
Abnormalities of third stage of
labour
Post partum hemorrhage:
Postpartum hemorrhage (PPH) is excessive bleeding after
delivery of the fetus and may occur before or after delivery
of the placenta, Postpartum hemorrhage (PPH) is
traditionally defined as
the loss of more than 500
milliliters of blood following vaginal delivery or
more than 1000 milliliters following cesarean
delivery.
PPH is considered severe when blood loss exceeds 1000
milliliters after vaginal delivery or results in signs or
symptoms of hemodynamic instability,
Postpartum hemorrhage can be classified as
primary
,
which occurs within 24 hours of delivery, or
secondary
,
which occurs 24 hours to 12 weeks postpartum. Primary
PPH is more common than secondary PPH
Potential
sequel
of PPH include orthostatic hypotension,
anemia and fatigue which can make breastfeeding and
maternal care of the newborn more difficult. Postpartum
hemorrhage may increase the risk of postpartum depression
and acute stress reactions. Transfusion may be necessary and
carries associated risks including infection and transfusion
reaction. In the most severe cases, dilutional coagulopathy
should be anticipated. Hemorrhagic shock may lead to
Sheehan’s Syndrome (posterior pituitary ischemia with delay or
failure of lactation), occult myocardial ischemia, or death.

Risk Factors for Postpartum Hemorrhage:
Antepartum Risk Factors
History of PPH
• Nulliparity
• Grand multiparity (> five deliveries)
• Coagulopathy (congenital or acquired including use of
medications such as aspirin or heparin)
• Abnormal placentation
• Age > 30 years
• Anemia
• Overdistension of the uterus
Labor Risk Factors
Prolonged labor (first, second, and/or third stage)
• Preeclampsia and related disorders
• Fetal demise
• Induction or augmentation
• Use of magnesium sulfate
• Chorioamnionitis
Surgical Interventions
Operative vaginal delivery •
Cesarean section ,
episiotomy
Mnemonic for the Specific Causes of PPH
Tone Atonic uterus 70 percent
Trauma Lacerations, hematomas, inversion,
rupture
Tissue Retained tissue or membranes, invasive
placenta 10 percent
Thrombin Coagulopathies 1 percent
Diagnoses and management
Pregnant women have increased plasma volume and red blood
cell mass. In addition, they are typically healthy and can
accommodate mild to moderate blood loss without having signs
or symptoms such as orthostasis, hypotension, tachycardia,
