Urethra and Penispart IDr. Wadhah A. Marzooqassisst prof. (URO)dr_wadhah_uro@yahoo.com4th stage student2020
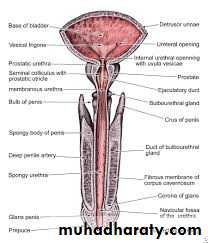
The male urethra
Anatomy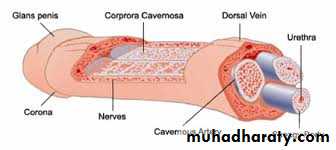
Congenital abnormalities.
APENIAMEGALOPENIS
MICROPENIS
Urethral stricture
Posterior urethral valves
Hypospadias.
Epispadias
APENIA
Congenital absence of the penis (apenia) is extremely rare. In this condition, the urethra generally opens on the perineum or inside the rectum.
Patients with apenia should be considered for assignment to the female gender. Castration and vaginoplasty should be considered in combination with estrogen treatment as the child develops.
MEGALOPENIS
The penis enlarges rapidly in childhood (megalopenis) in boys with abnormalities that increases the production of testosterone, for example, interstitial cell tumors of the testicle, congenital adrenal hyperplasia, or tumors of the adrenal cortex. Management is by correction of the underlying endocrine problem.MICROPENIS
A penis smaller than 2 standard deviations from the norm is considered a micropenis. The testicles are small and frequently undescended. Other organs, including the scrotum, may be involved. Early evidence suggests that the ability of the hypothalamus to secrete luteinizing hormone-releasing hormone (LHRH) is decreased.androgen replacement is the basic requirement. The objective is to provide sufficient testosterone to stimulate penile growth without altering growth and closure of the epiphyses.
Urethral stricture
This rare condition may be associated with duplication of the urethra. Usually, symptoms are delayed until adolescence, when it may be indistinguishable from a stricture due to unrecognized urethral injury in childhood. A single treatment by optical urethrotomy or dilatation is usually effective.Posterior urethral valves
They are usually just distal to the verumontanum but they may be within the prostatic urethra. They are flap( one way) valves and so, although urine does not flow normally, a urethral catheter can be passed without difficulty.Dilatation of the urinary tract now commonly leads to diagnosis by ultrasound scanning before birth.
Some time patient presented in the late childhood with poor urinary stream and recurrent urinary tract infection.
Posterior urethral valves need to be detected and treated as early as possible to avoid the development of renal failure.
Treatment
A suprapubic catheter is inserted to relieve the back pressure and allow the effects of renal failure to subside before definitive treatment by transurethral resection of the valves.If patient presented with impaired renal function so need treatment of uremia.
Hypospadias.
Hypospadias occurs in one in 200–300 boys and is the most common congenital malformation of the urethra.
• The external meatus opens on the underside of the penis or the perineum.
• The ventral aspect of the prepuce is poorly developed (‘hooded prepuce’).
• The penis deviated downward (chordee).

Types:
Hypospadias is classified according to the position of the meatus:• Glanular hypospadias.
• Coronal hypospadias.
• Penile and penoscrotal hypospadias.
• Perineal hypospadias.
There may be testicular maldescent, which may make it difficult to determine the sex of the child.



Treatment
Glanular hypospadias does not need treatment unless the meatus is stenosed, in which case a meatotomy is performed. Surgery is indicated for other forms of hypospadias to:• Improve sexual function.
• Correct problems with the urinary stream.
• Cosmetic reasons.
Most procedures use preputial skin and so circumcision should be avoided until the hypospadias has been repaired
Epispadias
Epispadias is very rare. In penile epispadias, the opening on the dorsum is associated with upward curvature of the penis. It may be associate with urinary incontinence.Epispadias usually coexists with bladder exstrophy and other severe developmental defects.
It usually require more than one stage corrective procedures.


Injuries to the male urethra
Rupture of the bulbar urethraThere is a history of a blow to the perineum, usually due to a fall astride a projecting object.
Clinical features
The signs of a ruptured bulbar urethra are:
• retention of urine,
• perineal haematoma .
• bleeding from the external urinary meatus.
Preliminary assessment and treatment
The patient should be treated with appropriate analgesic drugs. He should be discouraged from passing urine if rupture of the urethra is suspected. A full bladder should be drained with a catheter placed by percutaneous suprapubic puncture. This reduces urinary extravasation and allows investigations to establish the extent of the urethral injury. If the patient has passed urine when first seen and there is no extravasation, the rupture, if any, is partial and a catheter is not needed. In any case, it is probably wise to administer a course of prophylactic antibiotics.
Treatment
• Urethral cathetarization need to be avoided in patient with suspected urethal injury.• A suprapuic catheter need to be done.
• Urethrogram if available to assess the degree of injury.
• If suprapubic catheteriztion is not possible a single, soft trial of urethral cathetarivation with good lubricant and by well trained person. If any resistent is faced the procedure need to be teminated.
If the urethral tear is complete, the suprapubic catheter should remain until arrangements can be made to repair it. Some surgeons advocate immediate open repair of the urethra with excision of the traumatised section and spatulated end-to-end reanastomosis of the urethra. Others wait up to 3 months ( delayed repair) before embarking upon a repair operation.
Complications
• Subcutaneous extravasation of urine occurs in complete rupture if the patient attempts to pass urine.
• Stricture is a common sequel to urethral trauma, whether there is a partial or complete tear or simply periurethral bruising.
• Infection may also play a part.
Rupture of the membranous urethra
Intrapelvic rupture of the membranous urethra occurs near the apex of the prostate . It is most usually a result of pelvic fracture. There is an associated disruption of the sacroiliac joint so that one half of the pelvis and ischiopubic ramus is pushed up above the other. This applies a traction force on the prostate, which is firmly bound by ligaments to the back of the symphysis pubis. The torn ends of the urethra may be widely displaced by this type of injury.Clinical features
A. SYMPTOMSPatients usually complain of lower abdominal pain and inability to urinate. A history of crushing injury to the pelvis is usually obtained.
B. SIGNS
• Blood at the urethral meatus is the single most important sign of urethral injury. The presence of blood at the external urethral meatus indicates that immediate
urethrography is necessary to establish the diagnosis.
• Suprapubic tenderness and the presence of pelvic fracture are noted on physical examination.
• A large developing pelvic hematoma may be palpated.
• Perineal or suprapubic contusions are often noted.
• Rectal examination may reveal a large pelvic hematoma with the prostate displaced superiorly. Rectal examination can be misleading, however,
Partial disruption of the membranous urethra (currently 10% of cases) is not accompanied by prostatic displacement.
Complications
StrictureUrinary incontinence
Impotence
Orthopedics
Extravasation of urine
Treatment
A. EMERGENCY MEASURES
Shock and hemorrhage should be treated.
B. SURGICAL MEASURES
Urethral catheterization should be avoided.
• Immediate management—Initial management should consist of suprapubic cystostomy to provide urinary drainage.
• Delayed urethral reconstruction—Reconstruction of the urethra after prostatic disruption can be undertaken within 3 months.
• Immediate urethral realignment—Some surgeons prefer to realign the urethra immediately. Persistent bleeding and surrounding hematoma create technical problems.