
Learning objectives
•
Pathophysiology ,presentation and
management of mastitis
•
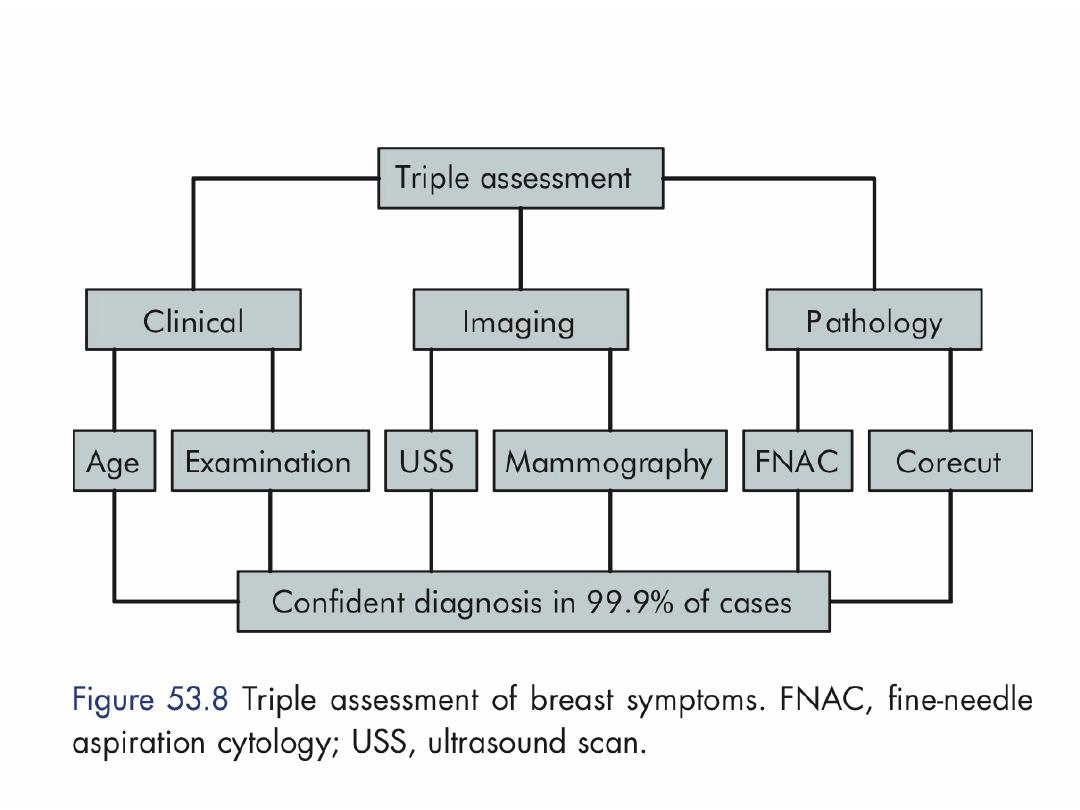
Diagnosis of Breast Cancer
•
Breast Cancer Staging and Biomarkers
•
Overview of Breast Cancer Therapy
•
Breast Surveillance
• Communication skills in breast cancer
• Gynecomastia

Acute and subacute inflammations of the
breast
Bacterial mastitis
Bacterial mastitis is the commonest variety of
mastitis and associated with lactation in the
majority of cases.
Some of these will be associated with an infected
haematoma or with periductal mastitis .

Aetiology :
Most cases are caused by Staphylococcus aureus.
The intermediary is usually the infant.
Ascending infection from a sore and cracked
nipple may initiate the mastitis.
Blockage of the lactiferous ducts by epithelial
debris leading to stasis — this theory is supported
by the relatively high incidence of mastitis in
women with a retracted nipple.

