HERNIA
Lecture 2Professor
Dr. Mohanned Alshalah
LEARNING OBJECTIVES
To know and understand:• Applied anatomy of the most common groin hernia
• Pathophysiology, clinical features, Investigations and principles of management of groin HerniasFemoral Hernia

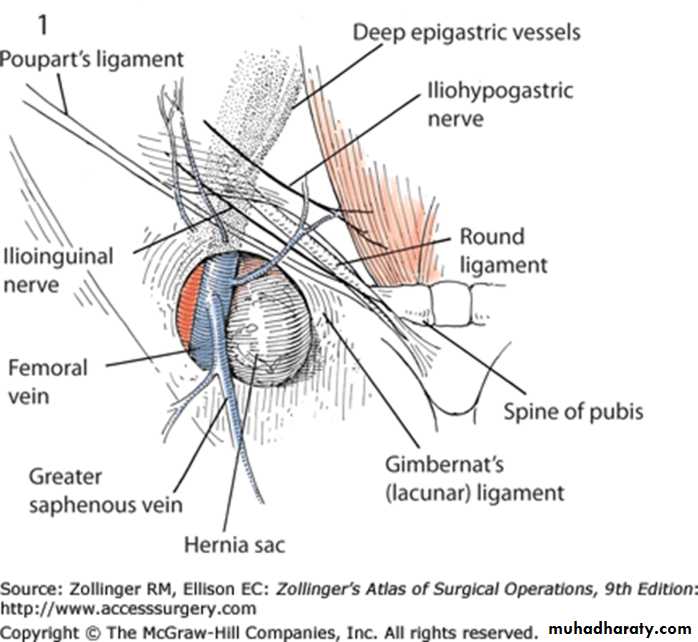
Femoral Canal Anatomy
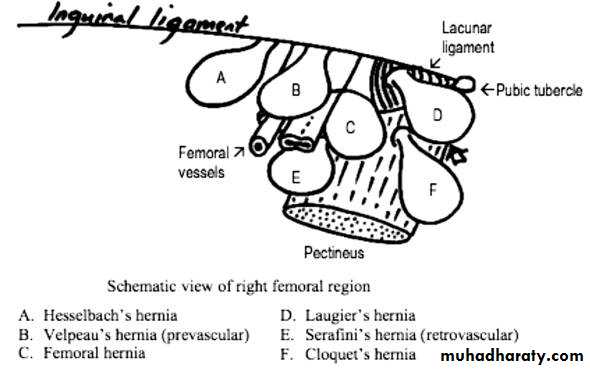
Subtypes of Femoral Hernia
Watchful Wait vs Repair
Cumulative risk of strangulation over 2 years 476 patients (439 Inguinal, 37 Femoral)34 strangulations (22 Inguinal, 12 Femoral)
•
• Cumulative Probability of Strangulation
3 months
2 yearsInguinal
2.8%
4.5%
Femoral
22.0%
45.0%
Strangulation


Richters Hernia

Femoral Hernia Repair
Mortality risk (Inguinal and Femoral)0.1% < 60 years
0.2% 60 – 69
1.6% 70 – 79
