3
rd
stage of labour:
Signs of placental separation
A fresh show of blood from vagina,
The umbilical cord lengthens outside the
vagina,
The fundus of the uterus rises up,
The uterus becomes firm and globular.
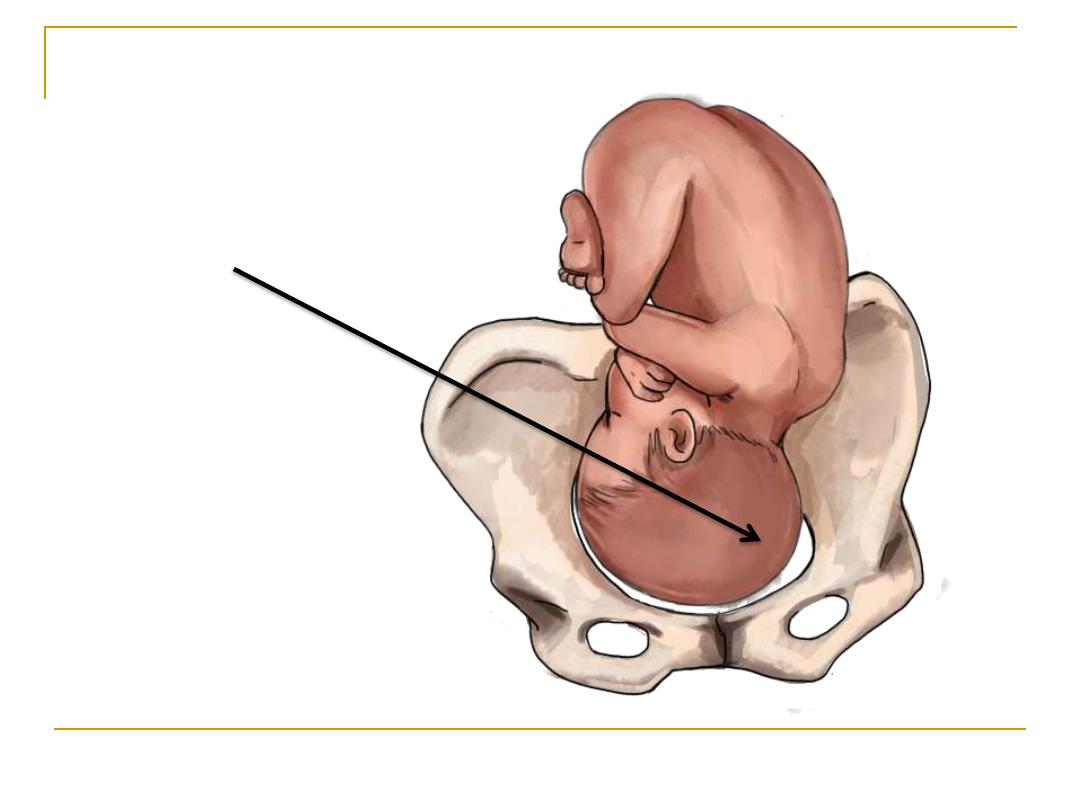
Engagement?
Position?
Atitude?
Station?
Moulding?
Important terms in obstetrics
LOT
right
left
Left Occipito-Transverse position
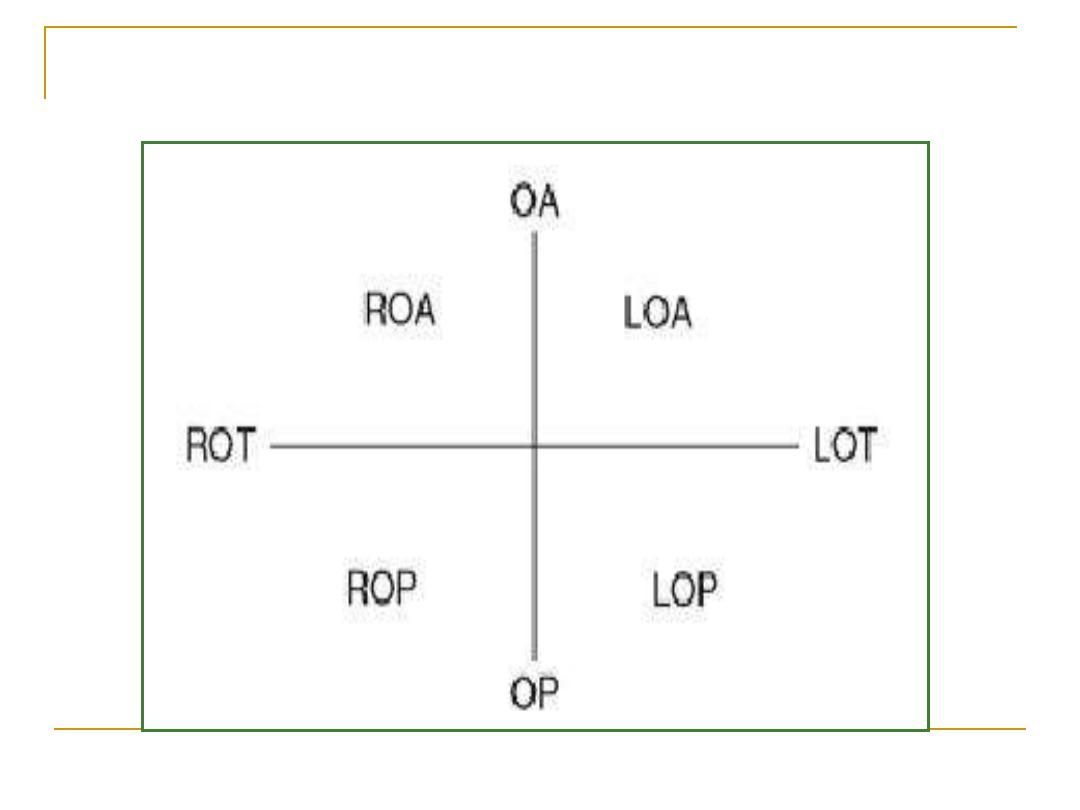
the position of the presenting part
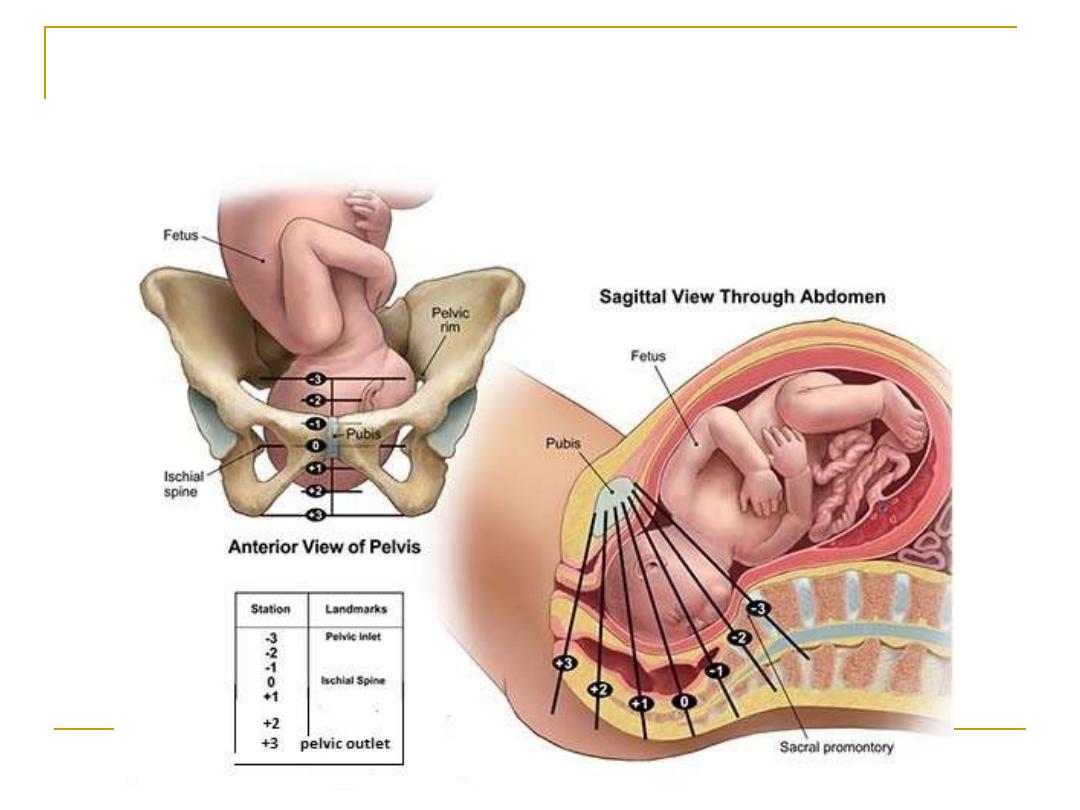
Engagement (and stations of fetal head during
delivery)
Normal Labour / 3
rd
Lecture
Mechanism of Labour
Reference Textbook
Dr. Suhaila Al-Shaikh Obstetrics by ten teachers
20
th
ed(2017): ch 12; p 386-89
Learning objectives
To understand the cardinal movements of
the fetal head when it passes through the
maternal pelvis and the effect of maternal
pelvis asymmetry and fetal skull asymmetry
in directing these movements
Mechanisms of labor, or the
cardinal movements of labor,
refer to the changes in
position and attitude that the
fetal head undergoes during
its passage through the birth
canal.
