HERNIA
Professor
Dr. Mohanned Alshalah
LEARNING OBJECTIVES
Basic anatomy of the abdominal wall and its
weaknesses
Causes of abdominal hernia
Types of hernia and classifications
Clinical history and examination finding in hernia
To know and understand:

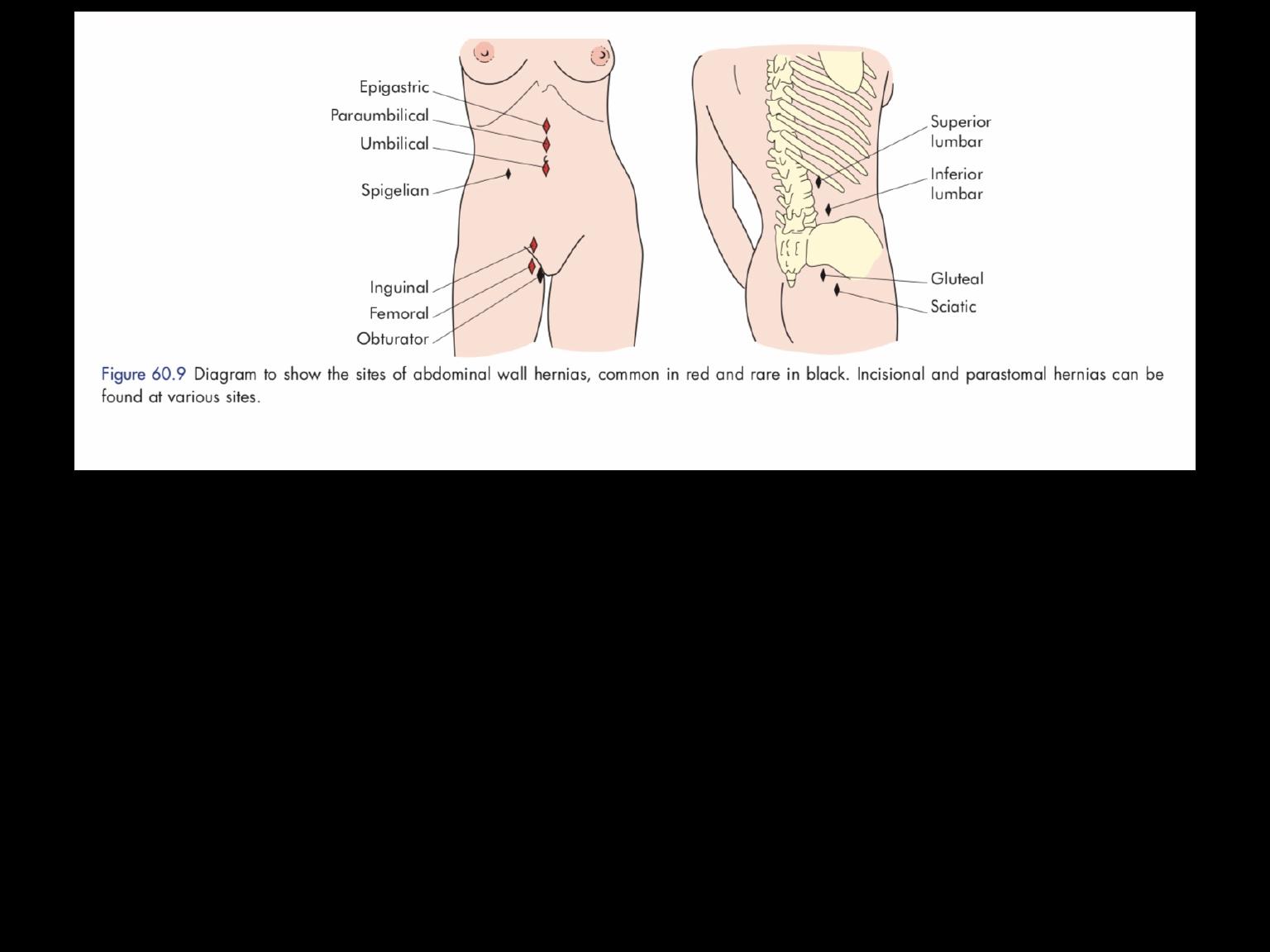
A hernia is the bulging of part of the contents of the
abdominal cavity through a weakness in the
abdominal wall.
