
Road traffic injuries
جروح وسائط النقل
• Injuries and fatalities occur in all forms of transportation but
numerically road traffic accidents account for the great majority
worldwide, causing more than 3000 deaths each day and killing
more than a million people annually and injuring some 20–50
million. I
• If the current trends continue, road traffic injuries are
• predicted to come the fifth leading cause of death
• by 2030. Approximately 90 per cent of these deaths
• occur in low- and middle-income countries, where the road traffic
fatality rates (21.5 and 19.5 per 100,000 population, respectively)
are higher than in high income countries (10.3 per 100,000
population

Facial lacerations from a shattered windscreen in an unrestrained driver.
The toughened glass breaks into small fragments, which produce the
characteristic ‘sparrowfoot’ marks. The laceration on the forehead was
made by the windscreen rim.
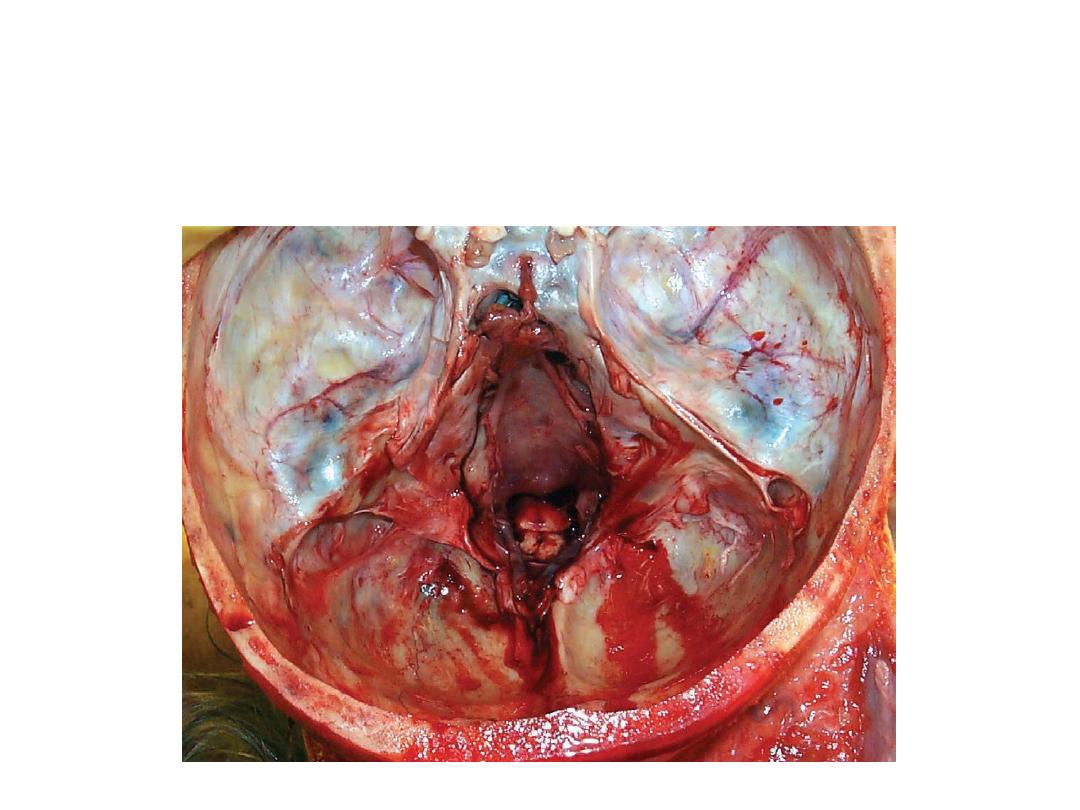
Ring fracture around the foramen magnum caused by
an impact on the crown of the head in a car
driver, who lost the control of his vehicle and crashed
into a tree.

Bruising, laceration and bilateral leg fractures
of a car driver in a frontal impact.

Facial injuries in a car driver unrestrained by a seatbelt. Following a
deceleration impact his face struck the windscreen, causing the typical small
cuts from broken safety glass and lacerations of the temple from striking
the windscreen rim or ‘A’ frame.

