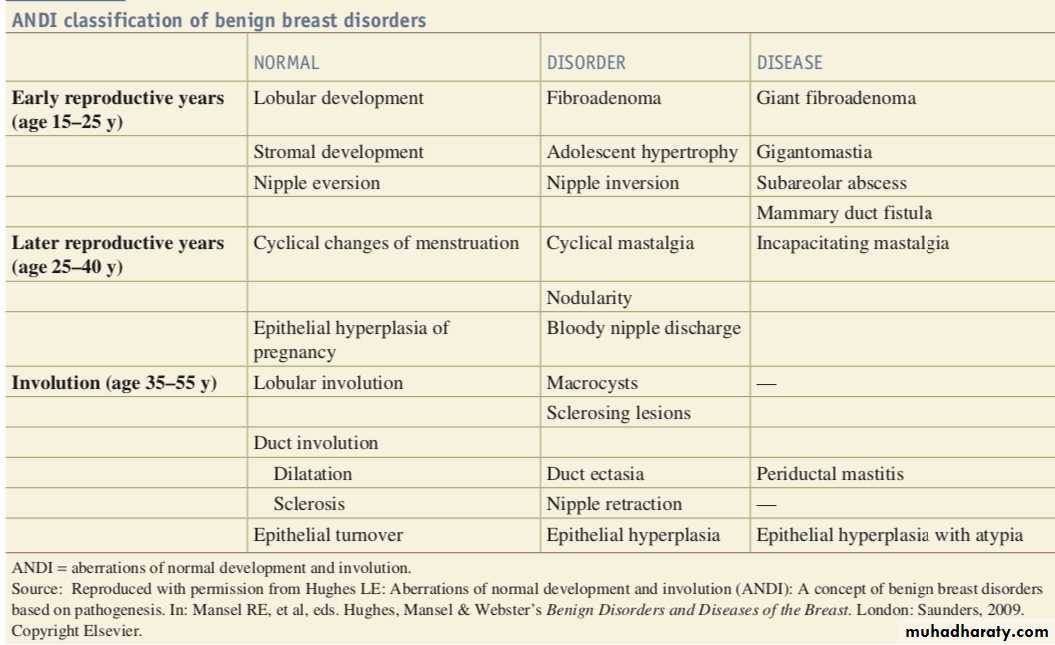
Benign breast disorders and diseases encompass a wide range of clinical and pathologic entities.Aberrations of Normal Development and Involution
The basic principles underlying the aberrations of normal development and involution (ANDI) classification of benign breast conditions are the following:• benign breast disorders and diseases are related to the normal processes of reproductive life and to involution;
• there is a spectrum of breast conditions that ranges from normal to disorder to disease; and
• the ANDI classification encompasses all aspects of the breast condition,
ANDI spectrum from normal, to mild abnormality (disorder), to severe abnormality (disease).
Pathological features of ANDI
cyst formation
Fibrosis
Hyperplasia
Papillomatosis
Clinical features of ANDI
An area of lumpiness or pain without lumpiness (mastalgia) or bothOr area of discrete lump:cyst or fibroadenoma
Characteristic : before menstrual period lumpiness and tenderness increase
• Diagnosis and treatment
The aim to exclude cancer,once this have been done , treatment any remaining symptoms.Mastalgia :Cyclic (Biopsy may be needed , oil of primrose,Danazole ) or Non-cyclic (Biopsy , NSAID)
Cyst: Aspiration ,excision May be needed.
Fibroadenoma
• It’s benign ,age is usually: 15-25 year• It’s usually presented with a mass 2-5 cm , defined capsule, mobile, not attached to skin or chest wall and not tender.
Treatment
• First ensure it’s not malignant by FNAC.if not malignant,so remove it surgically.
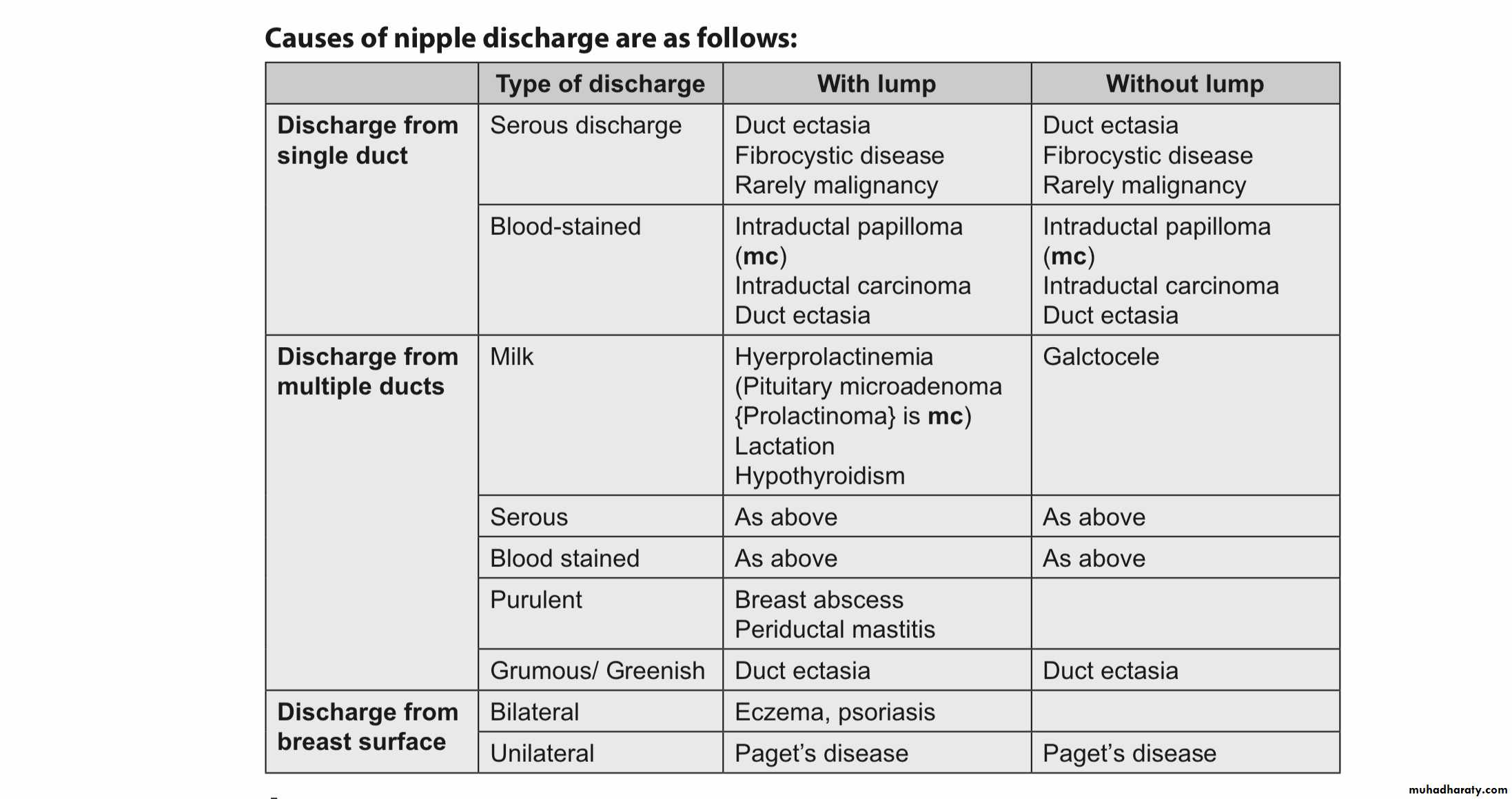
“Single duct, spontaneous, unilateral, blood-stained, clear or serous in a women above 40 years especially with a mass is suggestive of malignancy and needs evaluation.”
Management depends on the cause of the nipple discharge.
Nipple retractionTypes
Simple nipple retraction:It occurs at puberty .
Recent nipple retraction (it’s suspicious) :It occurs later in life.
Simple nipple retraction
It’s of unknown etiology.It may cause problems with breast feeding and infection may occur, especially during lactation due to retention of secretions.
Treatment
Usually unnecessary, the condition may correct itself.
Simple cosmetic surgery can be done to correct the cause ,but it can damage the ducts.
Recent retraction of the nipple
It’s a serious pathological condition. Occurs later in life.A slit -like retraction of the nipple may be caused by :
Duct ectasia
Chronic periodical mastitis
Circumferential retraction with or without an underlying lump, may well indicate an underlying carcinoma.
It is dilatation of lactiferous ducts with or without periductal inflammation, therefore, also known as periductal mastitis.
