NORMAL LABOUR
Introduction, maternal and fetal anatomy
By reference textbook
Suhaila Al-Shaikh Obstetrics by ten teachers
20
th
ed (2017)
Learning objectives
1.
The student should know the types of female
pelvis.
2.
understand the importance of the dimensions of
the bony pelvis of the pregnant woman in
determining the progress of labour and the mode
of delivery.
3.
How to assess pelvic dimensions.
4.
Know the dimensions of the fetal skull.
5.
Understand how the attitude of the fetal head
affects these dimensions.
labour
Labour or human parturition is the
physiological process
that results in
birth of a baby, delivery of the placenta
and the signal for lactation to begin.
POWER
PASSAGES
PASSENGER
The 3 Ps ??
Labour
Health professionals who manage labour should understand that:
The first important step is to recognize when labour has
started
.
Labour is then divided into three stages:
the
first stage
begins with diagnosis of the onset of labour and is
complete when full cervical dilatation ?? (how many cm )has been
reached;
the
second stage
begins with full cervical dilatation and ends with
birth of the baby;
and the
third stage
begins with birth of the baby and ends with
complete delivery of the placenta and membranes.
Complications
can
occur during any of the three stages
and can
be divided into maternal and fetal-neonatal complications.

• Labour
can be defined as the
process by which regular painful
contractions bring about
effacement and dilatation of the
cervix and descent of the
presenting part, leading to
expulsion of the fetus and the
placenta from the mother.

A doctor or midwife who manages
labour must be aware of the normal
anatomy and physiology of the
mother and fetus, what
distinguishes an abnormal from a
normal labour, and when it is
appropriate to intervene
Anatomy
Maternal bony pelvis
and fetal head
Bony pelvis
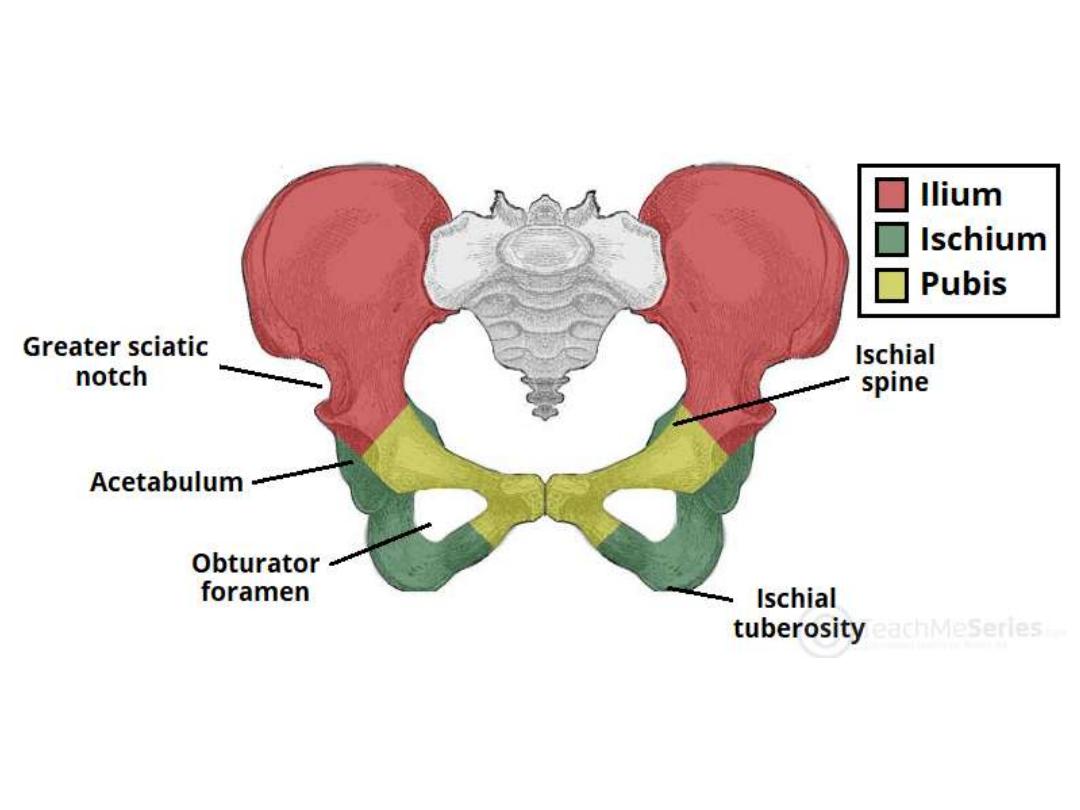
• The bony pelvis is made of 4
bones: the
sacrum, coccyx, and
2 innominate bones which are
(composed of the ilium,
ischium, and pubis).
These are
held together by the SIJ, SP, and
the SCJ joints.
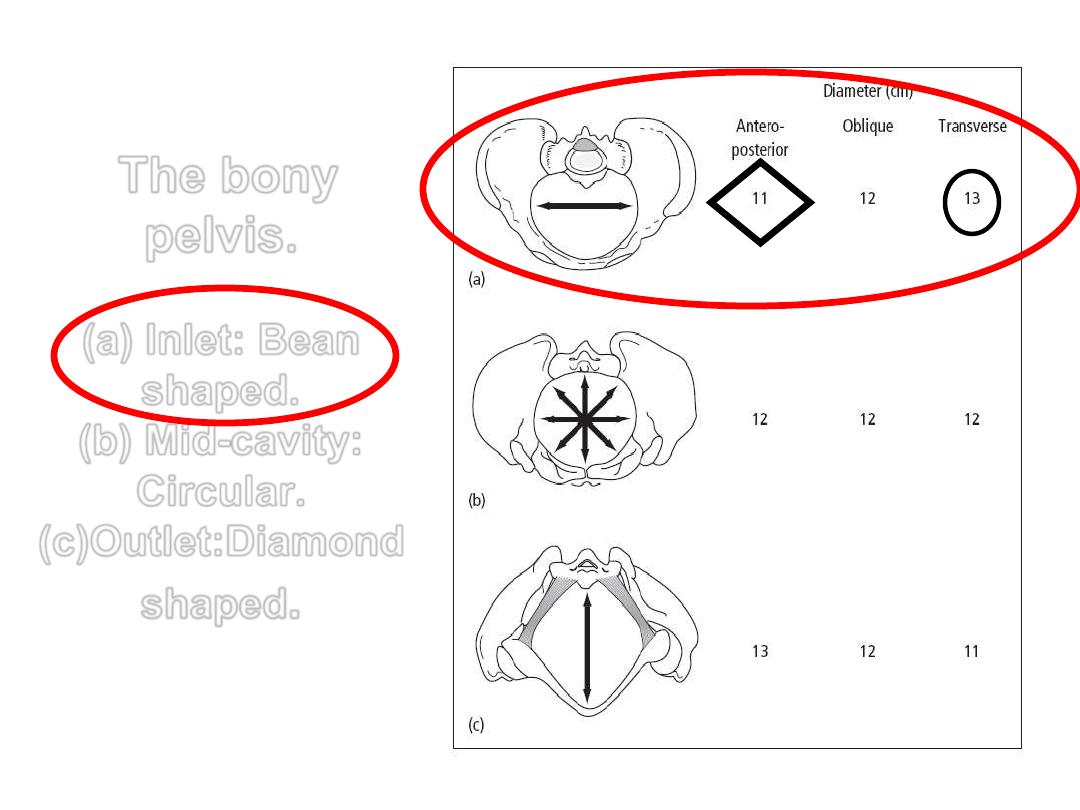
The bony
pelvis.