In normal labour
( i.e: for the vertex presentation and the
gynaecoid pelvis).
The relation of the fetal head and fetal body to
the maternal pelvis changes as the fetus
descends through the pelvis.
To get the optimal diameters of the fetal skull
while it descends through the birth passage
The movements arranged in
order:
Engagement
Descent
Flexion
Internal rotation
Extension
External rotation and restitution
Delivery of anterior and posterior shoulders
Expulsion of the rest of the body
Engagement
-
1
Engagement is descent of the
biparietal diameter of the fetal
head below the plane of the
pelvic inlet.
The head enters the pelvis in the
occiput transverse position in
women with a gynecoid pelvis.
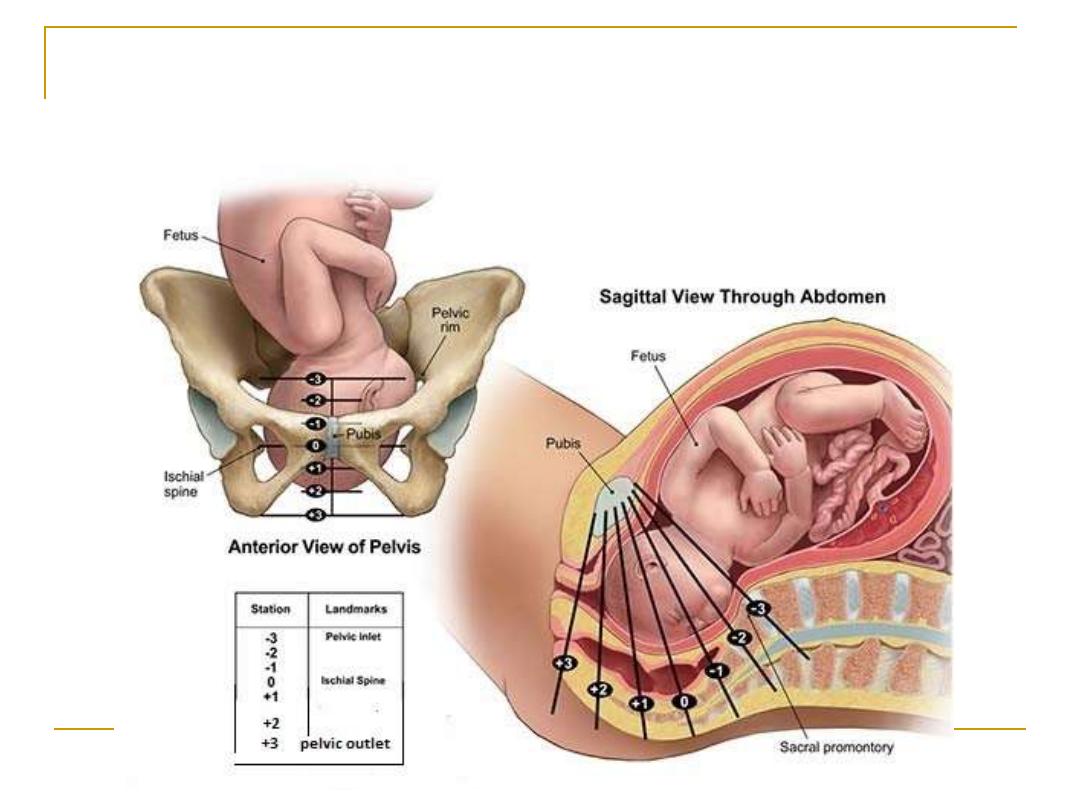
Engagement (and stations of fetal head during
delivery)
DESCENT:
-
2
When the uterus contract it
pushes the baby down through
the birth canal (
the fetal head
descend through the pelvic
brim to the midcavity).