3.3% > 80 years
Emergency repair for strangulation x 10 mortality risk – overall 10%
Groin Hernia GuidelinesASGBI 2013


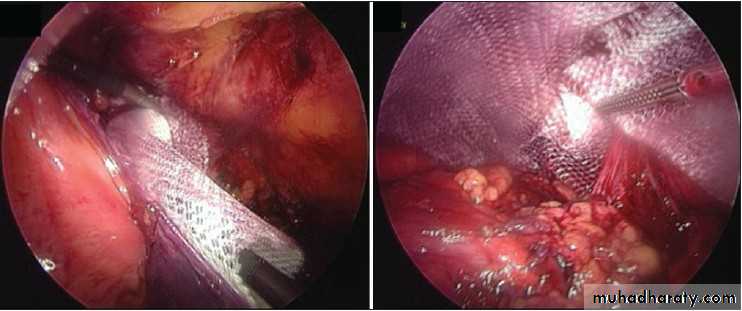
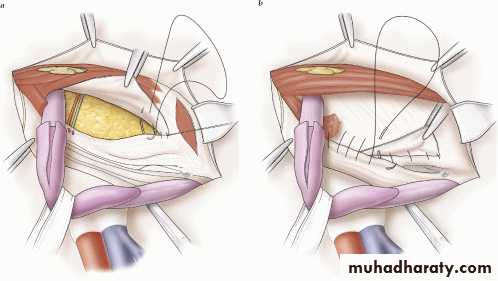
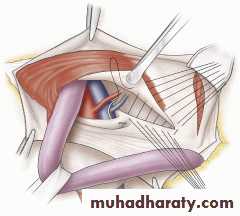
Laparoscopic Femoral Hernia Repair
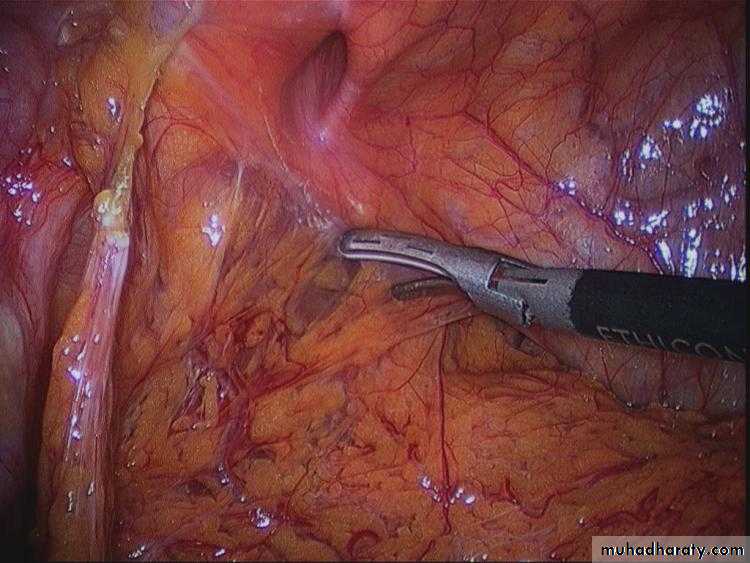
Laparoscopic Femoral Hernia Repair
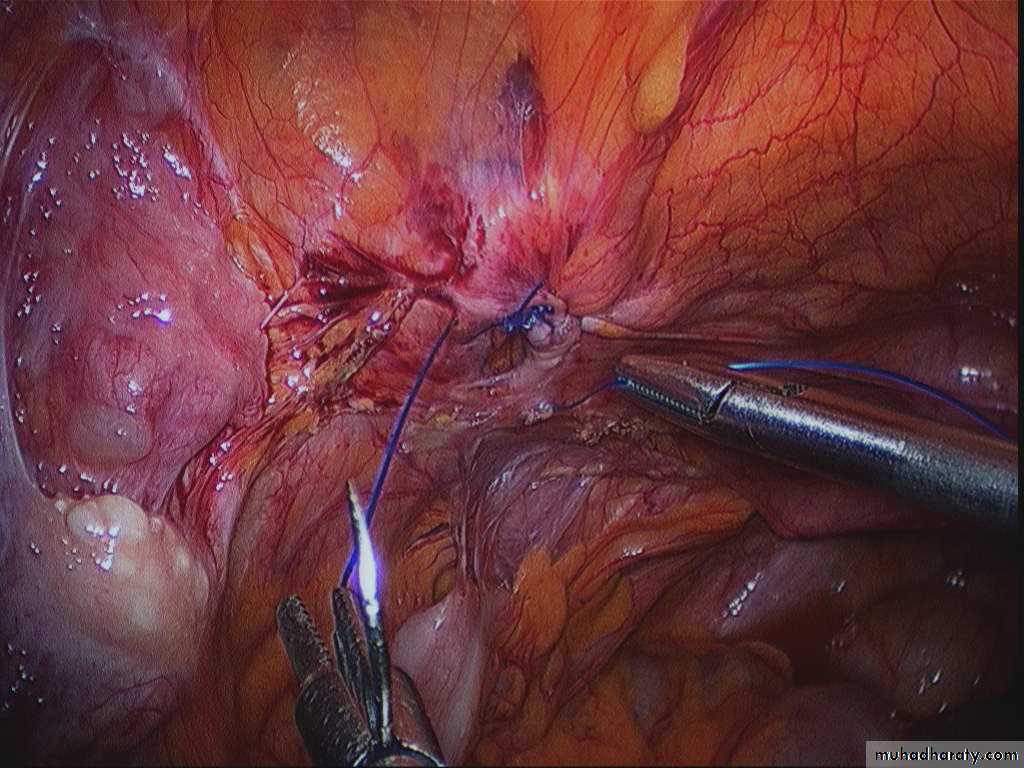
Laparoscopic Femoral Hernia Repair
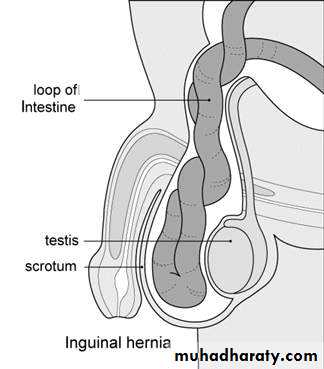
Inguinal Hernia

Nyhus Classification of Groin Hernias
Type I--indirect inguinal herniaInternal inguinal ring normal (i.e., paediatric hernia)
Type II--indirect inguinal hernia
Dilated internal inguinal ring with posterior inguinal wall intactType III--posterior wall defects