nausea pallor, slow cap refilling, dyspnea, oliguria, or chest pain
.Appreciation of risk factors,accurate estimation of blood loss
and recognition of women developing symptoms of
cardiovascular compromise are imp steps in mgx. Once excessive
blood loss is suspected, treatment must be initiated quickly by
progressing through the Four T’s mnemonic (Tone, Trauma,
Tissue, and Thrombin).
Management
Summon help from senior obstetrician , anesthetist, 2
midwives haematologist blood bank
Resuscitation
Two large bore IVs bladder catheter
Oxygen by mask
Fluid Resuscitation intravenously, fluid balance chart
central venus pressure and arterial lines
Monitor BP, HR, urine output CBC clotting factors LFT
, RFT, type and cross match at least 6 units of blood
Transfuse blood as soon as possible ,may need cryo
FFP plateletes
. Since uterine atony is the most common cause , the uterus
should be massaged and oxytocics given 40 IU in 500 ml saline
over 4 hours. Bimanual uterine compression and more potent
drugs can also be used like ergometrine 0.5 mg i.m misopristol
800 micrograms rectally ,cyclocaprone should be given in the
first 3 hours. A vaginal exam should be done to expel clots of
uterus which prevent its contraction ,the placenta should be
delivered if retained and inspected for missing cotyledons, and
assess genital tract trauma. Any tear should be repaired .if
bleeding continues referral to theater is indicated for further
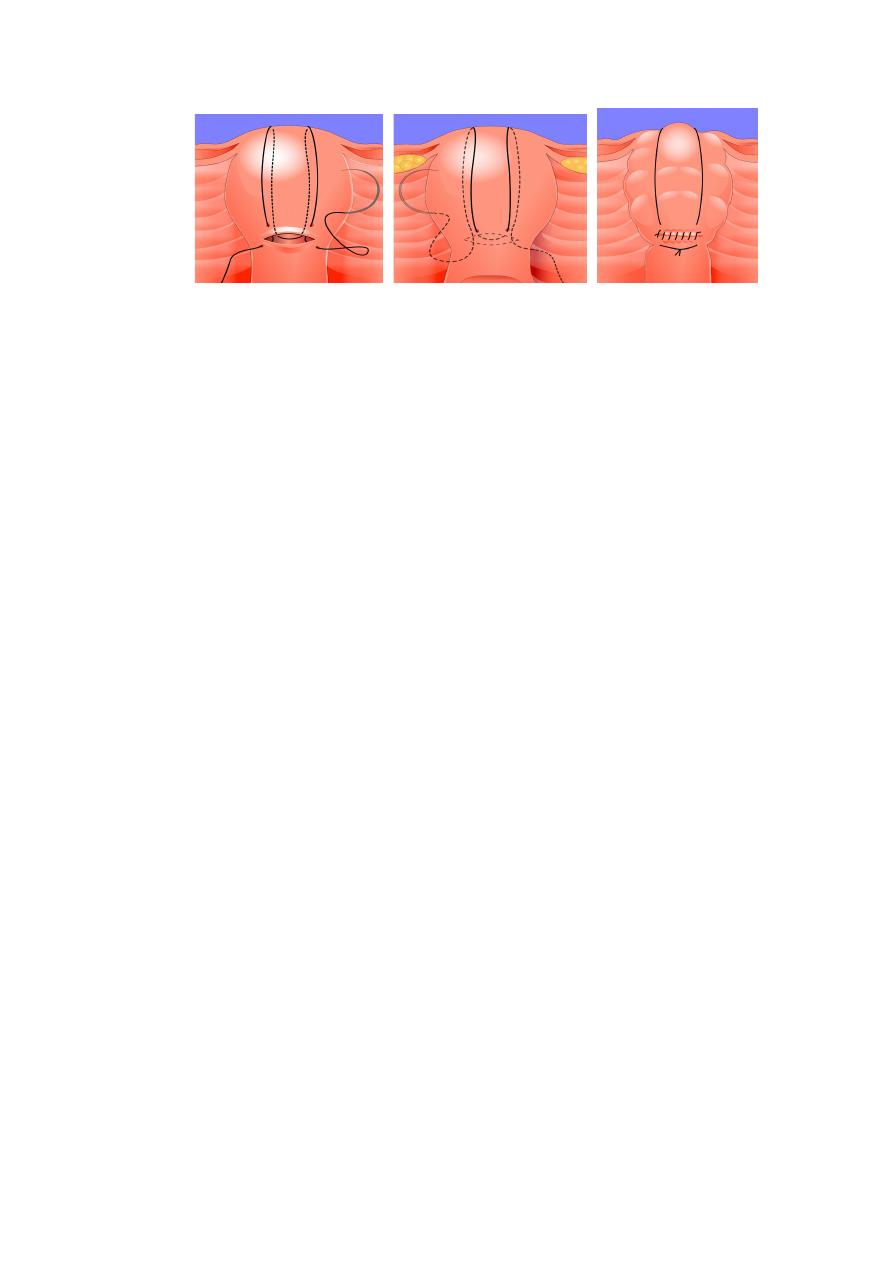
exam under anasthesea. Under GA we can do uterine
tamponade with balloons ,radiological occlusion of uterine
vessels, laparotomy for bilateral iliac artery ligation uterine
compression sutures(B-lynch), and finally hysterectomy.
Massive PPH require correction of clotting factors using FFP
platelets and cryo precipitate.
Secondary PPH is a rare cause and it is due to retained products
of conception and \or uterine infection.
TRAUMA
Lacerations and hematomas resulting from birth trauma
can cause significant blood loss that can be lessened by
hemostasis and timely repair. Sutures for hemostasis are
placed if direct pressure does not stop the bleeding,and
should be placed well above the apex of lacerations.
Cervical lacerations
should not be sutured unless
actively bleed.
Vaginal lacerations
require good light and good
exposure with running locked sutures.