Types of hernia by complexity
■ Occult – not detectable clinically; may cause severe
pain
■ Reducible – a swelling which appears and
disappears
■ Irreducible – a swelling which cannot be replaced in
the abdomen, high risk of complications
■ Strangulated – painful swelling with vascular
compromise, requires urgent surgery
■ Infarcted – when contents of the hernia have
become gangrenous, high mortality
Causes of hernia
■ Basic design weakness
■ Weakness due to structures entering and leaving the
abdomen
■ Developmental failures
■ Genetic weakness of collagen
■ Sharp and blunt trauma
■ Weakness due to ageing and pregnancy
■ Primary neurological and muscle diseases
■ ? Excessive intra-abdominal pressure
Aetiology
• Multi-factorial process
•
Technique is not the sole cause
•
Primary fascial pathology due to
1-2
:
- Abnormal collagen metabolism and production (found even in sites
remote from hernia)
- Increased matrix metalloproteinase (MMP) activity
•
Secondary fascial pathology due to:
- loss of normal tissue architecture
-replacement of fascial planes with scar
•
Mechanotransduction
- mechanical forces (coughing, straining, stretching) induce changes
in fibroblast function
3-4
- loss of this during primary healing leads to weaker tissue
- early laparotomy failure has significant incidence of recurrent
hernia
1. Read RC. Hernia 2006;10(6):454–5.
2. Peacock J. Fascia and muscle. Wound repair. 3rd edition. Philadelphia:W.B. Saunders; 1984. p. 332–62
3. Skutek M. Eur J Appl Physiol 2001;86(1):48–52
4. Katsumi A. J Biol Chem 2005;280(17):16546–9
Collagen I and III
•
Collagen Type I – mature collagen, greatest
strength component of ECM
•
Collagen Type III – immature isoform,
weaker, less crosslinking
•
Low ratios of CI:CIII have been
demonstrated in scar plates of recurrent
hernias
1. Read RC. Hernia 2006;10(6):454–5.
2. Peacock J. Fascia and muscle. Wound repair. 3rd edition. Philadelphia:W.B. Saunders; 1984. p. 332–62
3. Skutek M. Eur J Appl Physiol 2001;86(1):48–52
4. Katsumi A. J Biol Chem 2005;280(17):16546–9
MMP-2
•Encoded by MMP2 gene