(a) Inlet: Bean
shaped.
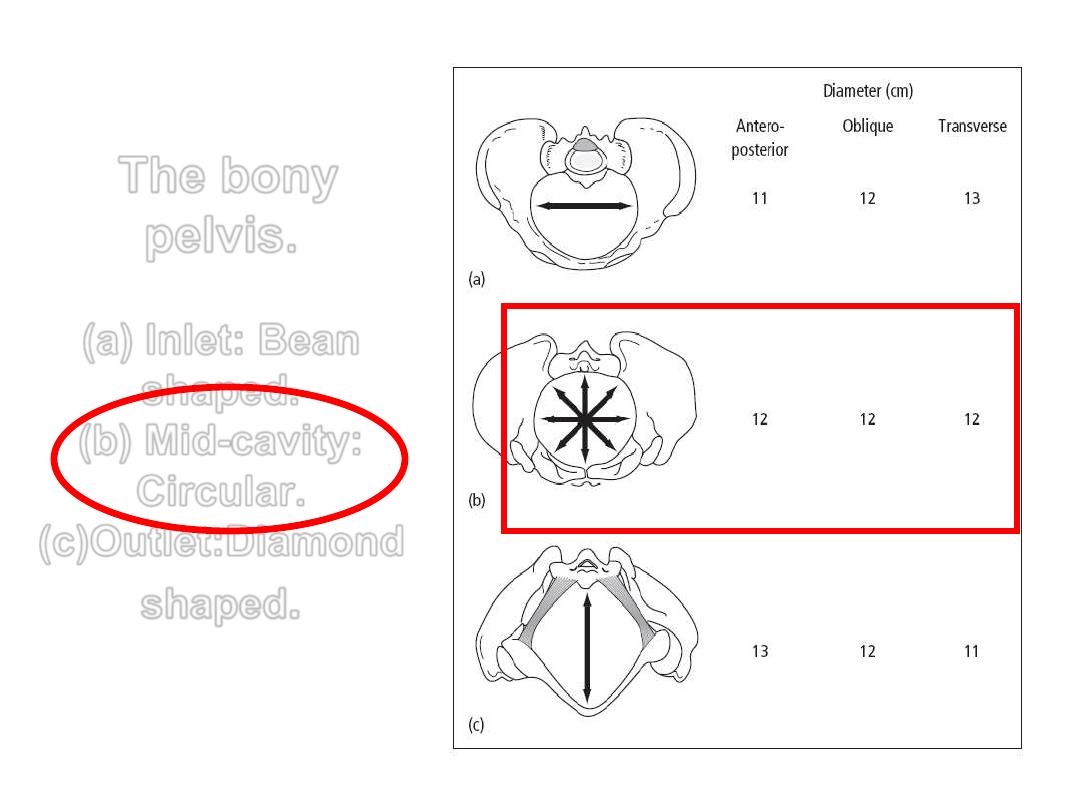
(b) Mid-cavity:
Circular.
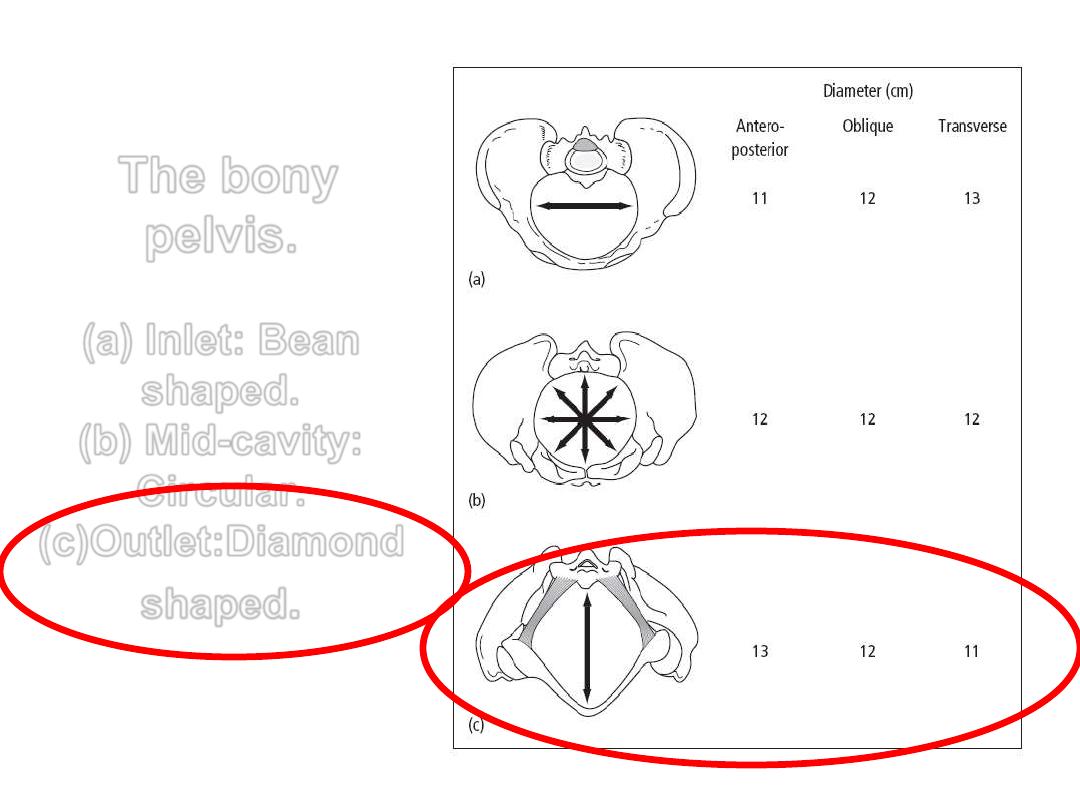
(c)Outlet:Diamond
shaped
.