Direct inguinal herniaIndirect inguinal hernia: dilated internal ring with large medial encroachment on the transversalis fascia of the Hesselbach's triangle (i.e., massive scrotal, sliding hernia)
Femoral hernia
Type IV--recurrent hernia
Inguinal herniaEpidemiology:
• Male : Female
• by 9 to 1 ratio
• Lifetime risk Male 27%, Female 3%
• young adults mostly have indirect inguinal hernia
• As age of patient increases, the incidence of direct hernias increases
• 10% emergency surgery
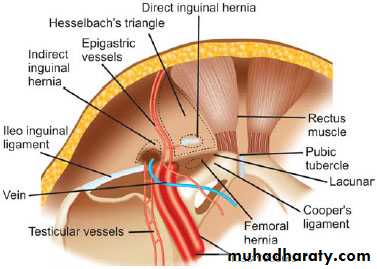
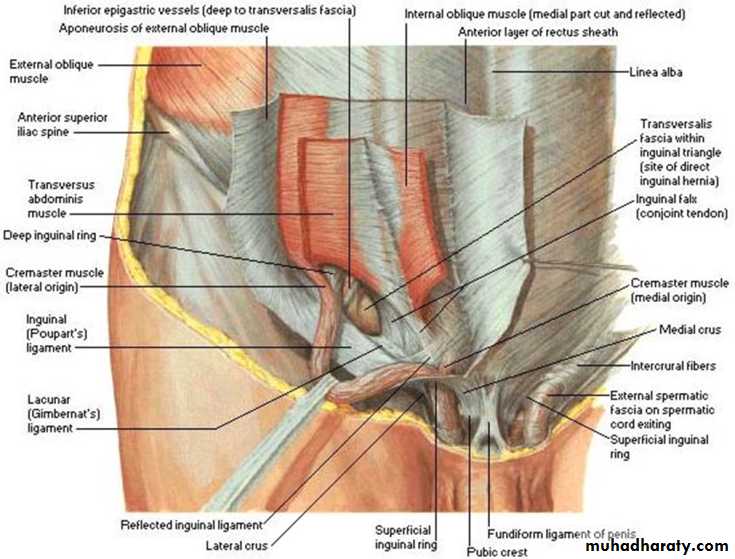
Inguinal Anatomy
Inguinal Hernia Surgery
BassiniShouldice
McVay
Lichtenstein
Preperitoneal
Laparoscopic
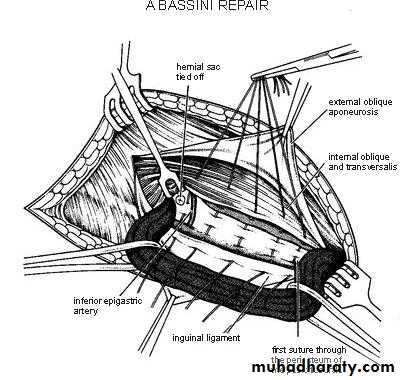
Bassini Repair (1884)
Conjoined tendon to the inguinal ligament.