•Involved with tissue remodeling
•Breakdown collagen and
otherextracellular matrix proteins
•Found to be elevated in patients
with recurrent hernias
1
1. Smigielski J. Eur J Clin Invest. 2011 Feb 8. Epub
2. Shumpelick. Recurrent Hernias. Page 66-68. 2007.
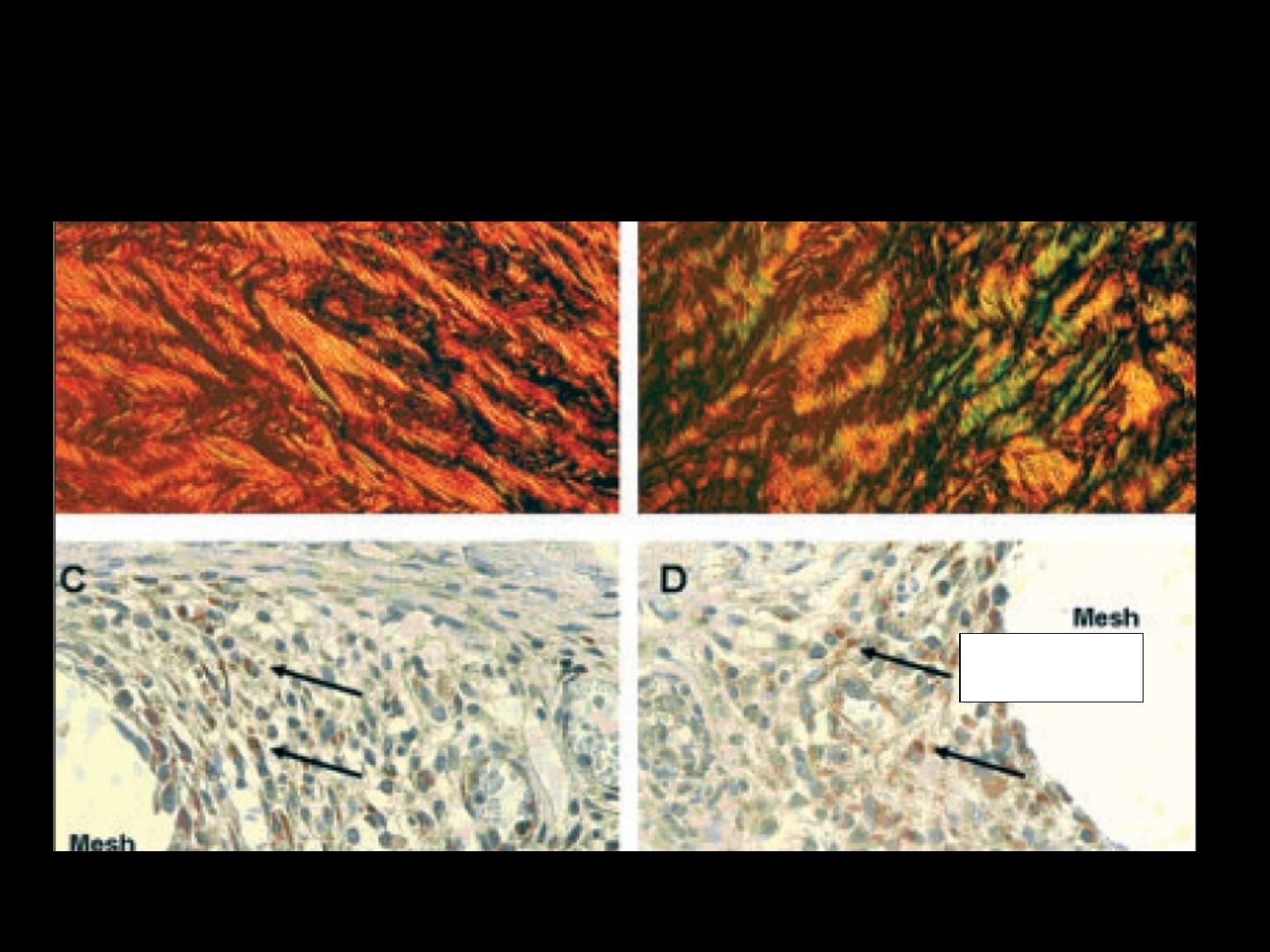
Collagen and MMP2s
CI/III - 14
CI/III – 3.6
MMP2
•
Checks
•
■ Reducibility
•
■ Cough impulse
•
■ Tenderness
•
■ Overlying skin colour changes
•
■ Multiple defects/contralateral side
•
■ Signs of previous repair
•
■ Scrotal content for groin hernia
•
■ Associated pathology
Clinical history and diagnosis in hernia cases
Patients are usually aware of a lump on the abdominal
wall under the skin.
The hernia is usually painless but patients may
complain of an aching or heavy feeling.
Sharp, intermittent pains suggest pinching of tissue.
Severe pain should alert the surgeon to a high risk of
strangulation.
One should determine whether the hernia reduces
spontaneously or needs to be helped.
The patient should be asked about symptoms which
might suggest bowel obstruction.
Examination
■ A swelling with a cough impulse is not
necessarily a hernia
■ A swelling with no cough impulse may still
be a hernia
Investigations
■ Plain x-ray – of little value
■ Ultrasound scan – low cost, operator dependent
■ CT scan – incisional hernia
■ MRI scan – good in sportsman’s groin with pain
■ Contrast radiology – especially for inguinal
hernia
■ Laparoscopy – useful to identify occult contra
lateral inguinal hernia
Emergency Hernia Surgery
•
Emergency
Strangulated
Incarcerated
Obstructed
•
Urgent
tender
irreducible
Management
■ Not all hernias require surgical repair
■ Small hernias can be more dangerous
than large
■ Pain, tenderness and skin colour changes
imply high risk of strangulation
■ Femoral hernia should always be
repaired
1. Reduction of the hernia content into the
abdominal cavity with removal of any non-
viable tissue and bowel repair if necessary;
2. Excision and closure of a peritoneal sac if
present or replacing it deep to the muscles;