Clinical features
The affected breast presented with the classical signs of
acute inflammation.
Early on this is a generalised cellulitis, but later an
abscess will form.
Treatment
In the cellulitic stage the patient should be treated with
an appropriate antibiotic, e.g. flucloxacillin or co
amoxiclav.
Feeding from the affected side may continue if the
patient can manage.
Support of the breast, local heat and analgesia will help
to relieve pain.


The breast should be incised and drained if the
infection did not resolve within 48 hours or if after
being emptied of milk there was an area of tense
induration or other evidence of an underlying
abscess.
This advice has been replaced with the
recommendation that repeated aspirations under
antibiotic cover (if necessary using ultrasound) be
performed.
This often allows resolution without the need for an
incision scar and will also allow the patient to carry
on breast-feeding.

Operative drainage of a breast abscess
Incision of a lactational abscess is necessary if
there is marked skin thinning and can usually be
performed under local anaesthesia.
The usual incision is sited in a radial direction
over the affected segment, although if a
circumareolar incision will allow adequate access
to the affected area this should be preferred
because of a better cosmetic result.
The wound may then be lightly packed with
ribbon gauze or a drain inserted to allow
dependent drainage.
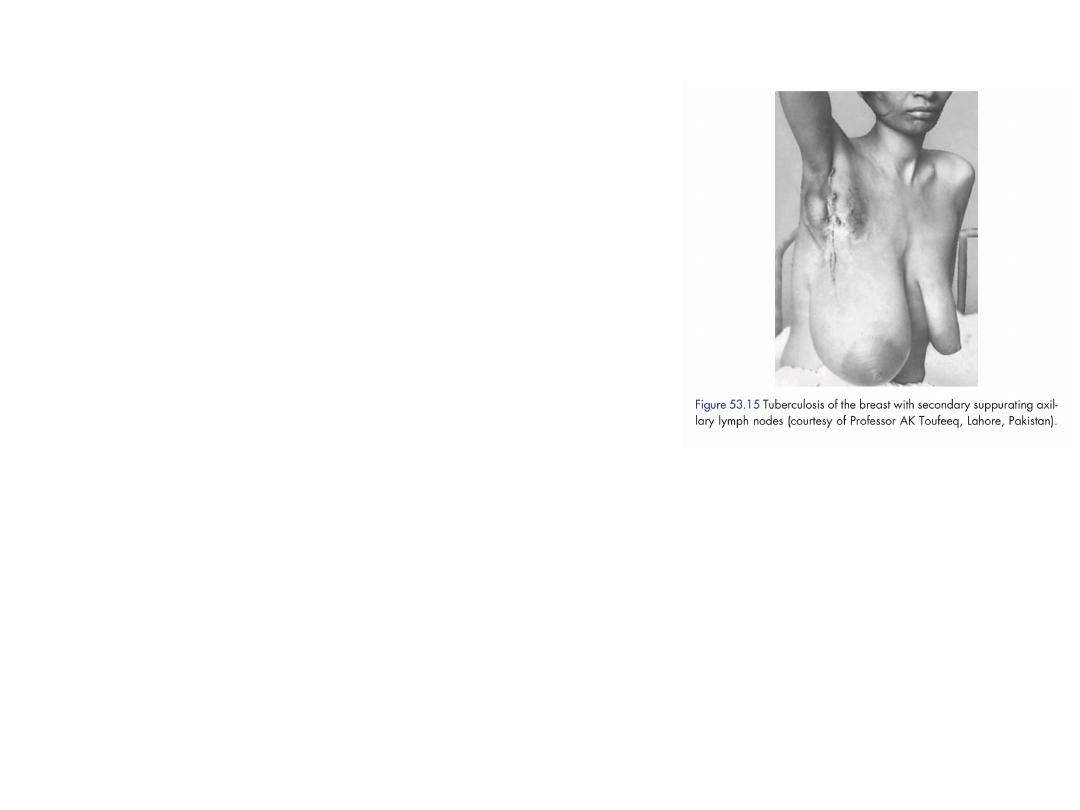
Tuberculosis of the breast
Tuberculosis of the breast is usually associated
with active pulmonary tuberculosis or
tuberculous cervical adenitis.
Tuberculosis of the breast occurs more often in
parous women and usually presents with multiple
chronic abscesses and sinuses and a typical bluish
attenuated appearance of the surrounding skin.
The diagnosis rests on bacteriological and
histological examination.
Treatment is with antituberculous chemotherapy.
Healing is usual although often delayed, and
mastectomy should be restricted to patients with
persistent residual infection.
Actinomycosis
Actinomycosis of the breast is rarer still.
The lesions present the essential characteristics
of faciocervical actinomycosis.