Mixed injuries in a restrained car driver from a head-on
collision. Death was caused by ruptured aorta.
Ruptured aorta in which the car occupant, unrestrained by
seatbelt, suffered severe deceleration. Aorta has torn in the
usual place, the distal arch where the curve of the vessel meets
the thoracic spine.
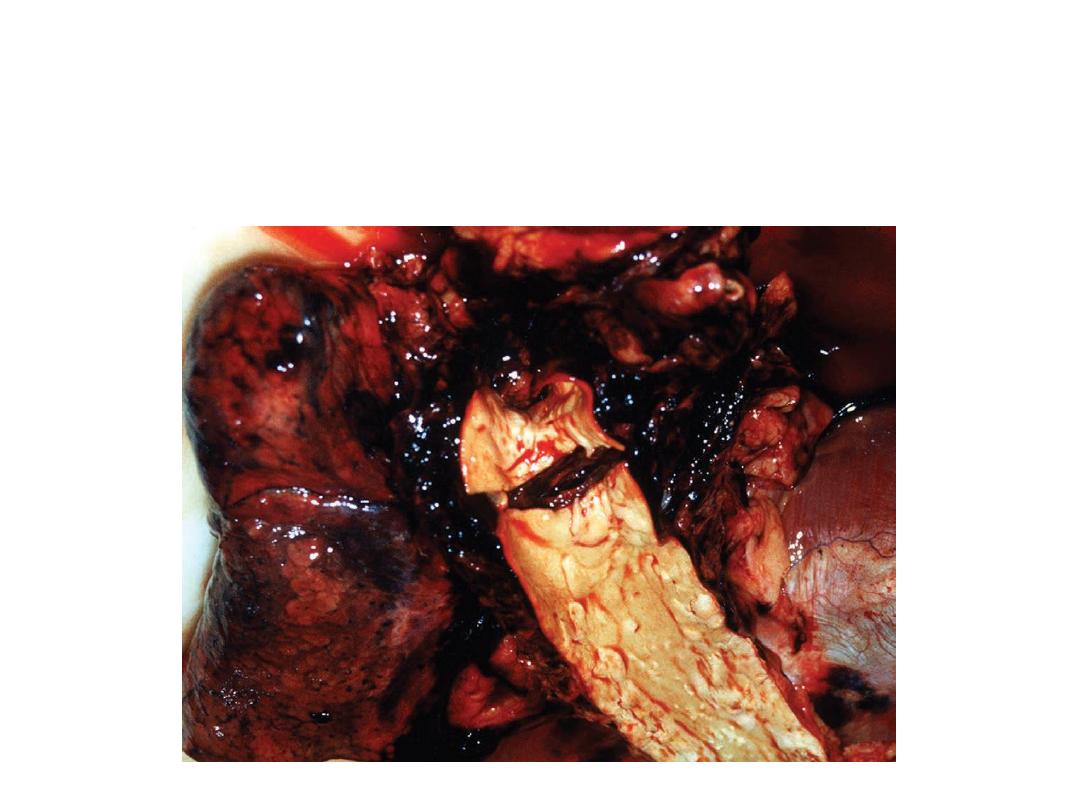
A car collided with a mobile home towed by an oncoming car.
The caravan broke into pieces and a wooden component
impaled the head of a car passenger.