Shouldice Repair (1930s)
Multilayer repair of the posterior wall of the inguinal canalDouble breasting of transversalis fascia
Transverse abdominis aponeurotic arch to the iliopubic tract and Conjoined tendon to the inguinal ligament
McVay Repair (1948)
Transverse abdominis aponeurosis to Cooper's ligament and iliopubic tract
Lichtenstein (1989)
First pure prosthetic, tension-free repair to achieve low recurrence rates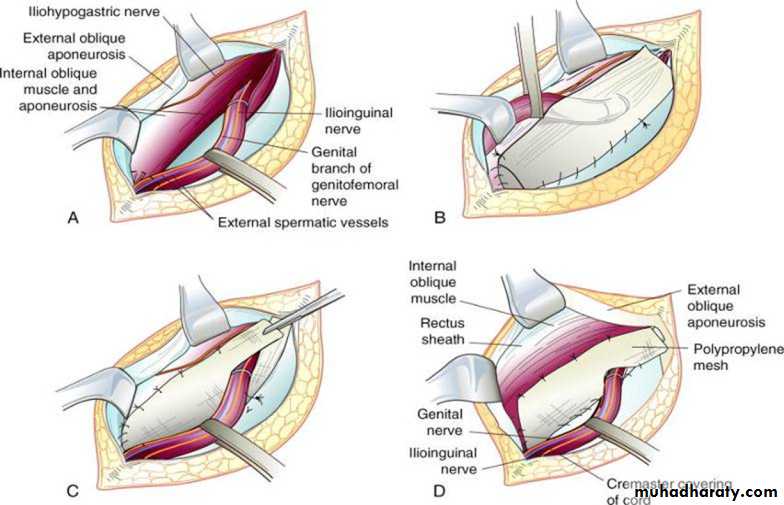
Prosthetic Repair
• Allows for a fibrotic reaction to occur between the inguinal floor and the posterior surface of the mesh, thereby forming scar and strengthening the closure of the hernia defectLaparoscopic Inguinal Hernia Repair
TAPP - transabdominal preperitoneal repair was reported in 1992, Arregui et al. (Surg Laparosc Endosc 2:53-58, 1992) and Dion and Morin (Can J Surg 35:209-212, 1992)TEP – totally extraperitoneal approach reported by Dulucq (Cahiers Chir 79:15-16, 1991)
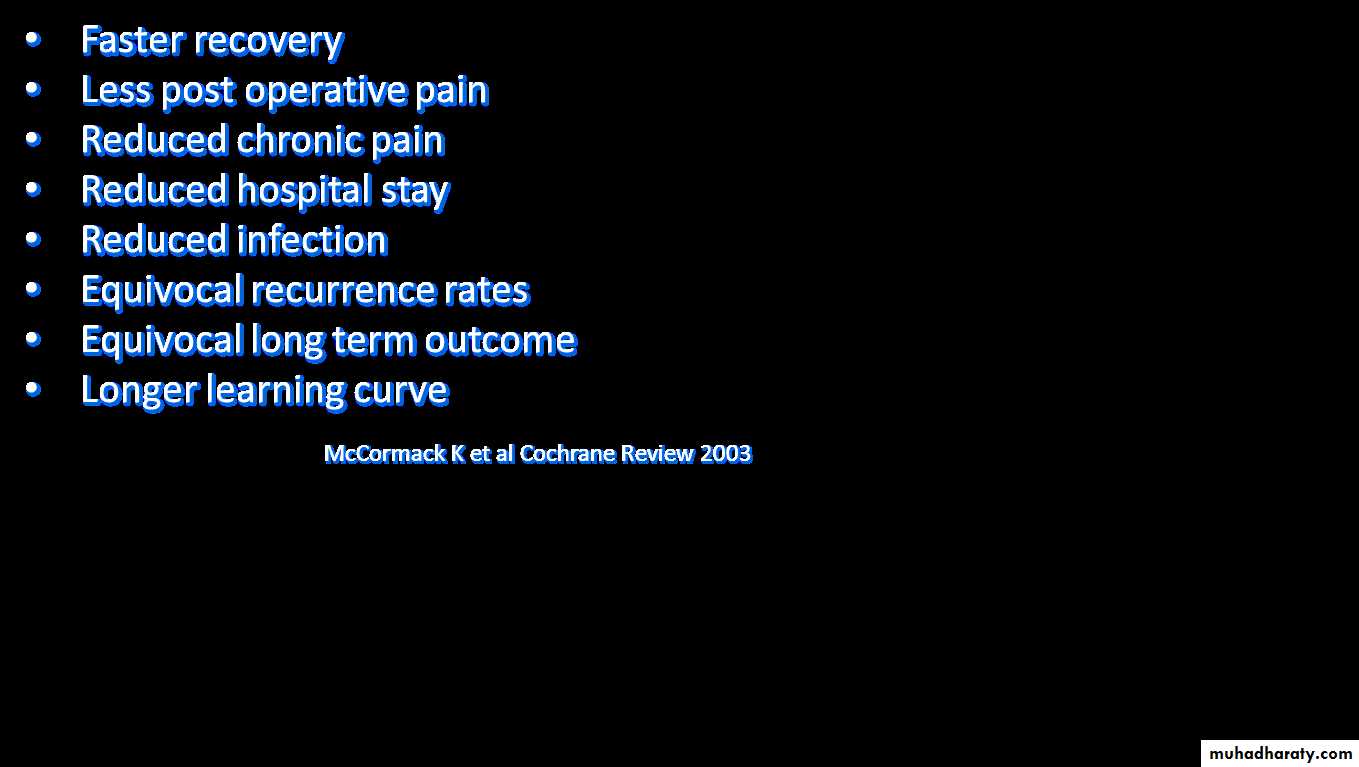
NICE guidelines on Laparoscopic Hernia – 2004• 37 RCTs were examined – Lap v open
• Lap longer operating time (13.3 min)
• Quicker return to work/ activities (3 days)
• Reduced rate of numbness (TAPP & TEP)
• NICE TA083 guidance DOH 2004
Laparoscopic Inguinal Hernia Repair
Complications of Inguinal Hernia Repair