Mondor’s disease is
thrombophlebitis of the
superficial veins of the breast
and anterior chest wall.
The differential diagnosis
is
lymphatic permeation from an
occult carcinoma of the breast.
The only treatment required is
restricted arm movements, and
in any case the condition
subsides within a few months
without recurrence,
complications or deformity.

Breast cancer is the commonest cause
of death in middle-aged women and
accounting 3—5 per cent of deaths

Aetiological factors
I. Geographical. It occurs commonly in the Western world
accounting for 3—5 per cent of deaths, yet is a rare tumour in
Japan. In developing countries it accounts for 1—3 per cent of
deaths.
2. Age. Carcinoma of the breast is extremely rare below the
age of 20, but thereafter the incidence steadily rises so that by
the age of 90 nearly 20 per cent of women are affected.
3. Gender. Less than 0.5% of patients with breast cancer are
male.
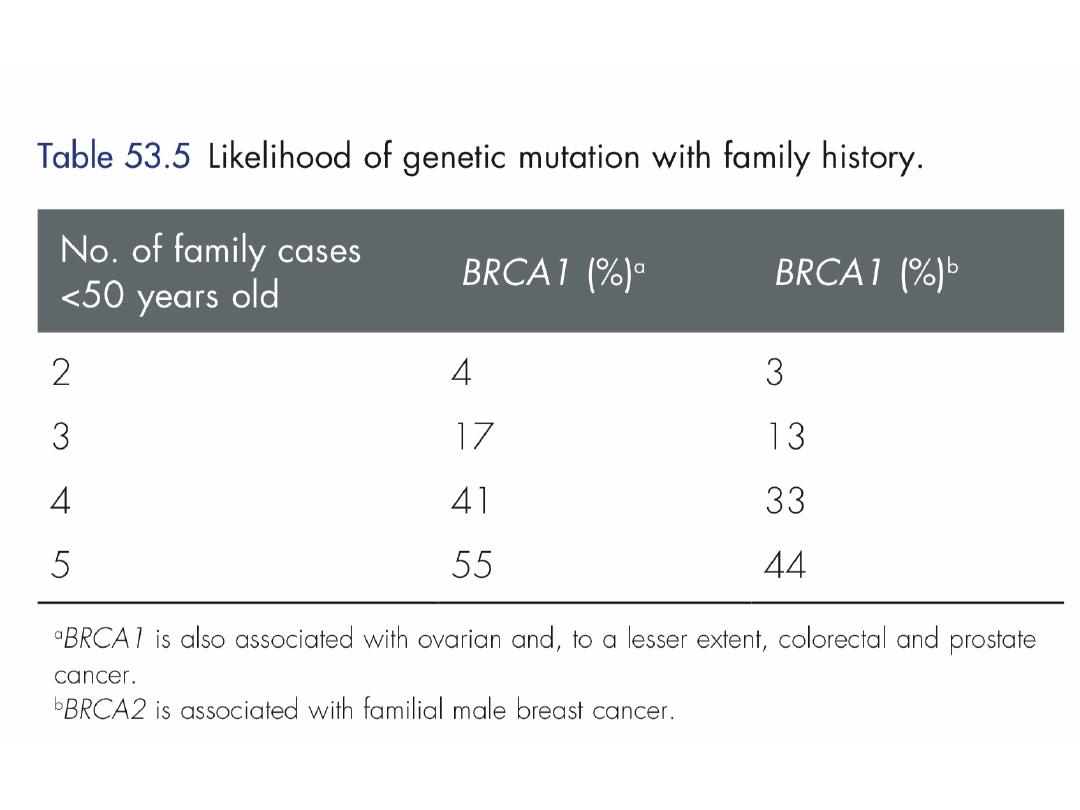
4. Genetic. It occurs more commonly in women with a family
history of breast cancer than in the general population. Breast
cancer related to a specific mutation accounts for
about 5 per cent of breast cancers.