More common in smokers.
Pathology• Dilatation of duct is followed by filling of the ducts with brown or green fluid which produces the nipple discharge.
• These fluids stimulate the inflammatory reaction and lead to periductal mastitis.
• If not checked at this stage, it can also lead to abscess or mammary duct fistula formation.
• Chronic mastitis can lead to fibrosis and result in recent onset nipple retraction.
This chronic mastitis and associated mass can mimic carcinoma.
Clinical featuresIt can present as any type of nipple discharge, or as mammary duct fistula, abscess or nipple retraction.
Management
• Antibiotics are started once the diagnoses is established . The most appropriate agents being co-amoxiclav or flucloxacilin and metronidazole.• Cessation of smoking.
• Hadfield operation (Radical duct excision) is the operation of choice.
Recurrent periductal mastitis is called Zuska’s disease.
Management is with incision and drainage, antibiotics and cessation of smoking.



Paget’s disease of nipple is a cutaneous marker of underlying malignancy either invasive or in situ ductal lesion.
It is unilateral and rarely bilateral chronic eczematous eruption of nipple which can progress to ulcerated weeping lesion.
The underlying lesion may be palpable or nonpalpable.
PathologyPaget cell: Large cell, pale staining, with round nuclei and large nucleoli.
They migrate from the nipple to lactiferous sinus to underlying breast epithelium.
But never invade the basement membrane on their own.
Differential diagnoses• Eczema: It is bilateral. No underlying lump is present in eczema.
• Superficial spreading melanoma. Paget’s is CEA positive whereas melanoma is S100 positive.
Management
Mammogram/USG, biopsy to establish the diagnoses.Treatment is with simple mastectomy.
Further management depends on the
histopathology report.Key Points
■ Common symptoms of breast problems may include a mass or lump, pain and nipple discharge.■ The ‘triple test’ includes the clinical examination, radiological imaging studies and tissue sampling.
■ A detailed history must include a discussion of the presenting problem, any previous breast problems, a detailed gynaecological history and a family history.
• The physical examination includes a detailed inspection and palpation of the breasts and axilla, with the patient in both the sitting and supine positions.
• Benign breast disease is a common entity in women aged 20–40 and covers a wide spectrum of conditions.
• Supportive diagnostic tools for evaluating breast lesions include mammography, ultrasound, MRI, FNA and core needle biopsy.