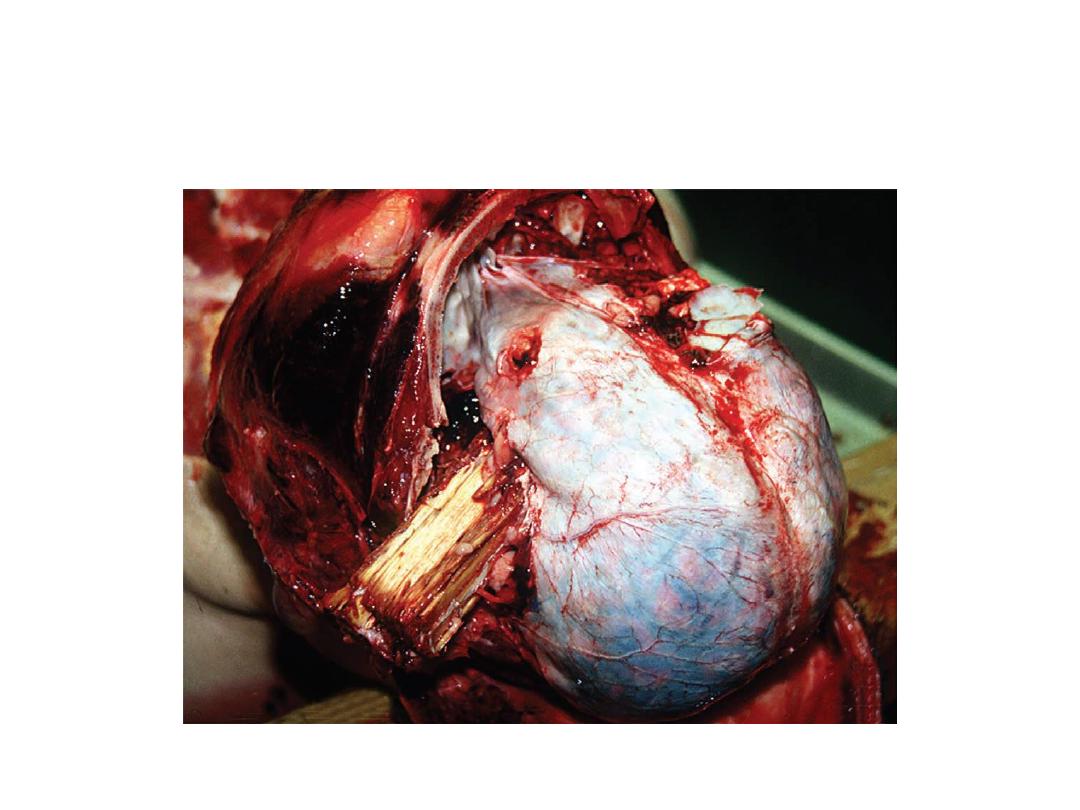
Penetration of the wrist and chest by a wooden component of
a bus seat. The victim drove his car at speed into a bus and part
of the resulting debris penetrated his left ventricle.
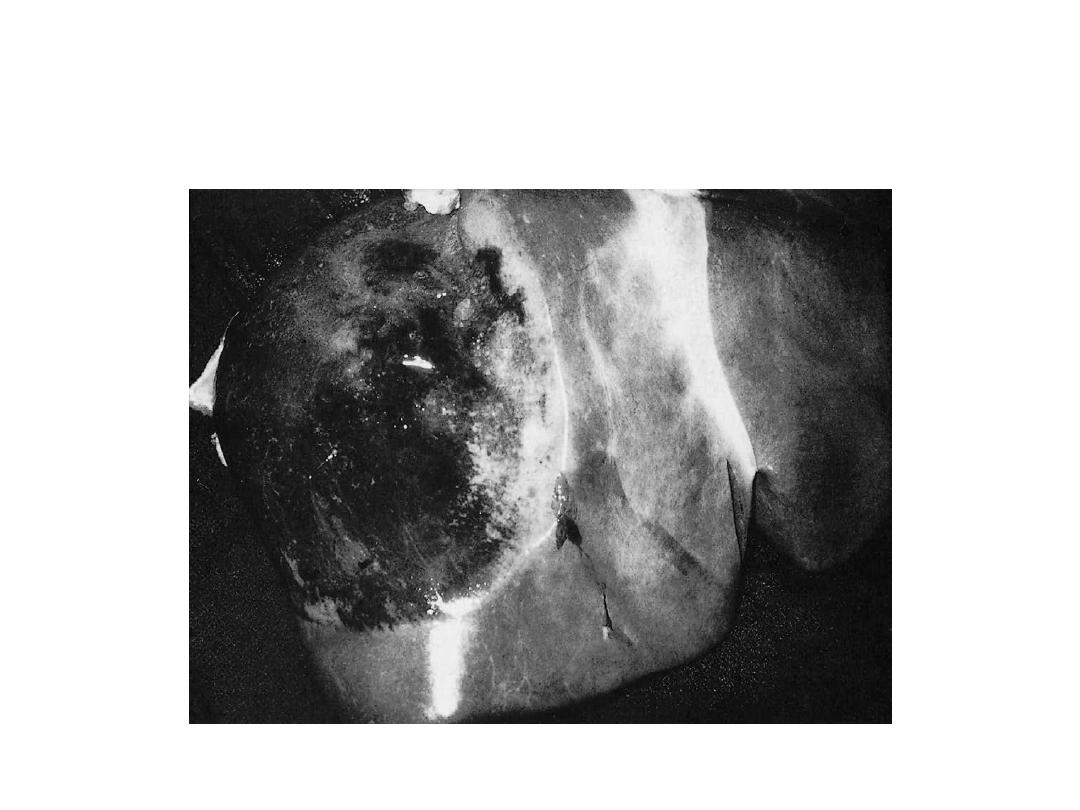
Large subscapular hemorrhage of the liver in a driver who struck the
rim of the steering wheel during severe deceleration. Such
subscapular lesions can remain intact for hours or even days, then
rupture into the abdominal cavity
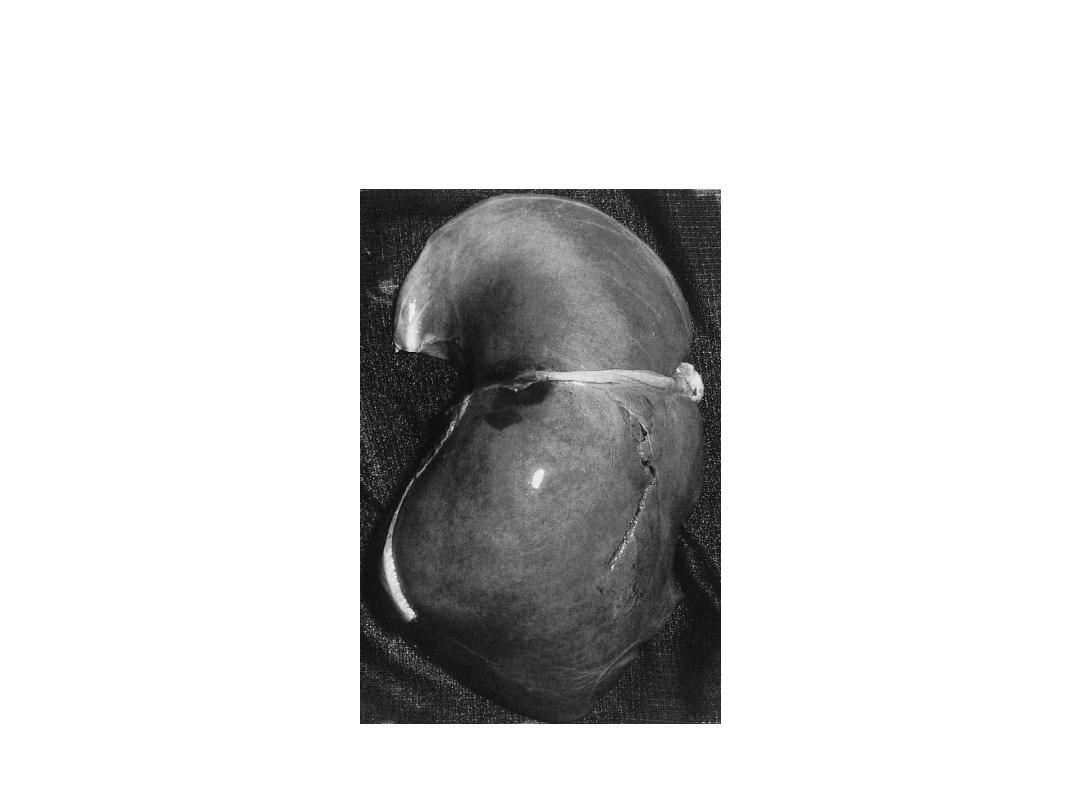
Anterior tear through the full thickness of the liver; there is
also a hemorrhage around the suspensory ligament. The victim
was a car driver who was impacted against the lover curve of
steering wheel in a frontal crash