5. Diet. There is some evidence that there is a link between diets
low in phyto-oestrogens. A high intake of alcohol is associated
with an increased risk of developing breast cancer.
6. Endocrine. Breast cancer is commoner in nulliparous women and
breastfeeding in particular appears to be protective. Also protective is
having a first child at an early age, especially if associated with late
menarche and early menopause.
It is known that in postmenopausal women, breast cancer is more
common in the obese. This is thought to be because of an increased
conversion of steroid hormones to oestradiol in the body fat.
Recent studies have clarified the role of exogenous hormones, in
particular the oral contraceptive pill and HRT, in the development of
breast cancer.
For most women the benefits of these treatments will far outweigh the
small putative risk; however, long-term exposure to the combined
preparation of HRT does significantly increase the risk of developing
breast cancer.

Previous radiation The risk appears about a decade
after treatment and is higher if radiotherapy occurred
during breast development
Abnormality
Relative risk
Nonproliferative lesions of the breast
No increase risk
Sclerosing adenosis
No increase risk
Intraductal papilloma
No increase risk
Florid hyperplasia
1.5 to 2-fold
Atypical lobular hyperplasia
4-fold
Atypical ductal hyperplasia
4-fold
Lobular carcinoma in situ
10-fold
Atypical ductal hyperplasia
10-fold
Cancer risk associated with benign breast disorders and in
situ carcinoma of the breast
Pathology
Breast cancer may arise from the epithelium of the duct system anywhere
from the nipple end of major lactiferous ducts to the terminal duct unit
which is in the breast lobule.
1.Ductal carcinoma is the most common variant
2.lobular carcinoma occurs in up to 15 per cent of cases. Invasive lobular
carcinoma is commonly multifocal and/or bilateral.
Rarer histological variants, usually carrying a better prognosis, include :
3.colloid carcinoma whose cells produce abundant mucin,
4.medullary carcinoma with solid sheets of large cells often associated with a
marked lymphocytic reaction and
5.tubular carcinoma.
6.Inflammatory carcinoma is a fortunately rare, highly aggressive cancer
which presents as a painful, swollen breast, which is warm with cutaneous
oedema.
This is due to blockage of the subdermal lymphatics with carcinoma cells.
A biopsy will confirm the diagnosis and show undifferentiated carcinoma
cells.

In situ carcinoma is preinvasive cancer which has
not breached the epithelial basement membrane.
In situ carcinoma may be ductal (DCIS) or lobular
(LCIS), the latter often multifocal and bilateral.
Both are markers for the later development of
invasive cancer which will go on to develop in at
least 20 percent of cases.
Although mastectomy is curative, this is
overtreatment in many cases and the best
treatment for in situ carcinoma is the subject of a
number of clinical trials.

Staining for oestrogen and progesterone receptors is
now considered routine, as their presence will
indicate the use of adjuvant hormonal therapy with
tamoxifen or the newer aromatase inhibitors .
Tumours are also stained HER2/neu (a growth factor
receptor) as patients who are positive can be treated
with the monoclonal antibody trastuzumab
(Herceptin), either in the adjuvant or relapse setting.