Uterine rupture
requiring laparotomy for repair or
subtotal hysterectomy.
TISSUE
Retained
tissue
(placenta,
placental
fragments,
membranes,and blood clots) prevents the uterus from
contracting enough to achieve optimal tone.
Retained Placenta
. The mean time from delivery until placental expulsion is
eight to nine minutes. A longer interval is associated with
an increased risk of PPH. Retained placenta, defined as the
failure of the placenta to deliver within 30 minutes after birth
(and after one hr in the absence of AMTL).
Active management of the third stage
should be recommended to all women because high quality
evidence shows that it reduces the incidence of postpartum
haemorrhage from 15 to 5 per cent.
AMSTL started with the delivery of anterior shoulder by
injection of oxytocin intramuscular. After delivery of the
baby and when the signs of placental separation are
recognized, controlled cord traction is used to expedite
delivery of the placenta. When a contraction is felt, the left
hand should be moved suprapubically and the fundus
elevated with the palm facing towards the mother. At the
same time, the right hand should grasp the cord and exert
steady traction so that the placenta separates and is
delivered gently, care being taken to peel off all the
membranes, usually with a twisting motion.
In approximately 2 per cent of cases, the placenta will not
be expelled by this method. If no bleeding occurs, a further
attempt at controlled cord traction should be made after 10
minutes. If this fails, the placenta is
‘retained’ and will
require manual removal under general or regional
anaesthesia in the operating theatre. Direct injection of
oxytocin into the umbilical vein may bring about delivery of
the placenta while preparations are being made for theatre.
Physiological management of the third stage is
where the placenta is delivered by maternal effort, and
no uterotonic drugs are given to assist this process. It is
associated with heavier bleeding . In the event of
haemorrhage or if the placenta does not
deliver after 30
minutes, manual removal of the placenta should be considered
Invasive placenta can be life threatening
risk factors include prior C\S, prior invasive placenta, placenta
previa (especially in combination with prior cesarean sections,
increasing to 67 percent with placenta previa and four or more
prior cesareans), advanced maternal age, and high parity
Classification is based on the depth of invasion. Placenta
accreta
adheres to the myometrium, placenta
increta
invades
the myometrium, and placenta
percreta
penetrates the
myometrium to or beyond the serosa. The usual treatment for
invasive placenta is hysterectomy
THROMBIN
Coagulation disorders, a rare cause of PPH, are unlikely to
respond to the uterine massage, uterotonics, and repair of
lacerations. Coagulation defects may be the cause and/or
the result of a hemorrhage and should be suspected in
those patients who have not responded to the usual

measures to treat PPH, are not forming blood clots, or are
oozing from puncture sites.
Many patients taking medications such as heparin or
aspirin or who have chronic coagulopathies such as
idiopathic
thrombocytopenic
purpura,
thrombotic
thrombocytopenic purpura, von Willebrand’s disease, and
hemophilia are identified prior to delivery, allowing
advanced planning to prevent PPH. Coagulopathic
bleeding before or during labor can be the result of HELLP
syndrome (Hemolys Elevated Liver enzymes and Low
Platelets) or disseminated intravascular coagulation (DIC).
Obstetric conditions that can cause DIC include severe
preeclampsia, amniotic fluid embolism, sepsis, placental
abruption (often associated with cocaine use or
hypertensive disorders), massive PPH and prolonged
retention of fetal demise.
Evaluation should include a platelet count, prothrombin time
(INR), partial thromboplastin time, fibrinogen level, and fibrin
split products (d-dimer). If rapid laboratory testing is not
available, an empty whole blood tube (“red top”) can be filled
with maternal blood and taped to the wall. It should form a clot
within five to 10 minutes. Management of coagulopathy consists
of treating the underlying disease process, serially evaluating the
coagulation status, replacing appropriate blood components.
OBSTETRICAL SHOCK

Hypotension without significant external bleeding may
result from concealed hemorrhage uterine inversion and
amniotic fluid embolism.
An improperly sutured episiotomy can lead to
concealed
PPH
.A soft tissue haematoma usually of the vulva can
lead to occult blood loss without any evidence of
laceration or episiotomy.