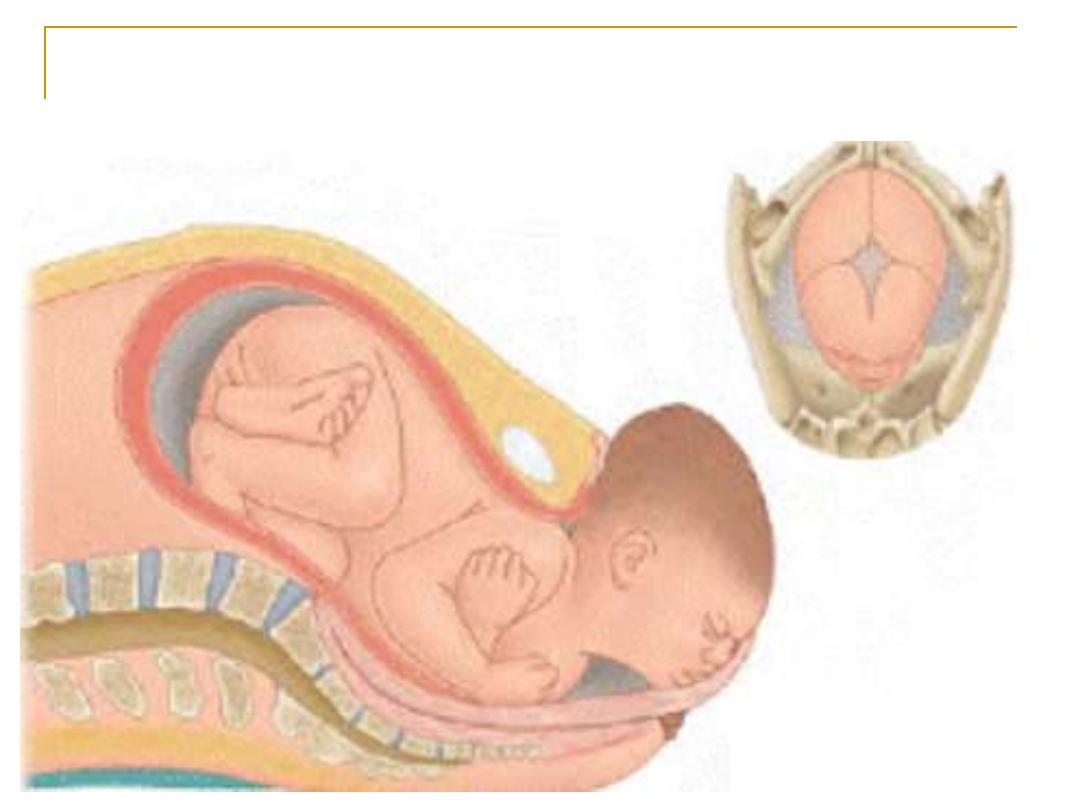
3- Flexion
Uterine activity is fundally dominant;
the line of force is down the fetal
spine and causes flexion of the
fetal head. flexion is a passive
movement that permits the
smallest diameter of the fetal head
(suboccipitobregmatic diameter) to
be presented to the maternal
pelvis.
With the progress at the
end of the first stage and
beginning of the 2
nd
stage
there is
further descent &
flexion
of the presenting
part (head) in the pelvis