Seroma/haematomaTesticular Ischaemia
Visceral injury
Nerve injury
• Numbness
• Chronic pain - up to 40%
• Foreign body feeling
Recurrence 1%
Mesh infection 0.2%
Mortality ‹ 1%
Comparison of open approachesRecurrence
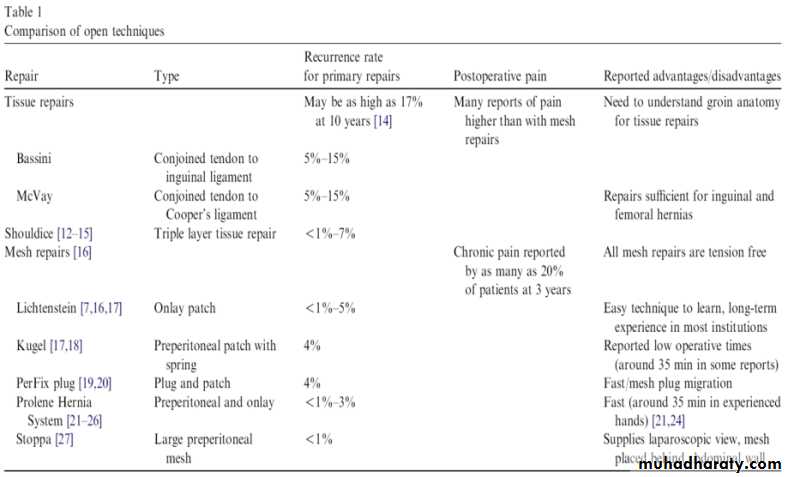
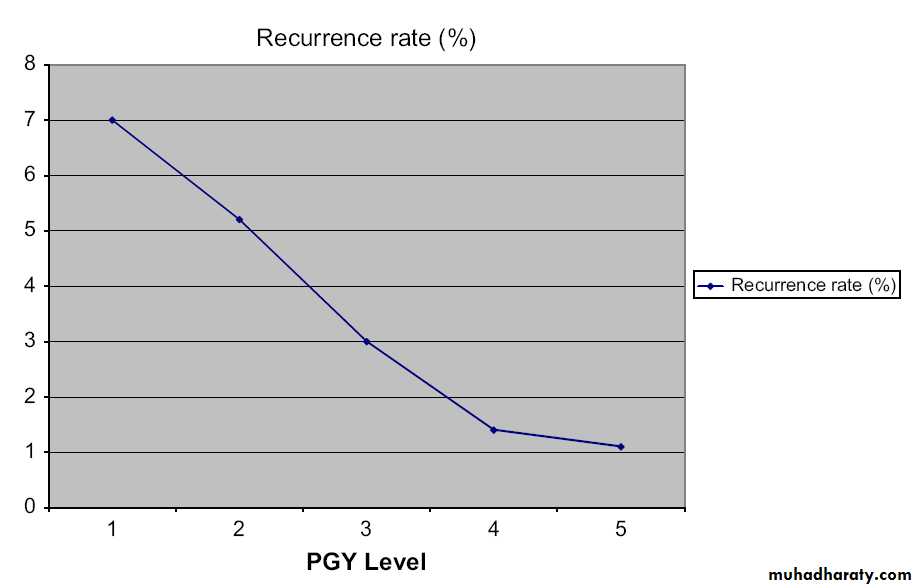
Recurrence rateSurgical Trainees

Watchful Wait vs Repair
Cumulative risk of strangulation over 2 years• 476 patients (439 Inguinal, 37 Femoral)
• 34 strangulations (22 Inguinal, 12 Femoral)
• Cumulative Probability of Strangulation
3 months
2 yearsInguinal
2.8%
4.5%
Femoral
22.0%
45.0%
Watchful Wait vs Repair
Two independent systematic reviews both concluded that watchful waiting is safe, but most patients will develop symptoms (mainly pain) over time and will require an operation
Inguinal Hernia RepairMortality
ELECTIVE• All series < 1%
• Swedish Registry – not raised above that of background population
• Danish study - 26,304 patients
0.02% <60 years, 0.48% >60 years
EMERGENCY
• 7% in Danish Study
• Swedish Registry – x7 emergency surgery
x20 bowel resection
Mortality and Groin Hernias
Women have a higher mortality risk than men, due to a greater risk for emergency procedure irrespective of hernia anatomy and a greater proportion of femoral herniasAfter a femoral hernia operation, the mortality risk was increased seven-fold for both men and women