The bony
pelvis.
(a) Inlet: Bean
shaped.
(b) Mid-cavity:
Circular.
(c)Outlet:Diamond
shaped
.
The bony
pelvis.
(a) Inlet: Bean
shaped.
(b) Mid-cavity:
Circular.
(c)Outlet:Diamond
shaped
.
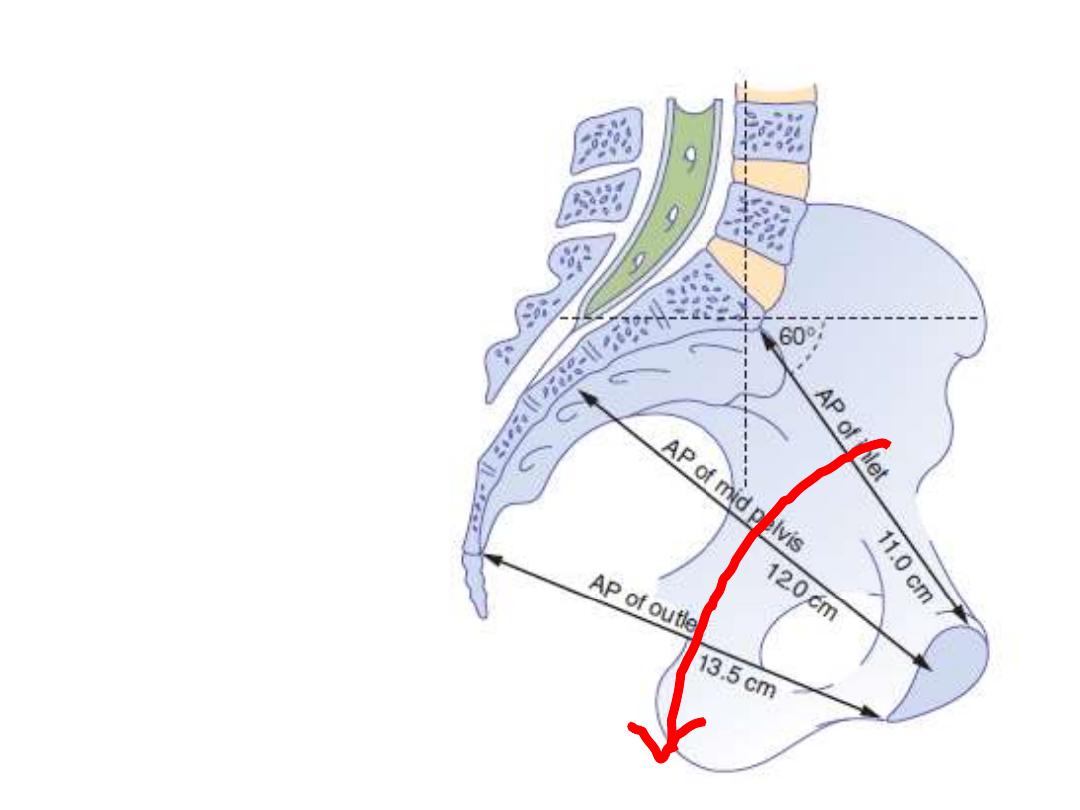
The
pelvic axis
describes
imaginary
curved line,
a path that
the centre
of the fetal
head must
take during
its passage
through the
pelvis
The pelvic brim or inlet
The pelvic mid-cavity
The pelvic mid-cavity can be described as an area
bounded in
front
by the middle of the symphysis
pubis,
on each side
by the pubic bone, the obturator
fascia and the inner aspect of the ischial bone
and spines,
and
posteriorly
by the junction of the second and
third sections of the sacrum.
The pelvic cavity is almost rounded
T- diam. = 12 cm
A-P diam. = 12 cm.
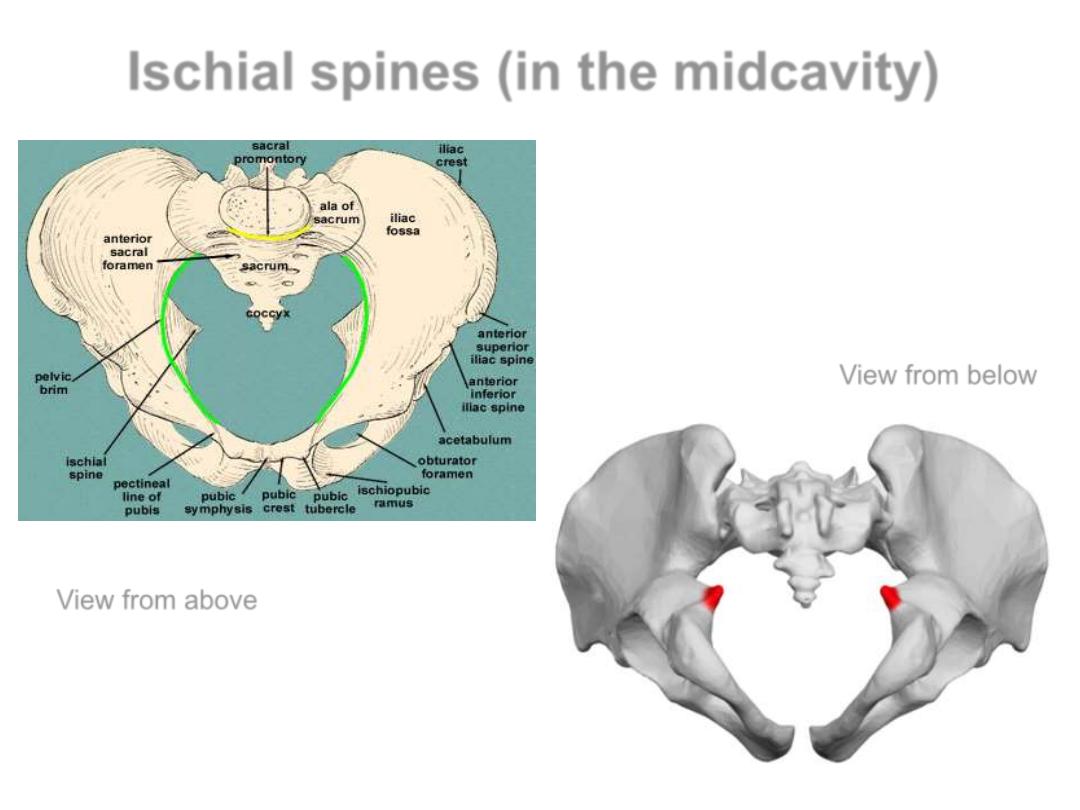
Ischial spines (in the midcavity)
View from below
View from above

The ischial spines are palpated vaginally
and are used as landmarks to:
1. assess the descent of the head on vaginal
examination (station of the presenting
part).