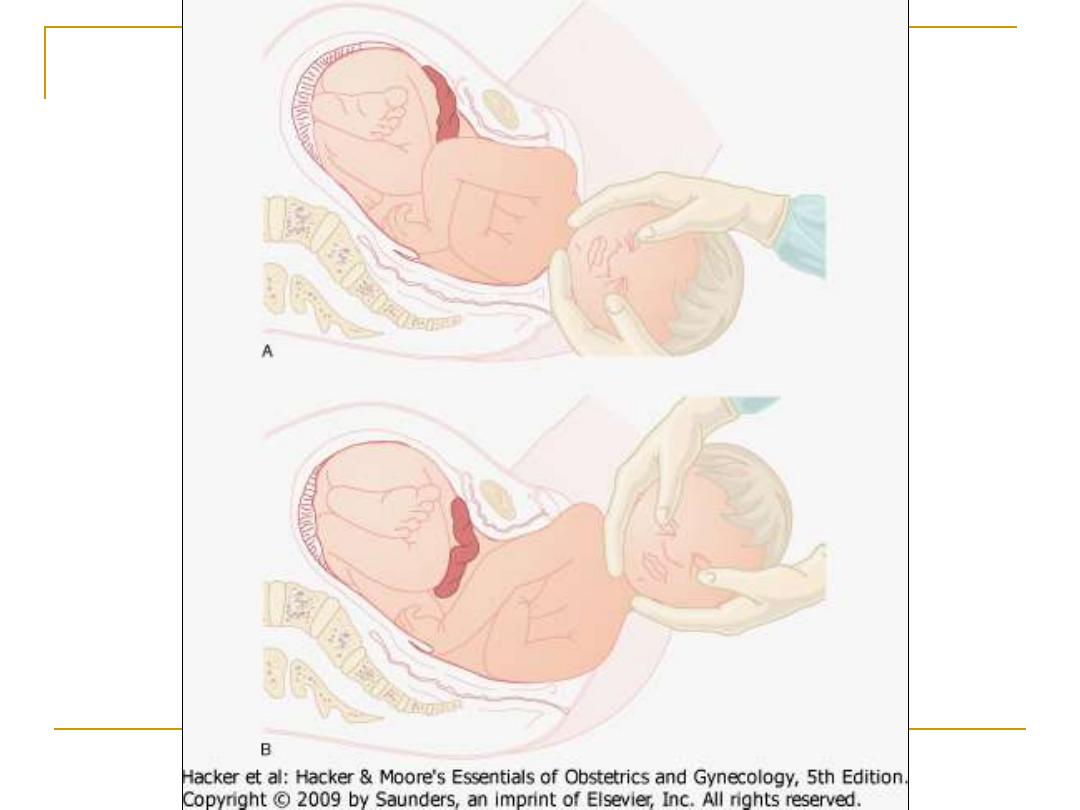
Internal rotation
-
4
The head rotates from the
left occipito-transverse
position at engagement to
become direct occipito-
anterior position.
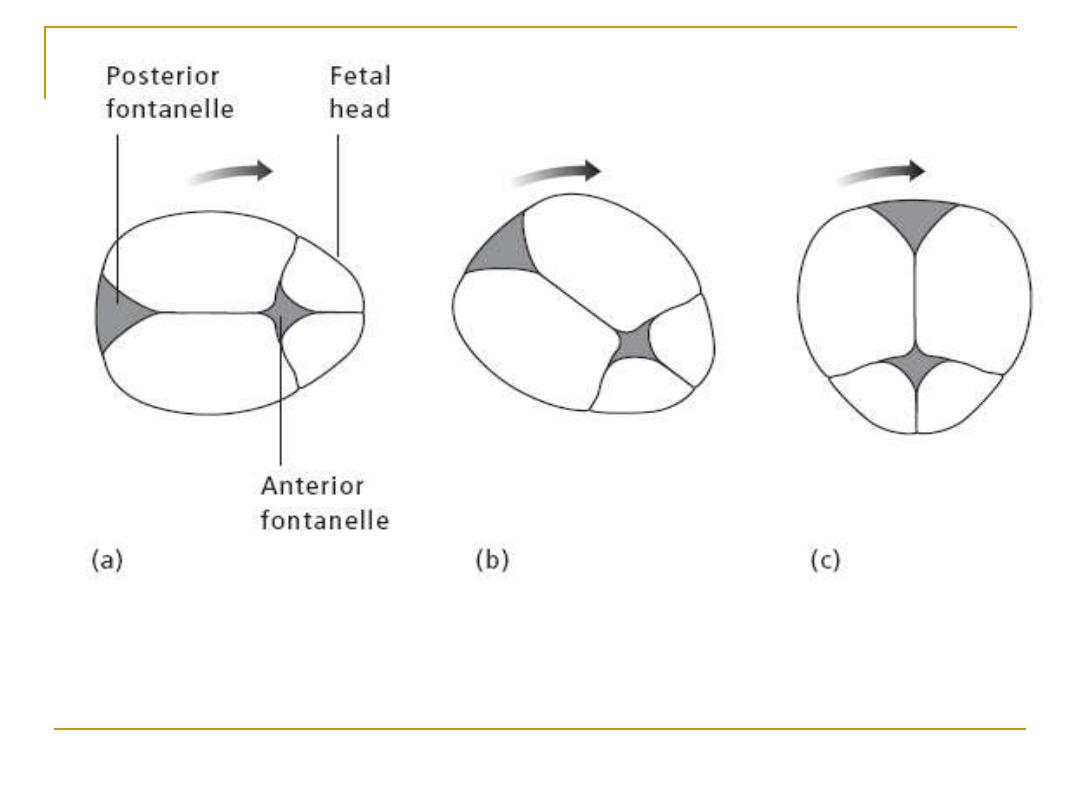
Internal rotation of the head. (a) Inlet: right
occipitotransverse position. (b) Mid-cavity: right
occipitoanterior position. (c) Outlet: direct
occipitoanterior position
Further descent through the
pelvis causes the chin to be
forced tightly up against the
fetal chest.