Typical band-shaped subcutaneous haemorrhage due to
diagonal seatbelt injury.

Severe brush abrasions or ‘friction burns’ in a
motorcyclist, who came off his machine and skidded
across the road surface.
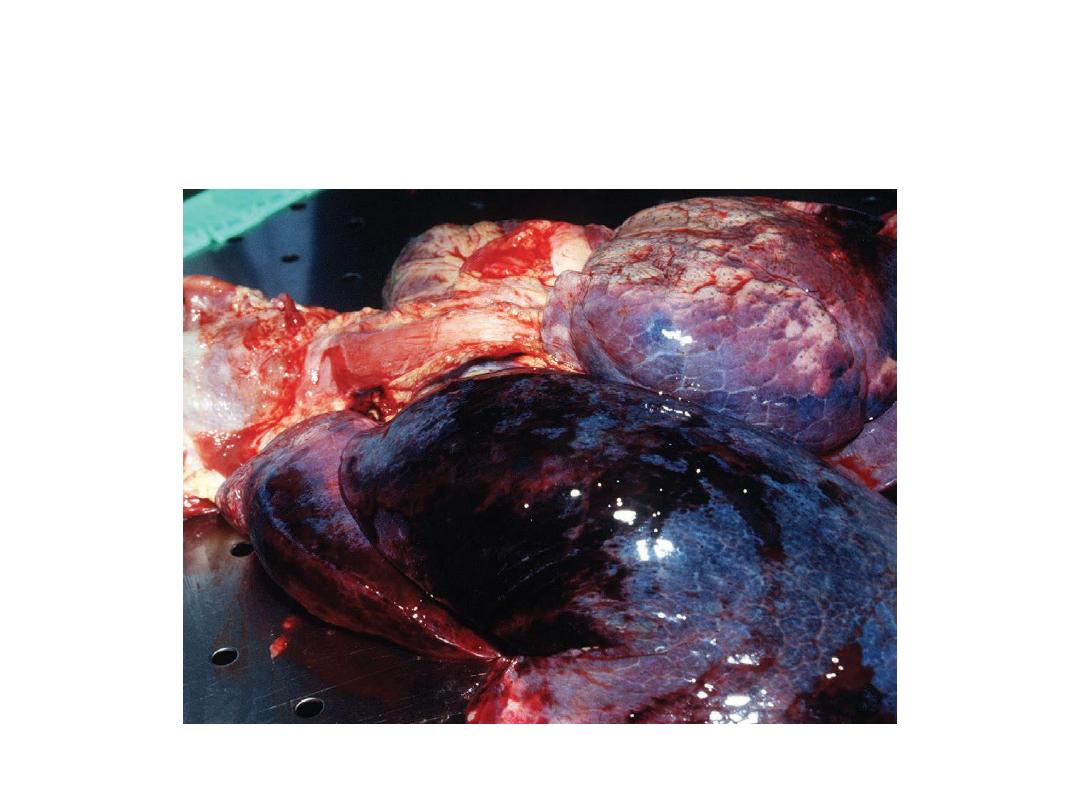
Pulmonary contusions in a motorcyclist, who collided with a
truck and was hurled into a signpost. Death was caused by a
cranial fracture and multiple injuries of the internal organs