The spread of mammary carcinoma
1.Local spread: The tumour increases in size and invades
other portions of the breast. It tends to involve the skin
and to penetrate the pectoral muscles, and even the chest
wall.
2.Lymphatic metastasis: occurs primarily to the axillary
lymph nodes and to the internal mammary chain of lymph
nodes.
In advanced disease there may be involvement of
supraclavicular nodes and of any contralateral lymph
nodes.
3. Spread by the bloodstream: It is by this route that
skeletal metastases occur (in order of frequency) in the
lumbar vertebrae, femur, thoracic vertebrae, rib and skull;
they are generally osteolytic.
Metastases may also occur in the liver, lung and brain, and
occasionally the adrenal glands and ovaries.

The multidisciplinary team approach
Good doctor–patient communication plays a vital
role in helping to alleviate patient anxiety.
Participation of the patient in treatment
decisions
is of particular importance in breast cancer when
there may be uncertainty as to the best
therapeutic option and the desire to treat the
patient within the protocol of a controlled clinical
trial.
Advice should be available on breast prostheses,
psycho- logical support and physiotherapy, when
appropriate.

The care of breast cancer patients is
undertaken as a joint venture between the
surgeon, medical oncologist, radiotherapist and
allied health professionals such as the clinical
nurse specialist.

The basic principles of treatment of breast
cancer are to reduce the chance of local
recurrence and the risk of metastatic spread.

Algorithm for management of operable
breast cancer
Achieve local control
Appropriate surgery
■ Wide local excision (clear margins) and radiotherapy, or
■ Mastectomy ± radiotherapy (offer reconstruction – immediate or
delayed)
■ Combined with axillary procedure
■ Await pathology and receptor measurements
■ Use risk assessment tool; stage if appropriate
Treat risk of systemic disease
■ Offer chemotherapy if prognostic factors poor; include Herceptin
if Her-2 positive
■ Radiotherapy as decided above
■ Hormone therapy if oestrogen receptor or progesterone receptor
positive
Procedure
Axillary node sample
picks out a minimum of four individual lymph
nodes from the axillary fat
Axillary node clearance
(axillary lymph node
dissection)
block dissection of the axillary contents
level 1 - up to the lateral border of pectoralis
minor
level 2 - up to the medial border of pectoralis
minor
Sentinel node biopsy
selective removal of the first tumour-
draining node(s)

The sentinal node
is that lymph node designated as the
first axillary node draining the breast.
The internal mammary nodes are fewer in number and lie
along the internal mammary vessels deep to the plane of
the costal cartilages.

Systemic therapy such as chemotherapy or hormone
therapy is added if there are adverse prognostic
factors such as lymph node involvement, indicating a
high likelihood of metastatic relapse.
In locally advanced or metastatic disease is usually
treated by systemic therapy to palliate symptoms,
with surgery playing a much smaller role.