Extension
-
5
As the head continues its descent,
The fetal occiput comes to lie
behind the maternal symphysis
pubis, gradual extension of the
fetal head occurs distending the
perineum
With more extension, the widest
diameter passes through the
vulval introitus (crowning) and
the head is born by extension at
the fetal neck.
Extension
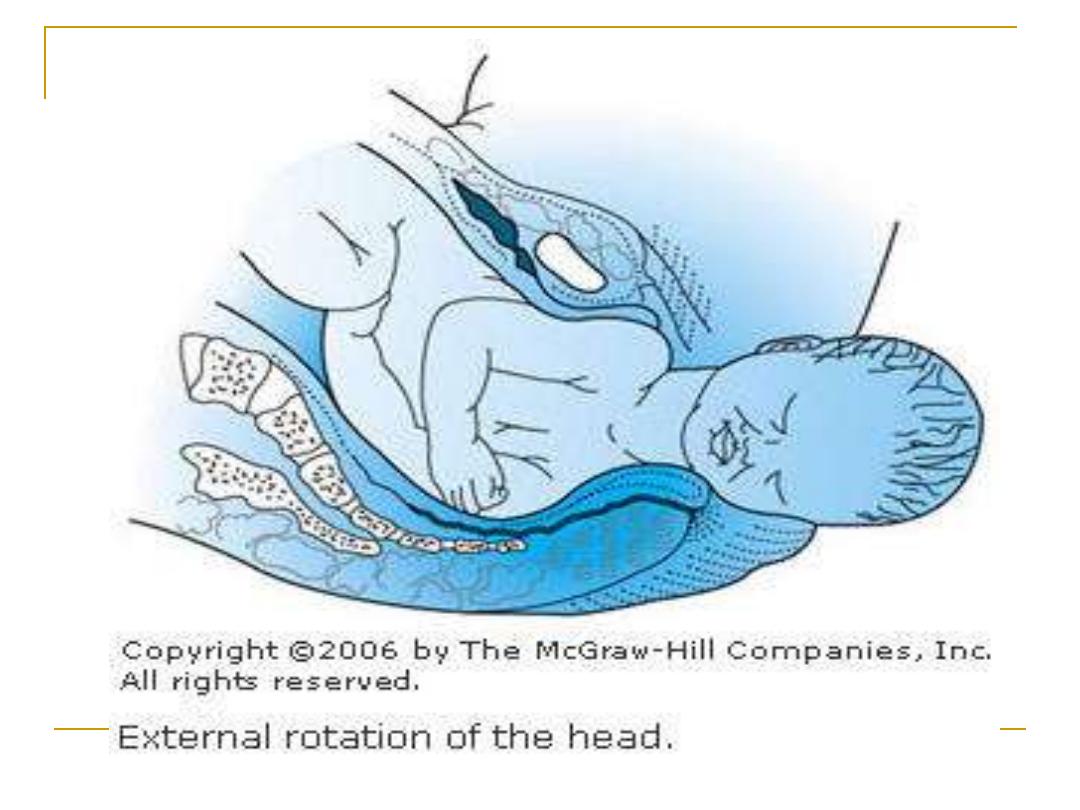
Restitution and external
-
6
rotation
As the head is being born, the shoulders
enter the maximum diameter (the
transverse diameter) of the maternal
pelvic inlet. As they descend through the
canal, the shoulders rotate (just as the
head did in internal rotation) and, as they
do so, the head (outside the body now)
rotates 90
°. The shoulders now lie in the
anteroposterior diameter behind the
maternal symphysis pubis.
Delivery of the body
-
7
Delivery of the anterior shoulder is
aided by gentle downward traction
on head. The posterior shoulder is
then delivered by gentle upward
traction on the head. Following
these maneuvers, the body, legs,
and feet are delivered with gentle
traction on the shoulders.
features of normal labour?
1. Spontaneous onset at 37
–42 weeks’ gestation.
2. Singleton pregnancy.
3. Cephalic vertex presentation.
4. No artificial interventions.
5. Cervical dilatation of at least 1 cm every 2 hours
in the active phase of first stage.
6. Active second stage no more than 2 hours in
primiparous and 60 minutes in multiparous
woman.
7. Spontaneous vaginal delivery.
8. Third stage lasting no more than 30 minutes
with active management.