3. Reapproximation of the walls of the neck of the
hernia if possible;
4. Permanent reinforcement of the abdominal
wall defect with sutures or mesh
All surgical repairs follow the same
basic principles:
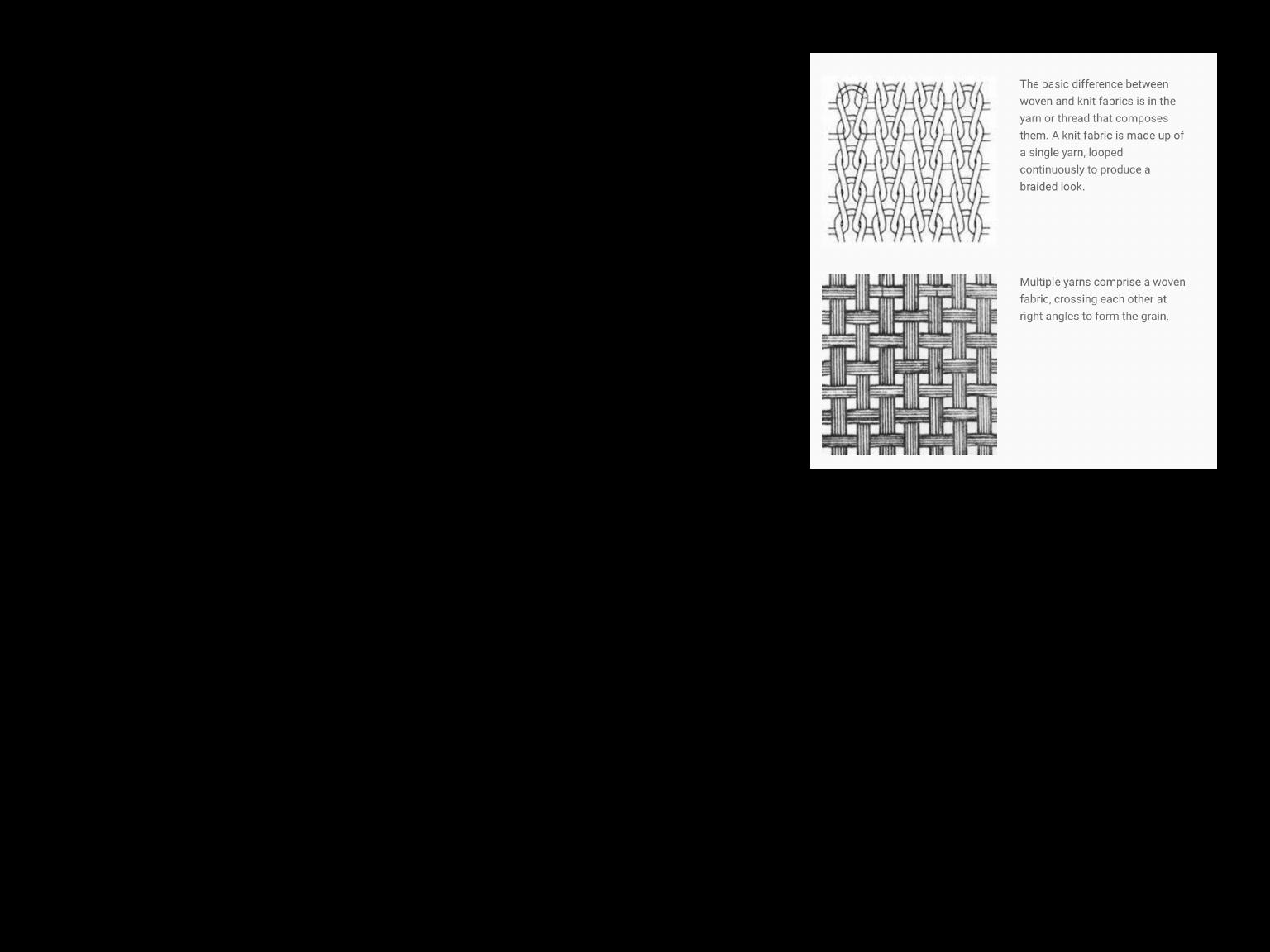
Mesh characteristics
■ Woven, knitted or sheet
■ Synthetic or biological – mainly
synthetic
■ Light, medium or heavyweight –
lightweight becoming more popular
■ Large pore, small pore – large
pore causes less fibrosis and pain
■ Intraperitoneal use or not – non-
adhesive mesh on one side
■ Non-absorbable or absorbable –
mainly non-absorbable
All meshes provoke a fibrous reaction
More dense or heavyweight meshes provoke a greater
reaction leading to collagen contraction and stiffening
and mesh shrinkage.
This can lead to tissue tension and pain, a common
complication of mesh repair.
It can also lead to hernia recurrence if the mesh no
longer covers the defect.
EMERGENCY HERNIA SURGERY
•
Femoral
•
Inguinal
•
Umbilical
•
Spigelian
•
Obturator
•
Incisional
•
Parastomal
•
Groin disruption
Epidemiology
(Adults)
Hernia
•
Inguinal
•
Incisional
•
Femoral
•
Umbilical
•
Epigastric
•
Other
%
80
10
5
4
<1
<1
Epidemiology
Hernia
•
Inguinal
•
Femoral
•
Umbilical
•
Other
Male %
Female %
96
45
2
39
1
15
1
1
Right-sided groin hernias are more common than on
the left
EMERGENCY HERNIA SURGERY
Case Study 1
•
85 years Female 55Kg
•
Painful red and tender Right groin lump ? Femoral
•
Abdominal distension and vomiting
•
Hypotensive, AKI, Septic
•
High lactate
•
Small bowel dilatation on AXR
Management ?
What operation?
EMERGENCY HERNIA SURGERY
Case Study 2
•
65 years Female 55Kg
•
Painful tender Right groin lump ? Inguinal ? femoral
•
Soft abdomen, non distended, non tender
•
No history of vomiting
•
Normotensive
•
U & E’s normal
•
Normal lactate
Management ?
What operation?
EMERGENCY HERNIA SURGERY
Case Study 3
•
75 years Male 75Kg
•
Painful tender Right groin lump ? Inguinal
•
Tender distended abdomen
•
History of vomiting
•
Hypotensive
•
AKI
•
High lactate
Strangulated loop of small bowel at open inguinal
exploration
What operation?