Groin Hernia GuidelinesASGBI 2013Speed of Referral
Men, reducible, symptomatic – ROUTINEMen, irreducible – URGENT
Women – URGENT
Strangulated/obstructed - EMERGENCY
Groin Hernia GuidelinesASGBI 2013Imaging
Diagnostic uncertainty
To exclude other pathology
USS – first line
MRI – if USS neg, and groin pain persistsGroin Hernia GuidelinesASGBI 2013Indications for Surgery
Symptomatic InguinalAll Femoral hernias
Asymptomatic Inguinal – can be managed conservatively – but likely to require surgery in the future
Inguinal Hernia RepairPerioperative Antibiotics
ControversialSurgical Site Infection (SSI) rates 0 -14%
antibiotics may reduce wound infection rate
Mesh infection – 0.3 – 2%
Meta analysis/ Cochrane Reviews –
antibiotics vs controls – no significant difference in SSI or mesh infections
Routine use of prophylactic antibiotics – not recommended, except in high risk patients - >75yrs, Obesity, urinary catheter, Diabetes
Groin Hernia GuidelinesASGBI 2013Laparoscopic or Open Repair
Laparoscopic
• Younger patients
• Females• Groin pain with small hernias
• Bilateral hernias
• Recurrent (index op – Open)
• Femoral - elective
Open
• Elderly (LA)
• Comorbidity (LA)• Anticoagulants
• Large inguino-scrotal
• Hostile Abdomen
• Recurrent (index op – Lap)