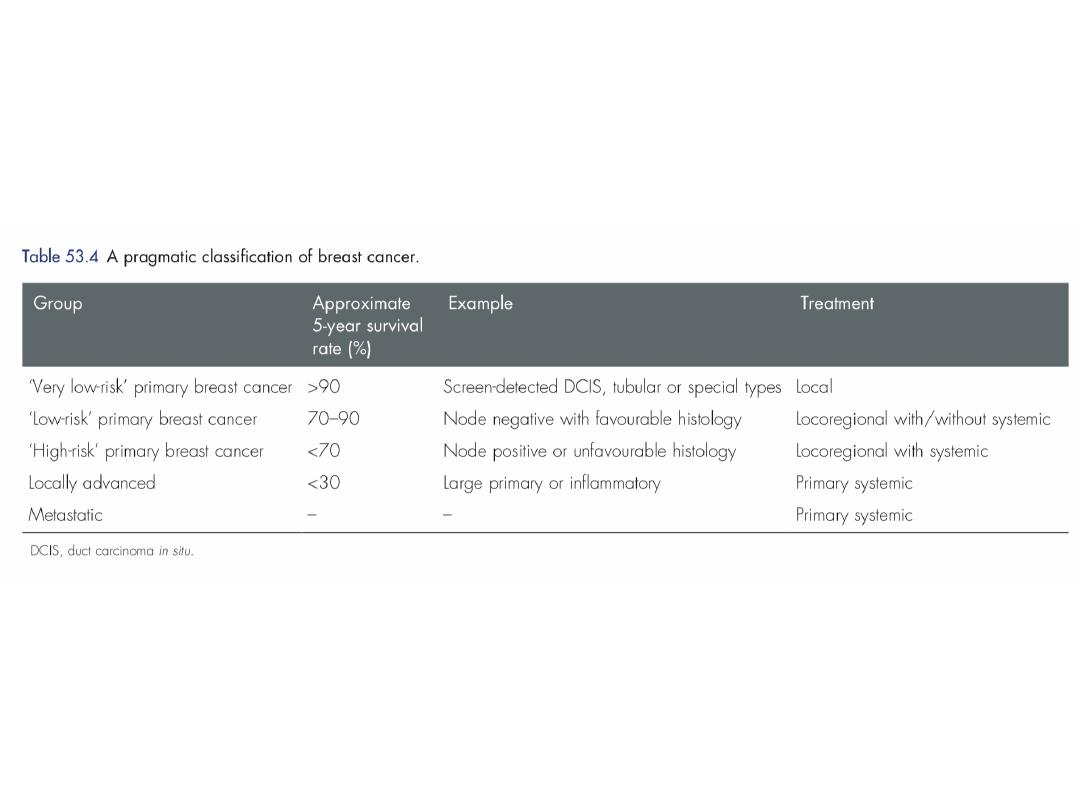
Nottingham prognostic index = (0.2* tumor size in cm)
+ tumor grade (1–3) + lymph node stage (1–3)
– Value < or = 2.4 – excellent prognosis
– Value < or = 3.4 – good prognosis
– Value < or = 5.4 – moderate prognosis
– Value > 5.4 – poor prognosis.
Prognosis

Follow-up
• Monthy self examination
• 6 monthly clinical examination and systemic
examination for 1st 2 years and yearly thereafter.
• Yearly mammogram.
• Metastatic follow-up as per the symptoms.

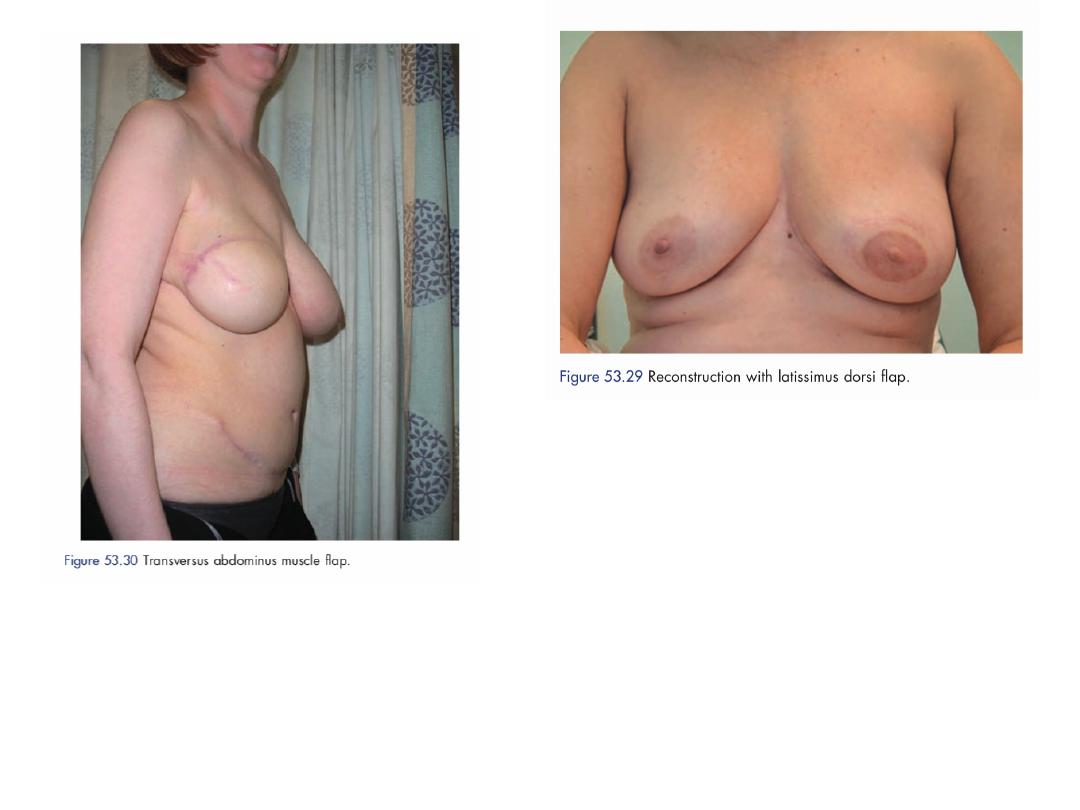
Breast reconstruction
These women can now be offered immediate or
delayed reconstruction of the breast.
The easiest type of reconstruction is using a silicone
gel implant under the pectoralis major muscle.
This may be combined with prior tissue expansion
using an expandable saline prosthesis first which
creates some ptosis of the new breast.

