Gall Bladder
Assist. Prof . Dr Salah aljanaby
General surgeon and laparoscopic surgeon
Babylon medical college
Lecture 3

Ultrasound
■
An ultrasound is the most common test used
for the diagnosis of biliary colic and acute
cholecystitis. It is 90-95% sensitive for
cholecystitis and 78-80% specific. For simple
cholelithiasis, it is 98% sensitive and specific.
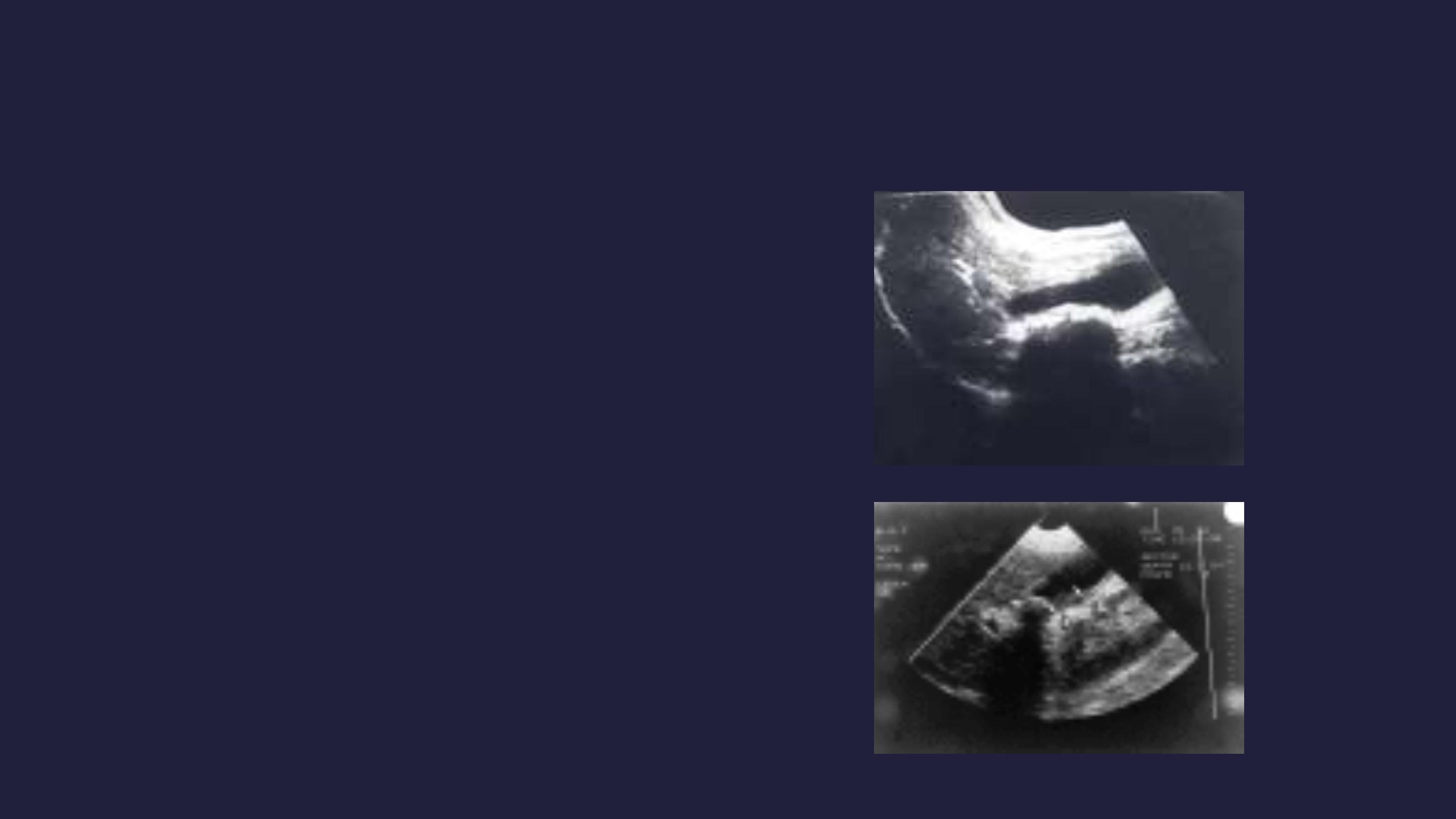
Findings include gallstones or sludge and one
or more of the following conditions
■
Gallbladder wall thickening
(>2-4 mm) -
False-positive wall thickening found in
hypoalbuminemia, ascites, congestive
heart failure, and carcinoma
■
Gallbladder distention
(diameter >4 cm,
length >10 cm)
■
Pericholecystic fluid
from perforation or
exudate
■
Air in the gallbladder wall
(indicating
gangrenous cholecystitis)
■
Sonographic Murphy sign
(86-92%
sensitive, 35% specific), pain when the
probe is pushed directly on the
gallbladder (not related to breathing)

■
Some sonographers recommend the diagnosis of
cholecystitis if both a sonographic Murphy sign and
gallstones (without evidence of other pathology) are
present.
■
Additional findings in the presence or absence of
gallstones: Dilated common bile duct or dilated
intrahepatic ducts of the biliary tree indicate common
bile duct stones. In the absence of stones, a solitary
stone may be lodged in the common bile duct, a
location difficult to visualize sonographically.

