Induction of labour
Definition :-
Induction of labour is defined as the
artificial initiation of labour , performed when it is considered
that there are benefits to the baby and or mother if the baby is
delivered , compared with the alternative of the baby
remaining in utero .
Current rate of induction of labour are 20 - 22 % .

Indications
1-Abruptio placentae .
2-Chorioamnionitis .
3-fetal demise .
4- Gestational hypertension .
5- Pre-eclampsia and eclampsia .
6- Pre-labour rupture of membranes .
7- post term .
8- Maternal medical conditions .
9- fetal comprise .

Contraindications
Absolute contraindications :--
Contraindication to vaginal delivery such as
1-complete placenta praevia
2-vasa praevia
3- transverse lie .
4-Conditions need immediate delivery such as cord prolapse
5-Previous classical C/S and previous myomectomy entering the
endometrial cavity .

Relative contraindications
Previous C/S ( at increased risk of uterine rupture ).
Success of induction of labor ::--
IOL is most successful when the cervix is ripe at the time of
induction .

●
Ripening :-
is the process by which the cervix changes in
consistency prior to the onset of labour , collagen content
decline and water content increases . The most commonly
used assessment of cervical ripening is the Bishop score .
this score comprises five components of the cervix , all
assessed on vaginal examination . IOL with unripe cervix
will require more uterine activity to effect cervical
dilatation , potentially causing , a longer labour , more pain
and stress for both mother and baby , higher risk of uterine
rupture and increase incidence of instrumental delivery and
C/S .
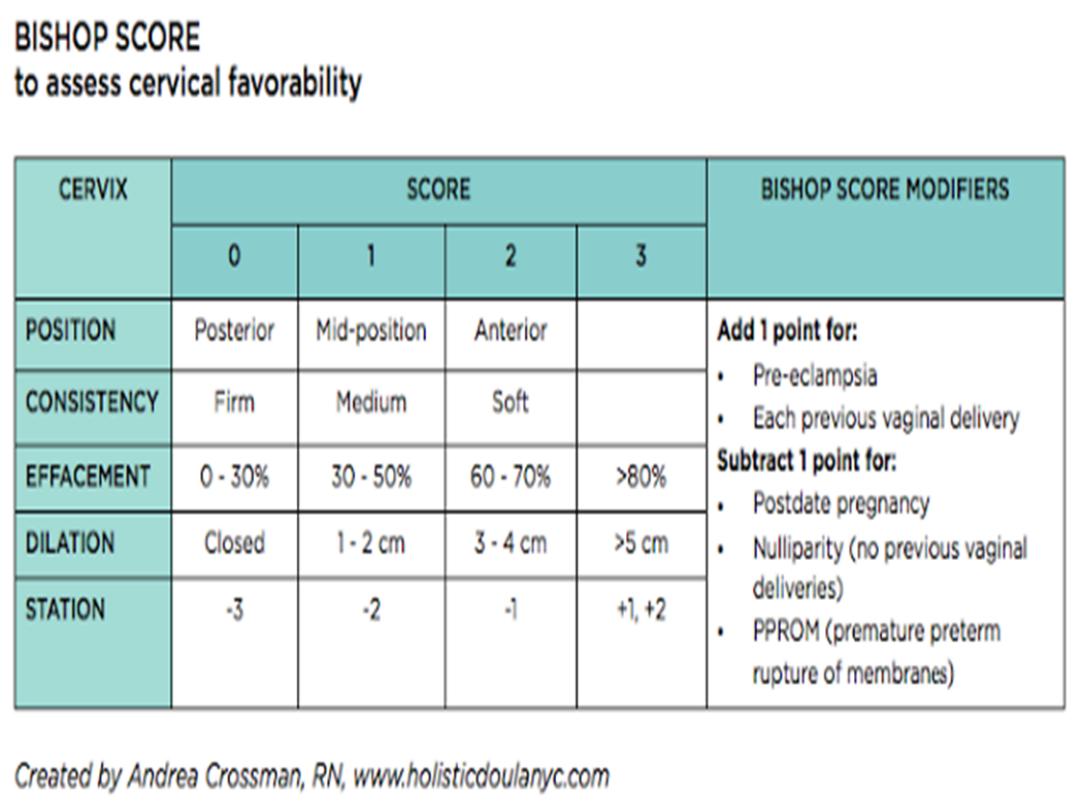

Note :---
Bishop score of 8 and above mean high success
rate of induction while low score mean unfavourable cervix
and high failure rate of induction .
Pharmacological method
1-intravaginal prostaglandin (PG E2, dinoprostone)
2- intravaginal prostaglandin (PG E1, misoprostol )
Mechanical method :--
( increase maternal infection )
1-intrauterine administration of Foley catheter followed by extra
amniotic saline .
2- laminaria .
3-Membrane sweeping .
Once the cervix is ripe , continuation of labor induction may involve
fore water amniotomy ( artificial rupture of membrane ) with or without
augmentation of labor with Syntocinon .

Augmentation of labor :-
is the process of speeding up the first
stage of labor .Amniotomy with or without oxytocin has been the
standard intervention .
Complications
1--Failure of procedure , 15% in primigravida with unfavourable
cervix but less commonly with multigravida and primi with
favourable cervix and high Bishop score at the start of induction .
2--Caesarean section and operative delivery .

3-Hyperstimulation :- uterine hyperstimulation is defined as a
contraction frequency of more than five in 10 min. or contraction
exceeding 2 min. duration .
4-Tachysystol : occur when uterine hyperstimulation is
accompanied by abnormal FHR patter n , which manage by
Putting the patient in left lateral position , O2 mask ,
rehydration , and if FHR not improve finally we can give the
patient tocolytic agent such as Teributalin .
Monitoring
Monitoring of maternal and fetal wellbeing during
induction of labor is sparse . cardiotocograph should be
performed to confirm that the FHR is normal prior to PG
insertion .The CTG should repeated when contraction begin
, normally 2-6 hr after PG administration .