If the skin at the mastectomy site is poor (e.g.
following radiotherapy) or if a larger volume
of tissue is required, a musculocutaneous flap
can be constructed either from
• Latissimus dorsi muscle (an LD flap) or
• Transversus abdominis muscle TRAM flap

Screening for breast cancer
•
Because the prognosis of breast cancer is
closely related to stage at diagnosis so
breast screening by mammography in women
over the age of 50 years will reduce cause-
specific mortality by up to 30 per cent.
•
Three-yearly mammographic screening for
women between the ages of 50 and 64 years
(now increased to 70 years).

Familial breast cancer
•
Breast cancer is due to an inherited genetic
change actually account for less than 5 per
cent of all cases of breast cancer.
•
Those who prove to be ‘gene positive’ have a
50–80 per cent risk of developing breast
cancer, predominantly while premenopausal.
•
Many will opt for prophylactic mastectomy.

For the great majority of women with a positive
family history, who are unlikely to be carriers of
a breast cancer gene should be assessed and
followed-up.
Tamoxifen given for five years appears to reduce
the risk of breast cancer by 30–50 per cent.

Causes of gynecomastia are as follows:
Physiological
• Neonatal gynecomastia due to placental estrogens.
• Adolescent gynecomastia due to relative estrogen
excess.
• Senescent gynecomastia due to relative
testosterone deficiency.
Pathological
• Idiopathic—mc
• Estrogen excess
Gynecomastia

Primary testicular failure
− Anorchia, Klinefelter syndrome,
testicular feminization syndrome
Secondary testicular failure
− Orchitis, trauma, castration, leprosy, − Renal failure
− Myotonic dystrophy or spinal cord
injury
Increased testicular production
− Testicular tumors (Leydig cell, sertolicell, granulose/ theca cell
tumor)
− Bronchogenic carcinoma and
transitional cell tumor of urinary tract
Increased aromatization
− Adrenal hyperplasia or carcinoma
− Cirrhoses, thyrotoxicoses, exogenous androgen administration

•
Common Drugs
(DOC4KS )
Digitalis, oral
contraceptive pills, cimetidine,
clomiphene, captopril, calcium channel
blockers, ketoconazole, spironolactone.
•
Other drugs: Isoniazid, tricyclic
antidepressants, methyldopa, flutamide.
Grade 1
Mild enlargement, no skin
redundancy
Grade 2A
Moderate enlargement, no
skin redundancy
Grade 2B
Moderate enlargement, skin
redundancy
Grade 3
Marked enlargement with
skin redundancy and ptosis
Simon grading

Investigations
History and physical examination.
Evaluate testis: Testicular ultrasound,
serum testosterone, LH, DHEAS,
endocrine profile—estrogen, prolactin,
adrenal CT.
Thyroid function tests.
Breast mammogram, ultrasound,
biopsy.
Liver function test, abdominal CT.