Primary injury to a pedestrian struck by a car. There is damage to both legs
at about the same level, with a compound fracture of the right leg. These
are sometimes called ‘bumper fractures’. The height of the injuries above
heel level should always be measured at autopsy

Abrasions and laceration at knee level in a pedestrian struck by a car
bumper. Their anterior position indicates that the victim was facing the
vehicle at the moment of contact, but this may be a last-instant turn during
final awareness of the car’s proximity.
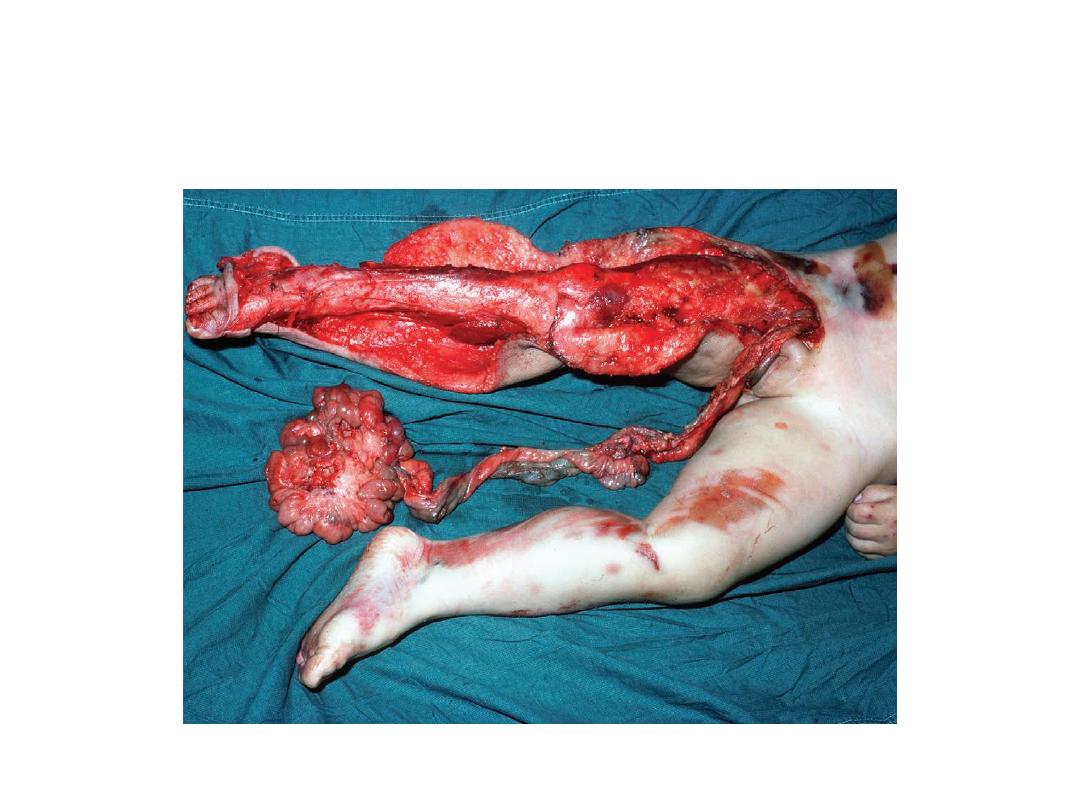
Injuries caused by being run over by a bus. The large rotating wheel has
‘flayed’ the right leg, stripping the skin and subcutaneous tissues from the
muscles. The passage of the adjacent double wheel over the abdomen has
extruded the intestines through the perineum

A patterned injury in a pedestrian struck by a truck. The circular bruise and
abrasion over the front of the left shoulder are from a headlamp rim. There
is also a well demarcated imprint around the left eye from some other
projection on the vehicle.