2. providing an anaesthetic block to the
pudendal nerve which is needed for
instrumental delivery.
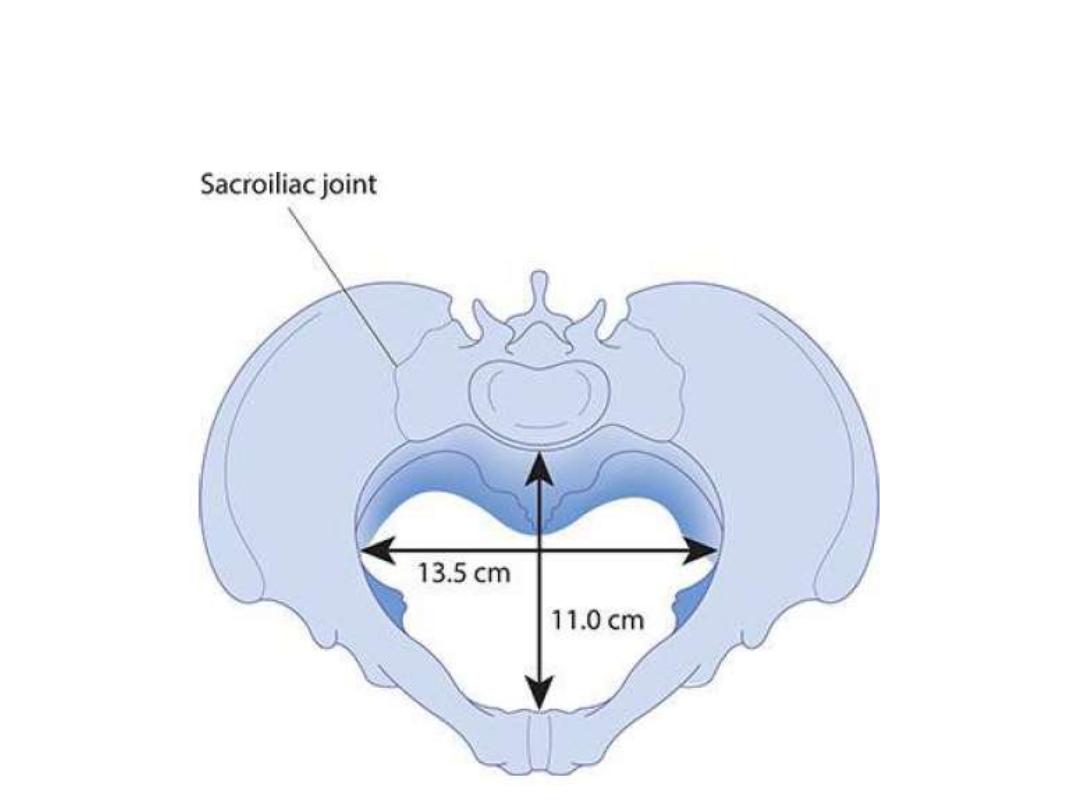
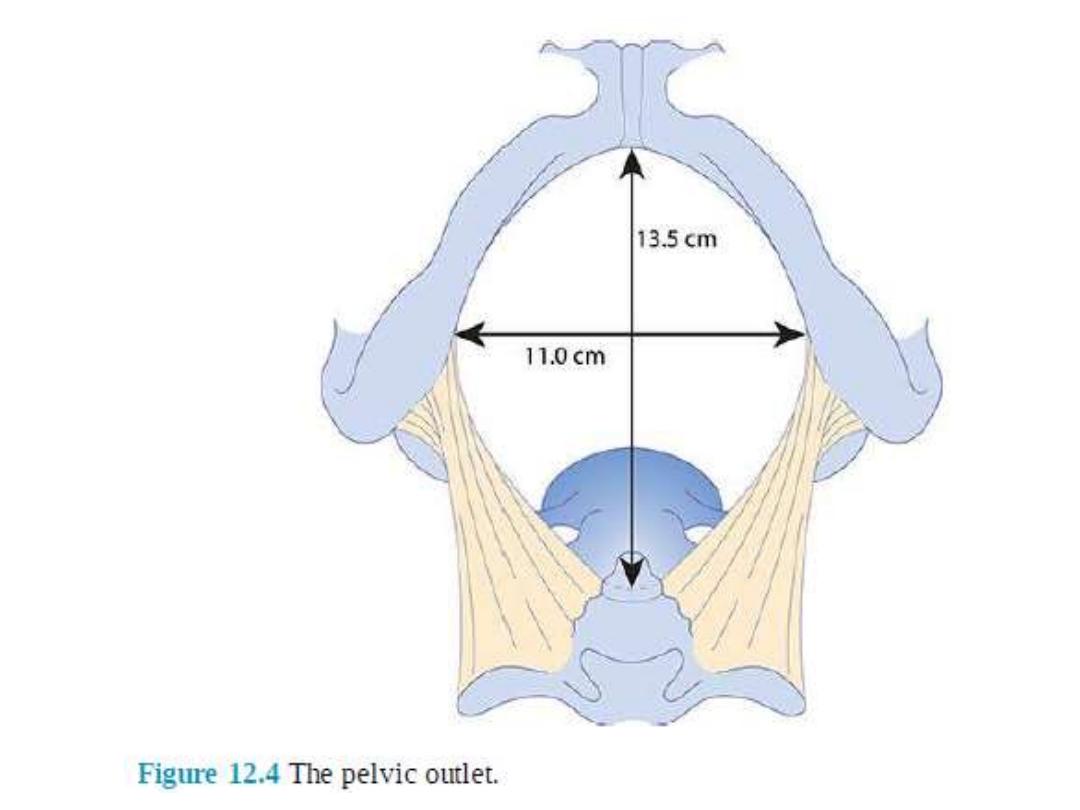
The pelvic outlet
The pelvic outlet is bounded
in
front
by the lower margin of the
symphysis pubis,
on each side
by the descending ramus of
the pubic bone, the ischial tuberosity and
the sacrotuberous ligament,
and
posteriorly
by the last piece of the
sacrum.