Treatment
1. Stop offending drug.
2. Treat the systemic disease, if present.
3. Karyotyping for klinfelter if positive, consider bilateral
mastectomy.
4. Most cases resolve spontaneously and 1 year observation
period is suggested.
5. Pharmacology during observation: Tamoxifen, danazol,
aromatase inhibitors all have been used in the treatment
of gynecomastia.
6. Surgery is done for gynecomastia of long duration,
cosmetic or psychological reason, symptomatic or
suspected malignancy.
7. Simple mastectomy, subcutaneous mastectomy,
liposuction, reduction mammoplasty are all suggested
procedures.

Do you counsel your patients to perform a
monthly breast self-examination (BSE)?
Risk Factors and Screening for Early-
Onset Breast and Ovarian Cancer
What risk factors for breast or ovarian cancer should
primary care providers (PCPs) be looking for in their
patients who are women younger than age 45?

How do you tell a patient she is at
increased risk for breast cancer?
What do you tell them?
A young woman who has a family history associated with an
increased risk for the BRCA1 or BRCA2 or other gene
mutations

What preventive measures can be taken by
young women with an inherited gene mutation
associated with high risk for breast cancer?

Prophylactic bilateral mastectomy with or without
reconstructive surgery
Some women who do not want surgery may
be candidates for chemoprevention with
agents such as tamoxifen.
She needs high-risk surveillance: an exam by a
breast surgeon every 6 to 12 months and
probably yearly MRI and mammograms starting
at age 25 and 30, respectively.

Are there limitations to cancer genetic
testing?

A 32-year-old woman presents for evaluation of a lump that she noticed in
her right breast on self-examination. She says that while she does not
perform breast self-examination often, she thinks that this lump is new. She
denies nipple dis charge or breast pain, although the lump is mildly tender
on palpation. She has never noticed any breast masses previously and has
never had a mammogram. She has no personal or family history of breast
disease. She takes oral contraceptive pills (OCPs) regularly, but no other
medications. She does not smoke cigarettes or drink alcohol. She has never
been pregnant. On examination, she is a well-appearing, somewhat anxious,
and thin woman. Her vital signs are within normal limits. On breast
examination, in the lower outer quadrant of the right breast, there is a 2-
cm, firm, well-circumscribed, freely mobile mass without over lying
erythema that is mildly tender to palpation. There is no skin dimpling,
retraction, or nipple discharge. While no other discrete breast masses are
palpable, the bilateral breast tissue is noted to be firm and glandular
throughout. There is no evidence of axillary, supraclavicular, or cervical
lymphadenopathy. The remainder of her physical examination is
unremarkable.
What is the most likely diagnosis of this breast lesion?
What is the first step in evaluation?
What is the recommended follow-up for this patient?
Routine use of screening mammography in women ≥50 years of age
reduces mortality from breast cancer by 25%. MRI screening is
recommended in women with BRCA mutations and may be considered
in women with a greater than 20% to 25% lifetime risk of developing
breast cancer.
Core-needle biopsy is the preferred method for diagnosis of palpable or
nonpalpable breast abnormalities.
Sentinel node dissection is the preferred method for staging of the regional
lymph nodes in women with clinically node-negative invasive breast cancer.
Axillary dissection may be avoided in women with 1 to 2 positive sentinel
nodes who are treated with breast conserving surgery, whole breast
radiation and systemic therapy.
Local-regional and systemic therapy decisions for an individual patient with
breast cancer are best made using a multidisciplinary treatment approach. The
sequencing of therapies is dependent on patient and tumor related factors
including breast cancer subtype.