Groin Hernia GuidelinesASGBI 2013Post Op Activity
“Do what you feel you can” – heavy weight lifting 2-3 weeks.Return to work – median 7 days (open and lap)
Driving – 7 days
Obturator Hernia
9 : 1 female to male ratio
Typical patient is > 70 yrs of age
Multiparous women
Up to 20% bilateral
Concurrent Femoral hernias common
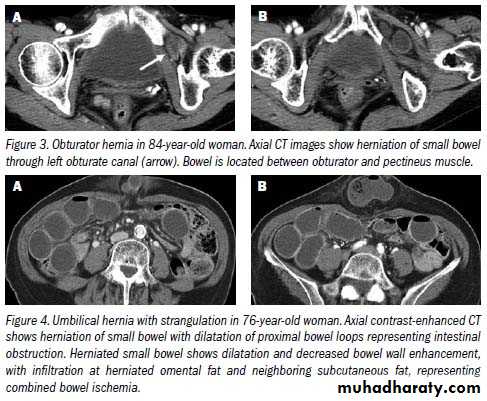
CLINICAL PRESENTATION
• Intestinal obstruction• most common presentation (80%)
• Up to 70% mortality with strangulation
• Overall mortality 25%
• Correct preoperative diagnosis in 20% to 38% of patients
ANATOMY
Formed by rami of the ischium and pubisBilaterally in anterolateral pelvic wall
Medial to the acetabulum
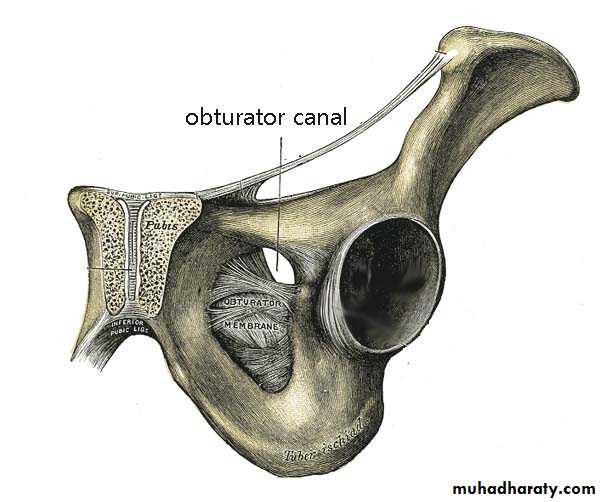
Obturator Foramen
• Covered by obturator membrane• Internal orifice closed by preperitoneal fat
• Contains obturator nerve and vessels

MRI

CT
Obturator HerniaOperative Approach
• REPAIR• Simple closure of the hernial defect with one or more interrupted sutures
• Plugging the canal with cartilage, free omentum ,obturator fascia, polypropylene mesh, teflonpatch, or bladder wall.
• Recurrence – 10% for simple closure
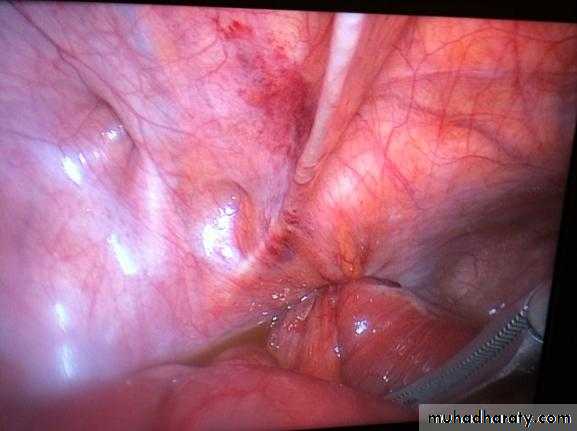
Intraoperative image showing left sided obturator hernia within white outline and incidental femoral hernia at 11’o clock position.