The AP diameter of the pelvic outlet is
13.5 cm and the transverse diameter is 11
cm

• Pelvic shape or type
• Maternal stature & ethnicity
• Previous pelvic fractures and metabolic bone disease,
such as rickets
• And as the loosening of pelvic ligaments towards the
end of the third trimester by relaxin, the pelvis
becomes more flexible and these diameters may
increase during labour.
• Some favourable maternal positions in labour (e.g.
squatting or kneeling).
Factors affecting pelvic dimentions
1. the
obstetric conjugate
of the pelvic
inlet ( A-P dimension) : 11 cm
2. the
bispinous diameter
(cavity width):
10.5 cm in the midcavity.
3. the
bituberous diameter
11 cm (the
pelvic outlet width)
4. the
the sacral concavity
and its length
5. the
subpubic angle (arch)
Pelvic diameters: These represent the space
available for the fetal head when it passes
through the pelvis during labour
Pelvic shapes (types)
We have 4 types or shapes of the
bony pelvis and these are:
gynecoid
android
anthropoid
platypelloid.
And their associated obstetric
outcomes
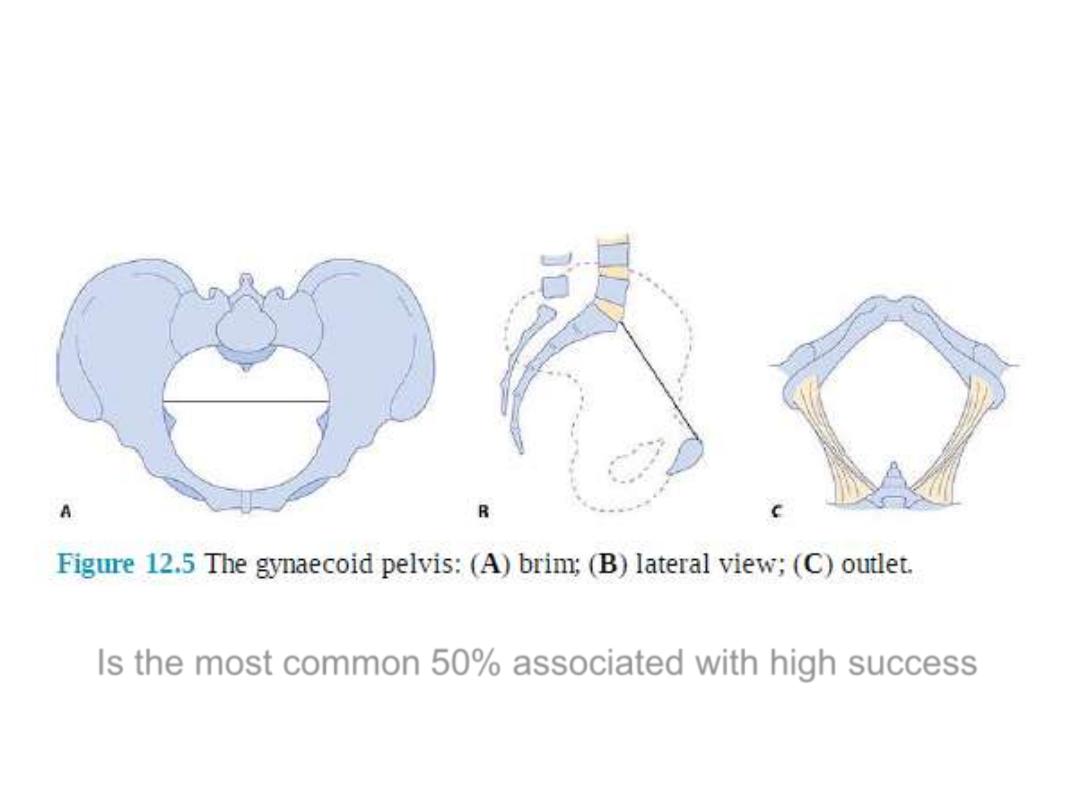
Gynecoid pelvis
Is the most common 50% associated with high success
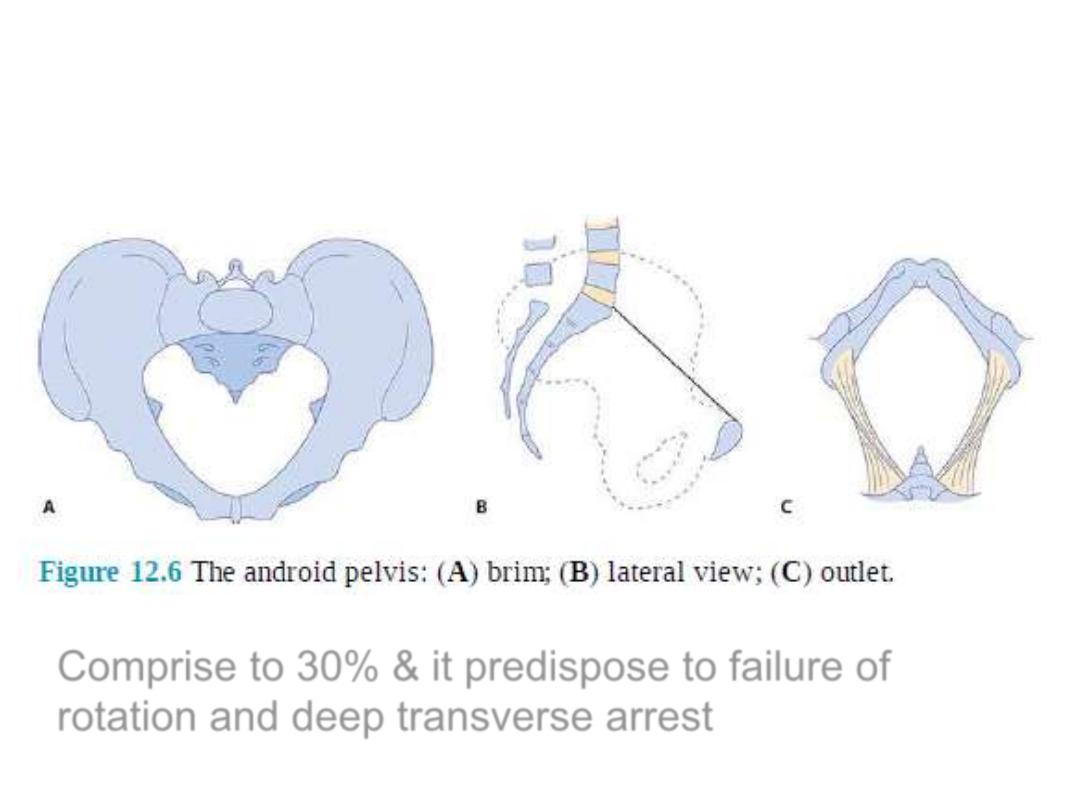
Android pelvis
Comprise to 30% & it predispose to failure of
rotation and deep transverse arrest