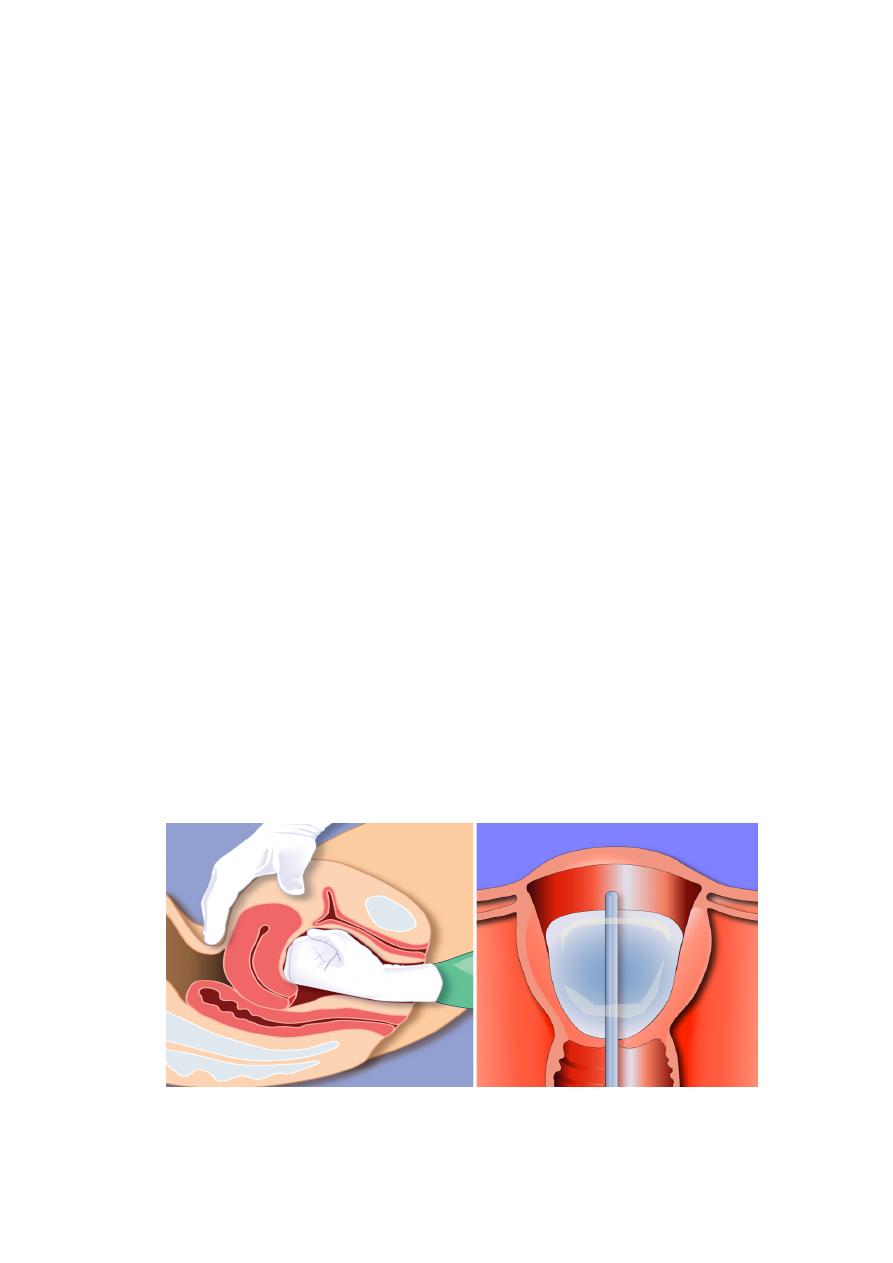
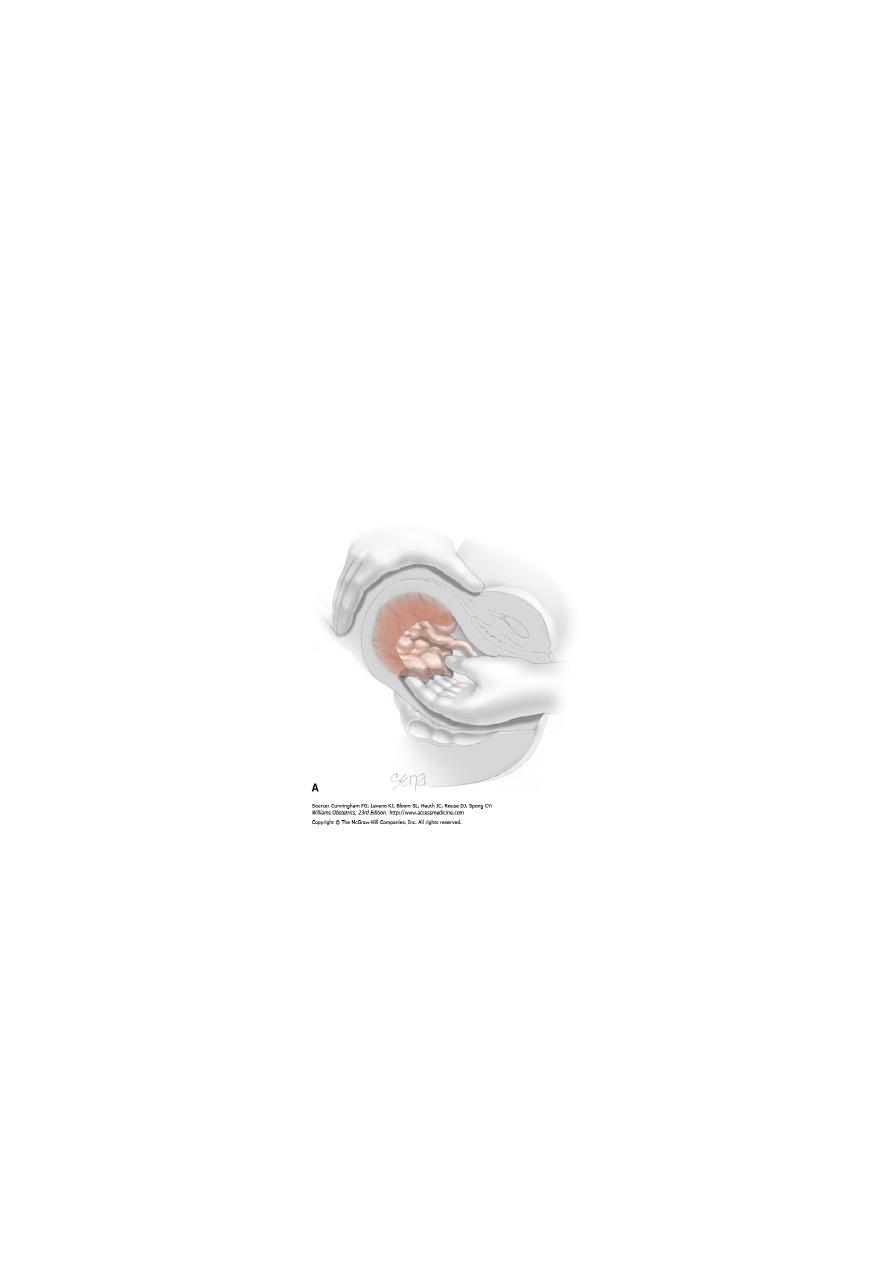
Uterine Inversion
• It is turning inside out of the uterus .Fundal, adherent,
or invasive implantation of the placenta may lead to
inversion. The patient may show signs of shock
(pallor, hypotension) without excess blood loss.