Primary pedestrian injury. The pattern is caused by the bumper bar striking
the leg. The height from the heel should always be measured for the police
to compare with the vehicle – though during extreme braking, many
vehicles will dip down at the front, thus lowering their bumper height

Intradermal bruising on the forehead of a live boy who was found
wandering in the street with amnesia for recent events. He had been struck
by a ‘hit-and-run’ car, which left identifiable tyre marks on the skin. An
astute casualty officer had a photograph taken as the marks faded in a few
hours.

Intradermal bruising reflecting the tyr tread pattern.
Note the bruising is of the ‘valleys’ and not the ‘hills’
in the tread.
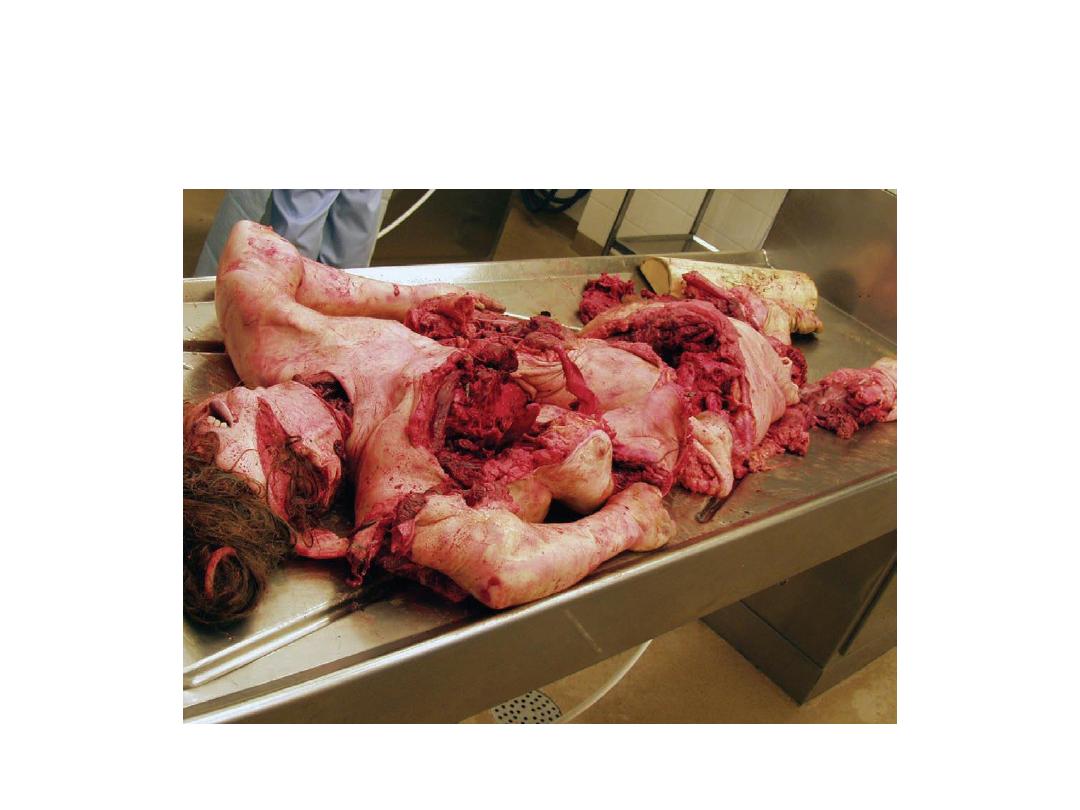
Extensive disintegration of the body that has been run
over by a train.