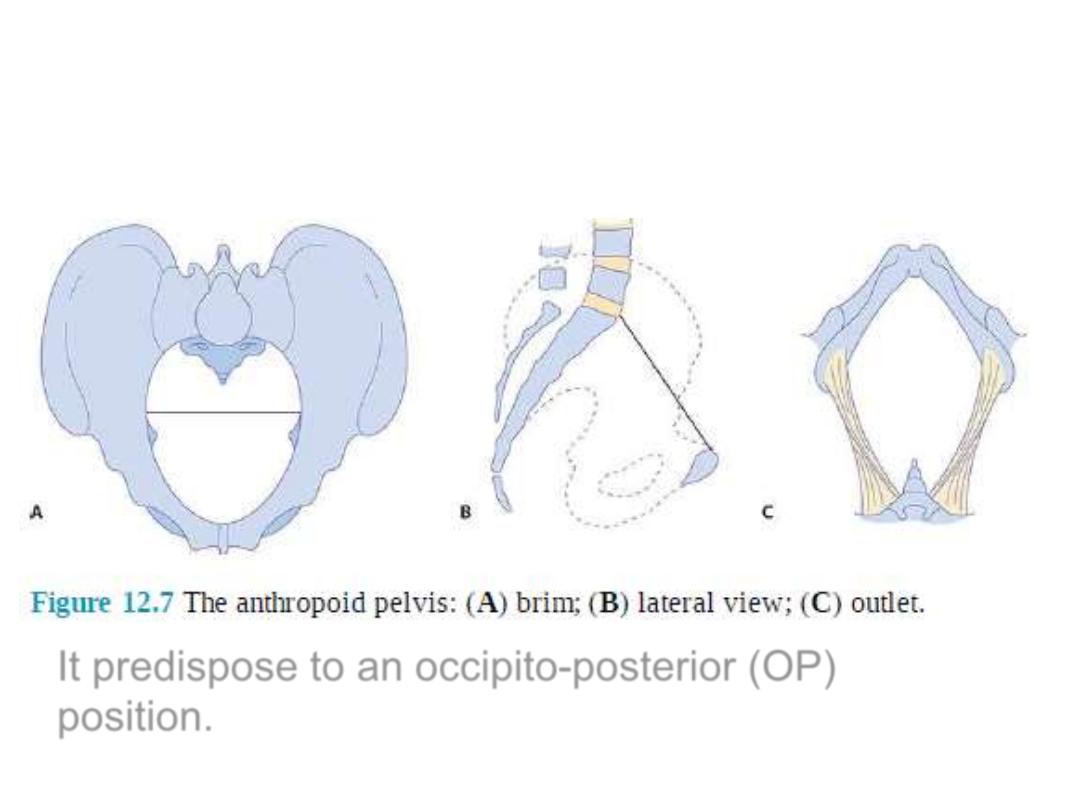
anthropoid pelvis
It predispose to an occipito-posterior (OP)
position.

Platypelloid pelvis
is associated with an increased risk of obstructed labour
due to failure of the head to engage, rotate or descend
.
The perineum
The final obstacle against the desent of
the fetus during labour is the
perineum. It may be involved in a
second-degree perineal tear and an
episiotomy in primiparous women .
While in multiparous it may remain
intact during vaginal delivery

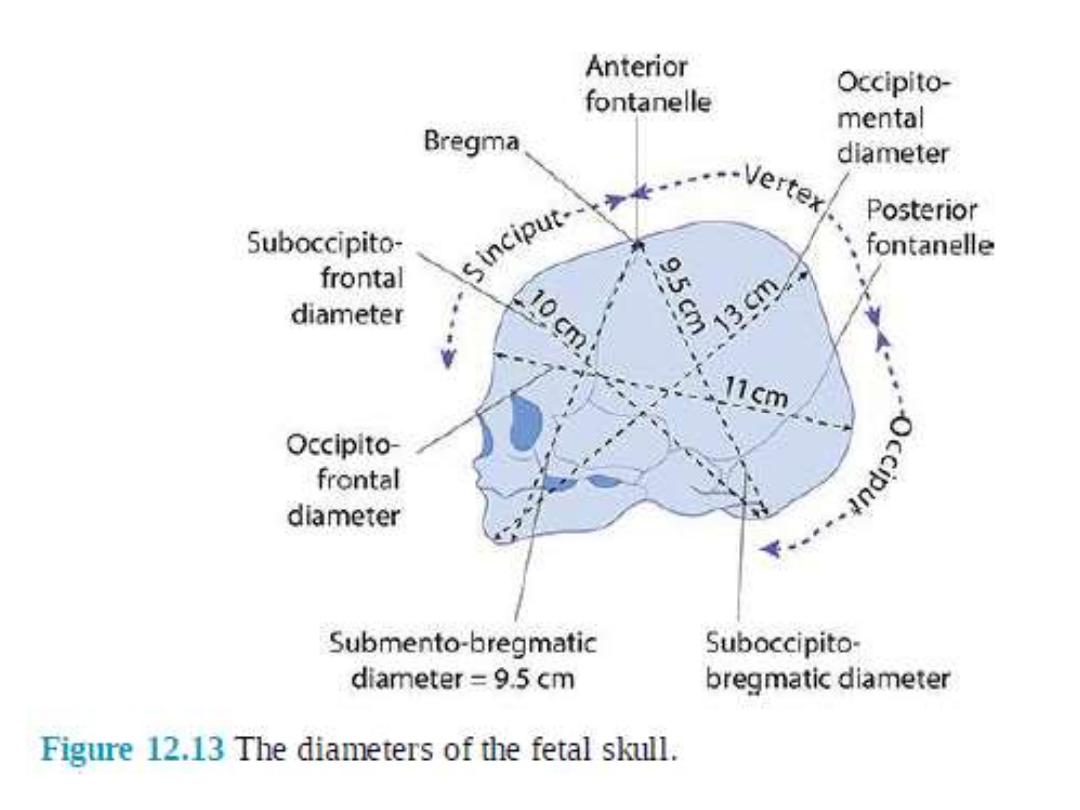
Dimensions of the fetal skull
• The fetal head is the largest and
the least compressible part of the
fetus
• The fetal skull consists of a base