Upon inspection, the inverted uterus may be in the
vaginal vault or may protrude from the vagina,
appearing as a bluish-gray mass that may not be
readily identifiable as an inverted uterus
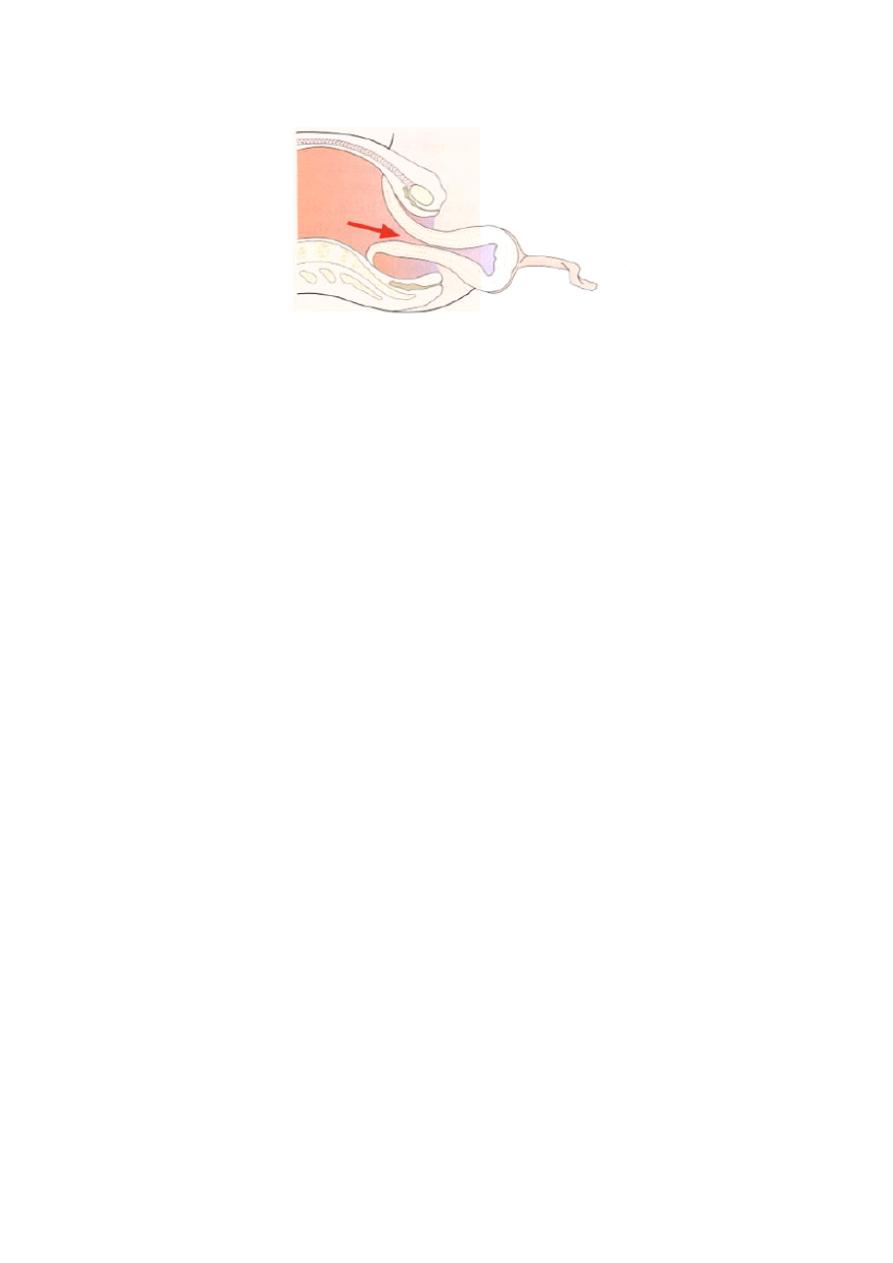
• If the placenta is still attached ,it should be left in place
until after reduction to limit hemorrhage. If oxytocin is
running, it should be stopped, and an attempt
should be made to replace the uterus. If initial
attempts to replace the uterus have failed ,general
anesthesia may allow sufficient uterine relaxation for
manipulation. Rarely surgery is required. Once
replacement is successful an oxytocin infusion should
be started before intrauterine hand is removed.
Amniotic fluid embolism
It is a rare condition charecterised by fulminating
consumption coagulopathy, bronchospasm and vasomotor
collapse.it is fatal in 80% of cases.
It is triggered by an intravascular infusion of significant
amount of amniotic fluid during a rapid labour in the
presence of ruptured membranes.the thromboplastin in the
amniotic fluid may trigger a consumption coagulopathy .
The treatment include immediate CPR with mechanical
ventilation ,correct the shock with electrolyte solution and
packed RBC transfusion ,and reversal of coagulopathy with
platelets and fibrinogene.