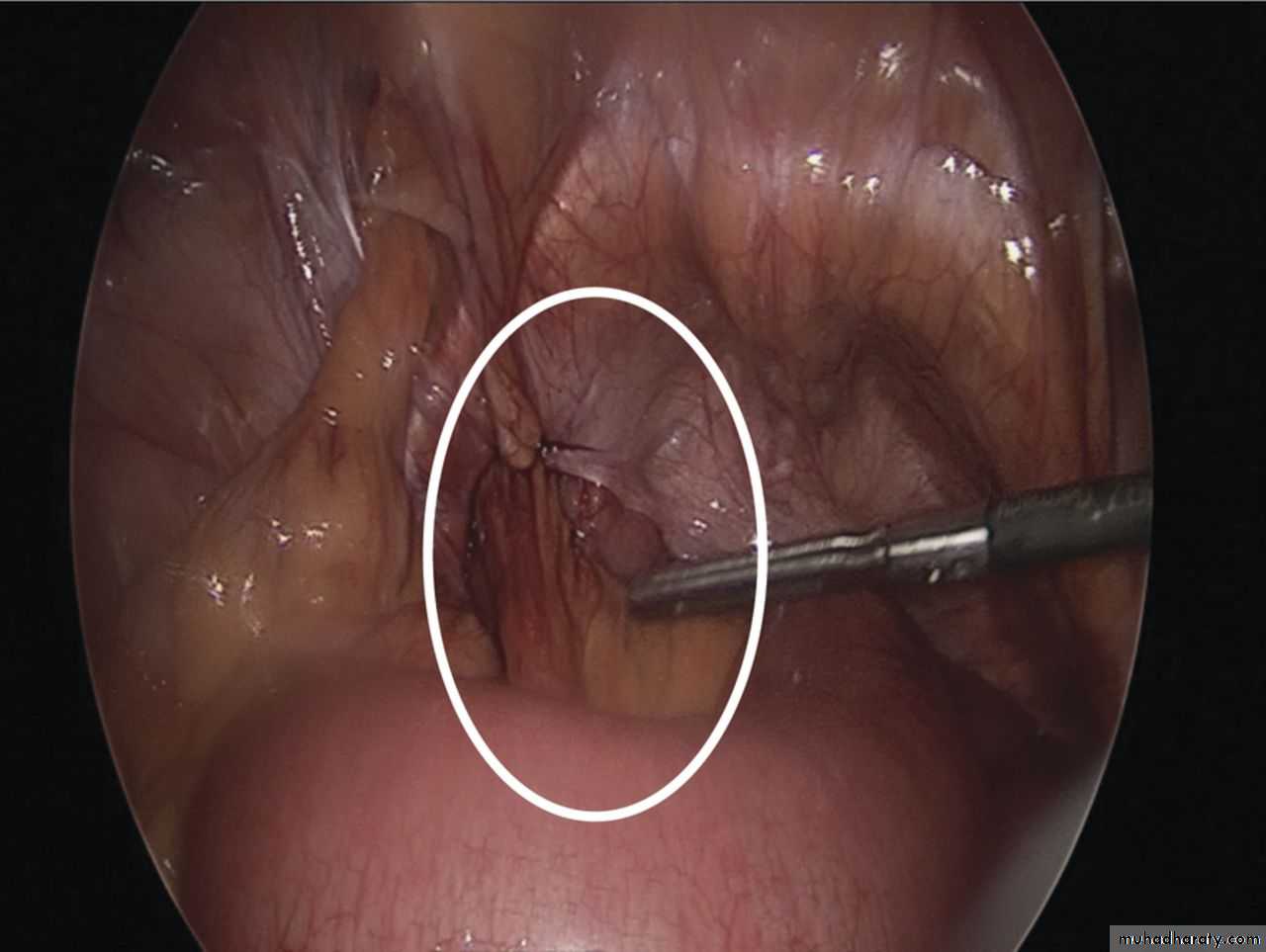
Noel P. Lynch et al. J. surg. case rep. 2013;2013:rjt050
Published by Oxford University Press and JSCR Publishing Ltd. All rights reserved. © The Author 2013.• Write a report to Identify, discuss and defend the medico-legal, socio-cultural and ethical issues when pertaining informed consent to patient presented with elective inguinal hernia.