and a vault (cranium) which
consists of the occipital, parietal,
frontal and temporal bones
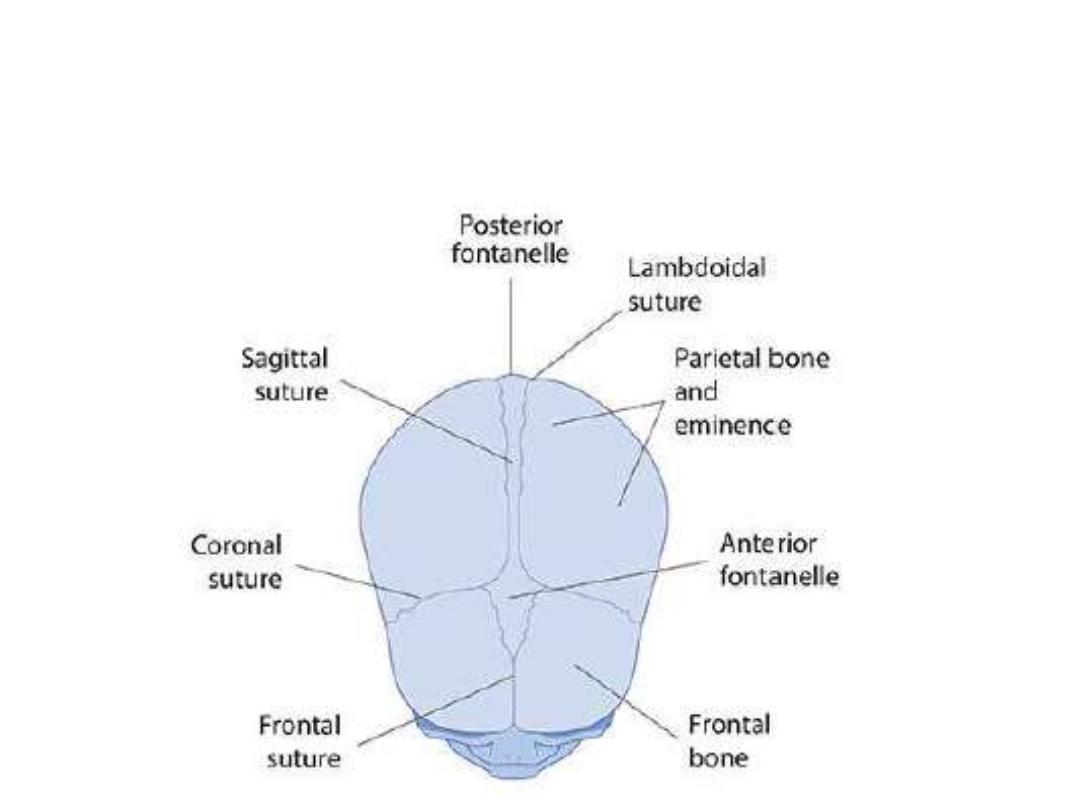
The fetal skull from the superior
view
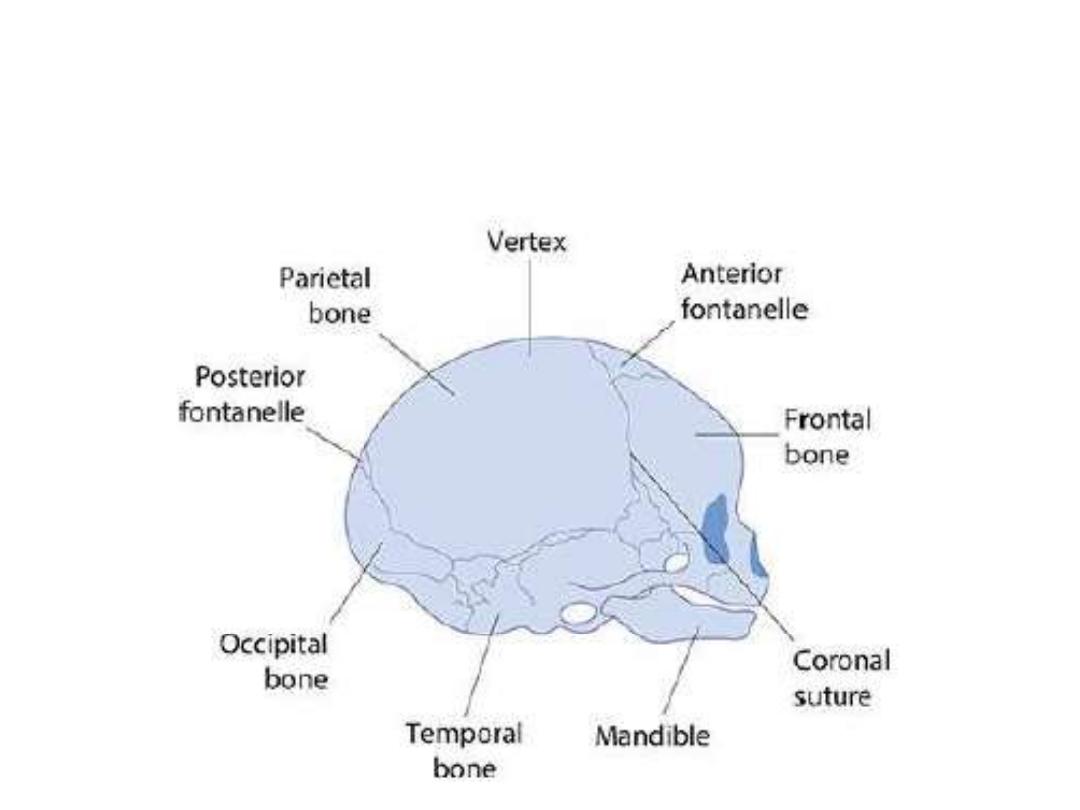
The fetal skull from the lateral
view

these are easily compressible
and interconnected by
membranes and these features
allow molding to occur which
means the overlap of these
bones under pressure and
changing their shape to
conform to maternal pelvis
during vaginal delivery
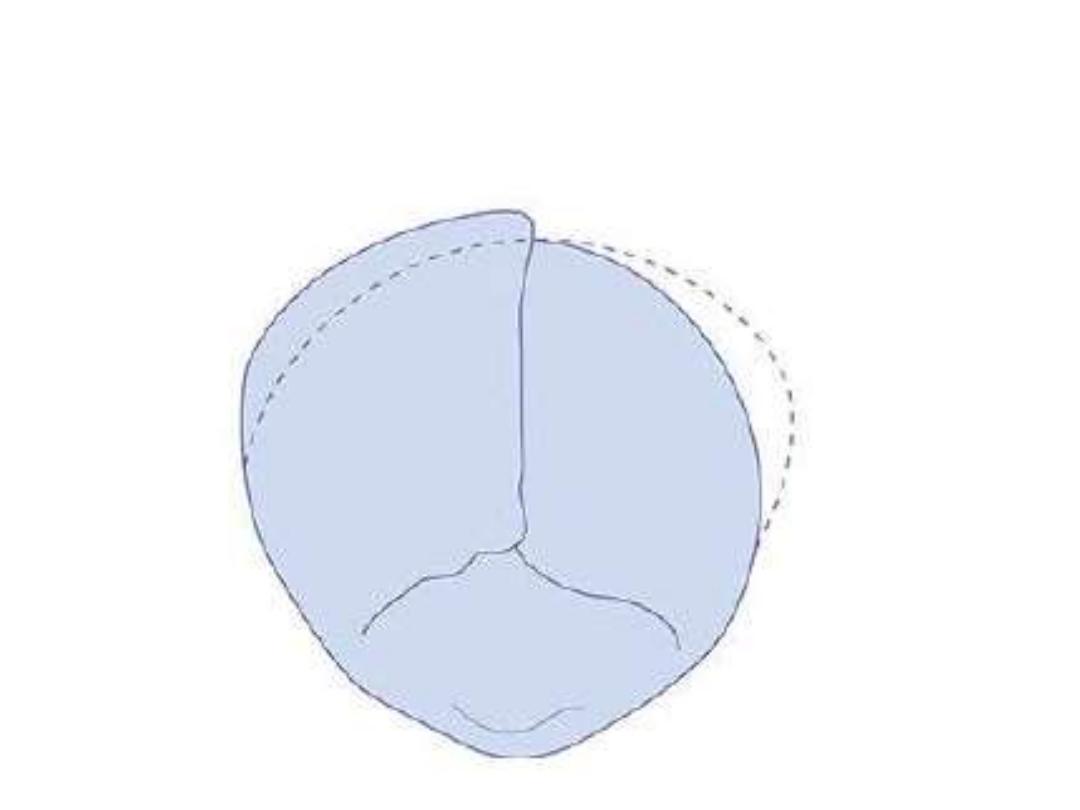
moulding of the fetal skull
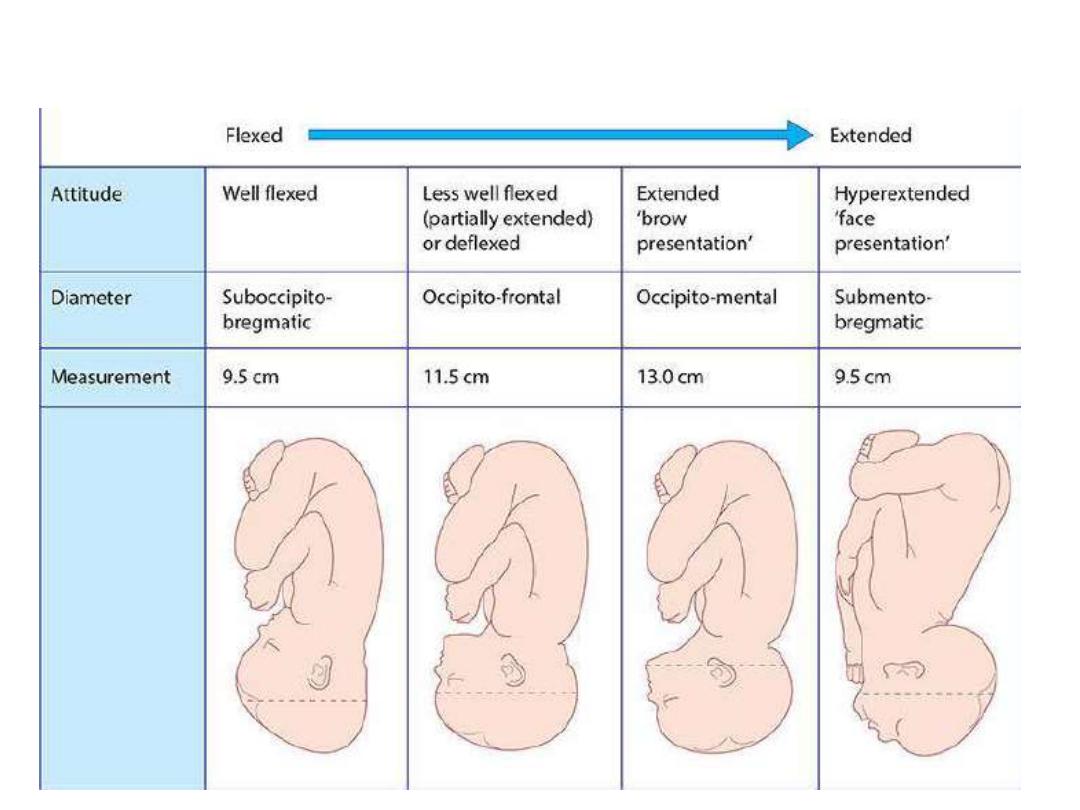
The effect of fetal attitude on the presenting diameter