Burning
الحروق
• Damage to the tissues arising from the
application of heat, which is either dry or wet
heat and commonly encountered in forensic
pathology,
and
sometimes
provides
a
challenging
problem
in
the
distinction
between
ante-mortem
and
post-mortem
burning, which may have serious criminal
aspects.
Scalds or wet burns in a child accidentally left in a hot bath while her
mother went to answer the telephone. This illustrates that time, as
well as temperature, is a factor in causing heat damage to skin. The
child died some days later from an intercurrent chest infection.
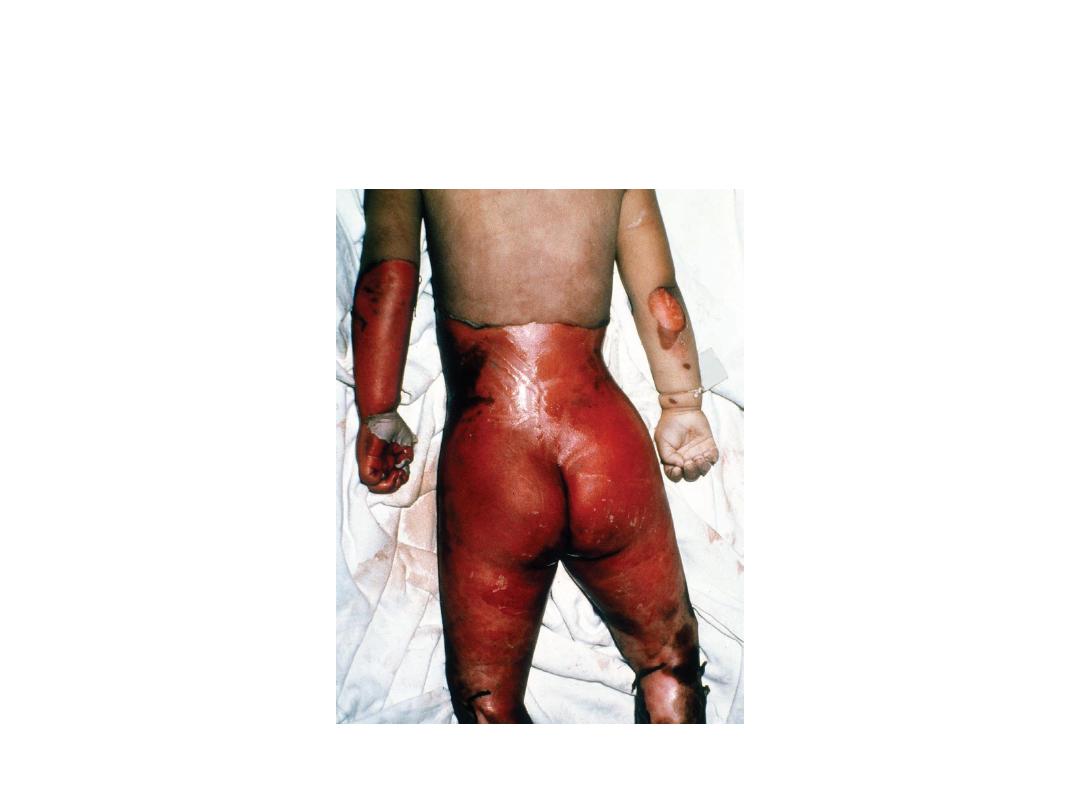
First- and second-degree burns on the right thigh and scrotum of a 5-
year-old diabetic child, who had been treated by a ‘quack’, who had
promised the parents to cure the child by hot baths. Death was