■
Advantages of sonography include the following:
■
Images other structures (eg, aorta, pancreas, liver)
■
Identifies complications (eg, perforation, empyema,
abscess)
■
Rapidly performed at the bedside
■
No radiation (important in pregnancy)
■
Disadvantages of sonography include the following:
■
Operator dependent and patient dependent
■
Inability to image the cystic duct
■
Decreased sensitivity for common bile duct stones

■
Biliary scintigraphy (HIDA, diisopropyl iminodiacetic
acid [DISIDA]), nuclear medicine studies
■
Sonography or nuclear medicine testing is the test of
choice for cholecystitis. HIDA scans have sensitivity
(94%) and specificity (65-85%) for acute cholecystitis.
They are sensitive (65%) and specific (6%) for chronic
cholecystitis. Oral cholecystography is not practical for
the ED.
■
HIDA and DISIDA scans are functional studies of the
gallbladder. Technetium-labeled analogues of
iminodiacetic acid (IDA) or diisopropyl IDA-DISIDA are
administered intravenously (IV) and secreted by
hepatocytes into bile, enabling visualization of the liver
and biliary tree.

■
Normal scans are characterized by normal
visualization of gallbladder in 30 minutes.
■
With cystic duct obstruction (cholecystitis), the
HIDA scan shows nonvisualization (ie,
considered positive) of the gallbladder at 60
minutes and uptake in the intestine as the bile is
excreted directly into the duodenum.
■
Obstruction of the common bile duct causes
nonvisualization of the small intestine.
■
The
rim sign
is increased tracer adjacent to the
gallbladder at 60 minutes and suggests
gangrenous cholecystitis.

■
Advantages of HIDA/DISIDA scans include the
following:
■
Assessment of function
■
Normal-appearing gallbladder (by ultrasound); obstructed
cystic duct abnormal on DISIDA scan but not ultrasound.
■
Simultaneous assessment of bile ducts
■
Disadvantages of HIDA/DISIDA scans include the
following:
■
High bilirubin (>4.4 mg/dL) possibly decreases sensitivity
■
Recent eating or fasting for 24 hours also possibly affects
study
■
No imaging of other structures in the area

■
Other Tests:
■
Endoscopic retrograde
cholangiopancreatography (ERCP)
■
ERCP provides both endoscopic and radiographic
visualization of the biliary tract. It can be diagnostic
and therapeutic by direct removal of common bile
duct stones.
■
Magnetic Resonance cholangiopancreatography
(MRCP)

TREATMENT; Conservative treatment
followed by cholecystectomy
Symptoms of acute cholecystitis subside with
conservative treatment in 90 % of cases
■
Four principles
1.
Naso-gastric suction & IV fluid
2.
analgesics
3.
Antibiotics (broad spectrum effective against Gm –
ve aerobes)
4.
Subsequent management ( if inflame. Subside→
oral fluids → fat free diet)

Cholecystectomy on the next available list or after 4-6
wks
■
Conservative treatment is not advised if there is:
1.
Uncertain diagnosis
2.
The possibility of high retrocecal appendix or
3.
Perforated DU cannot be excluded
■
Conservative treatment must be abandoned if pain
and tenderness increased →percutaneous
cholecystostomy → subsequent cholecystectomy

TREATMENT; Routine early operations
Indications:
1.
Within 24 hrs of the onset of the attack
2.
Experienced surgeons
3.
Excellent operating facilities
■
cholecystectomy can be done either by open
or laparoscopic approaches

Acalcuolous cholecystitis
■
Some patients have non-specific inflammation
of the GB , wherease other have one of the
Cholecystoses
■
Diagnosis either by oral cholecystography
( chronic cases) or by isotopic scanning (acute
cases)
■
Cholesterol crystal
in the duod. aspirate may
help diagnosis

Acute acalcuolous cholecystitis is seen more
frequently in:
■
Critical illness
■
Major surgery or severe trauma/burns
■
Sepsis
■
Long-term TPN
■
Prolonged fasting

The Cholecystoses
■
Not uncommon conditions affecting
the GB where there is chronin
inflamm. Changes with hyperplasia
of of all tissue elemnts
Cholesterosis (Strawberry GB)
■
Submucous aggregations of
cholesterol crystals and cholesterol
esters (yellow seeds) in the red
mucosa

Cholesterol polyposis of the GB
■
These are either cholesterol polyposis or
adenomatous changes
Cholecystitis glandularis proliferans (polyp,
adenomyomatosis and intramural diverticuolosis)
■
MM polyps- fleshy and granuolomatous
■
All layer of GB may be thickened
■
Sometimes incomplete septums forms
■
Intraparietal mixed calculi may be present

Diverticuolosis of the GB
■
Usually manifest as black pigment stones impacted in
the out-pouchings of the lacunae of Luschka
Typhoid GB
■
S. Typhi or occasionally S Typhimurium can infect the
GB leading to acute cholecystitis and more commonly
chronic cholecystitis
■
The patient being typhoid carrier excreting the
bacteria in the bils
■
Gall stones may be present

GB cancer
■
Rare ( common in certain area as India where it reaches 9% of
biliary tract disease
■
Found in less than 1% of GB operations
■
In over 90 % of cases gall stones are present
Presentations
■
Age= 70s
■
Sex= female (F-M= 5-1)
Pathology
■
Scirrhous, but may be squamous cell & mixed squamous
adenocarcinoma
■
Spread= direct, lymphatics and veins

Clinical P
■
Either extensive mass in the liver during investigations
for jaundice or
■
At cholecystectomy at the time the histology is
received
Treatment
■
Those diagnosed at cholecystectomy and confined to
the mucosa have a good prognosis (add wide excision
& LN clearance or not ??)
■
Large T reaching serosa= chemoradiotherapy
■
Median survival 1 year