caused by the untreated diabetes.
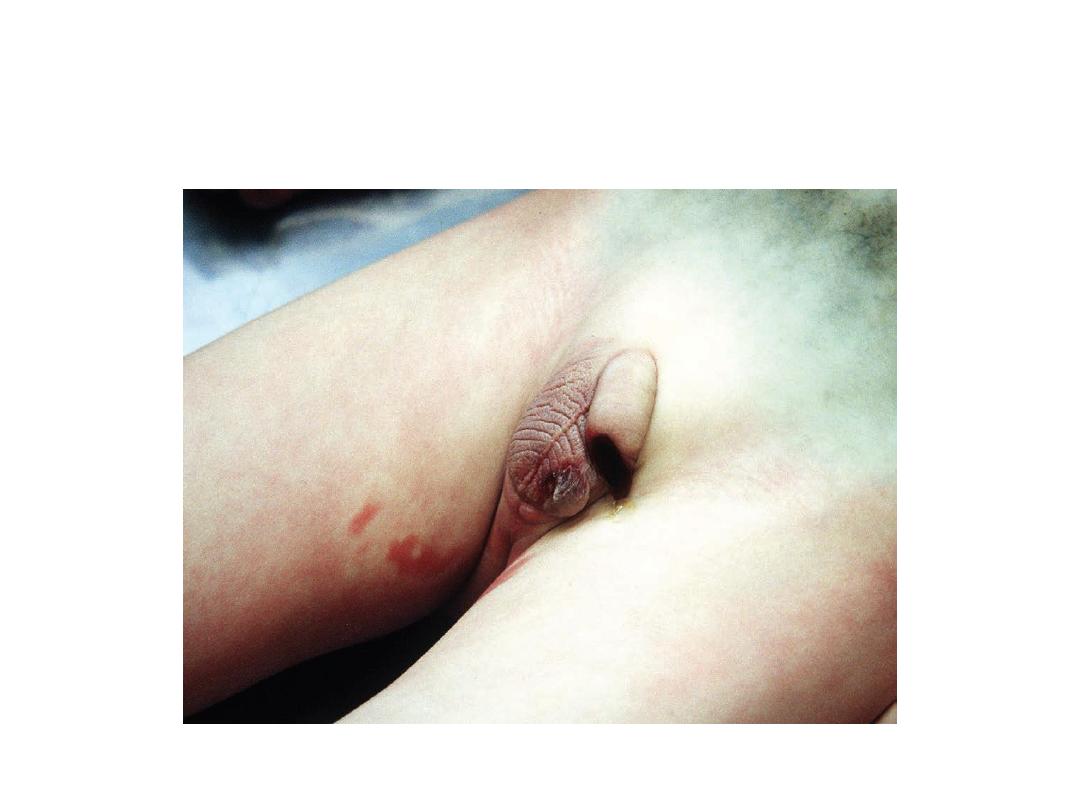
A second degree burn in a house fire victim. Note the pink
colouration of the hypostasis due to carbon monoxide poisoning and
the vertical pale pressure marks produced by clothing
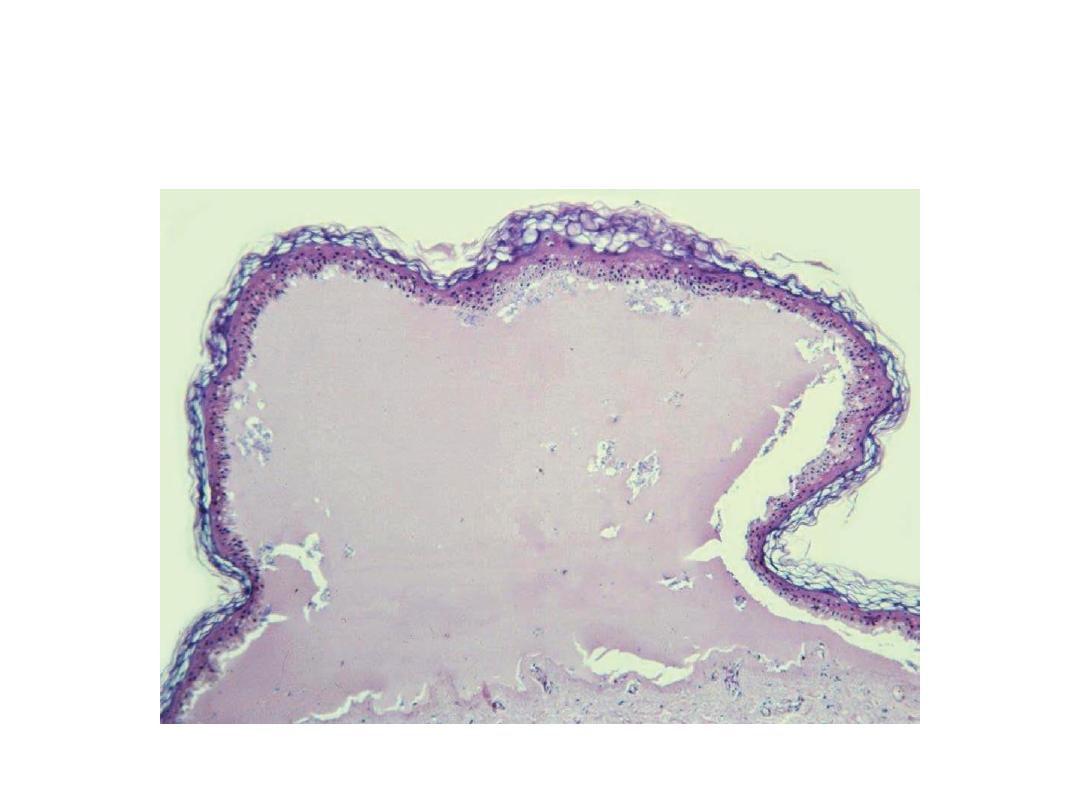
Haematoxylin-eosin-stained histological section of a second degree
burn showing a blister filled with eosinophilic liquid covered by a thin
layer of epidermis

Body of a 42-year-old male found dead in the steam room approximately 8 hours after having
gone alone to sauna. Blood alcohol concentration 2.3 per mille; urine alcohol concentration 3.2
per mille. Due to the long heat exposure, a ‘parboiled’ appearance with patchy loss of
epidermis due to skin slippage was found when the body was recovered and showing post-
mortem drying of the lesions.
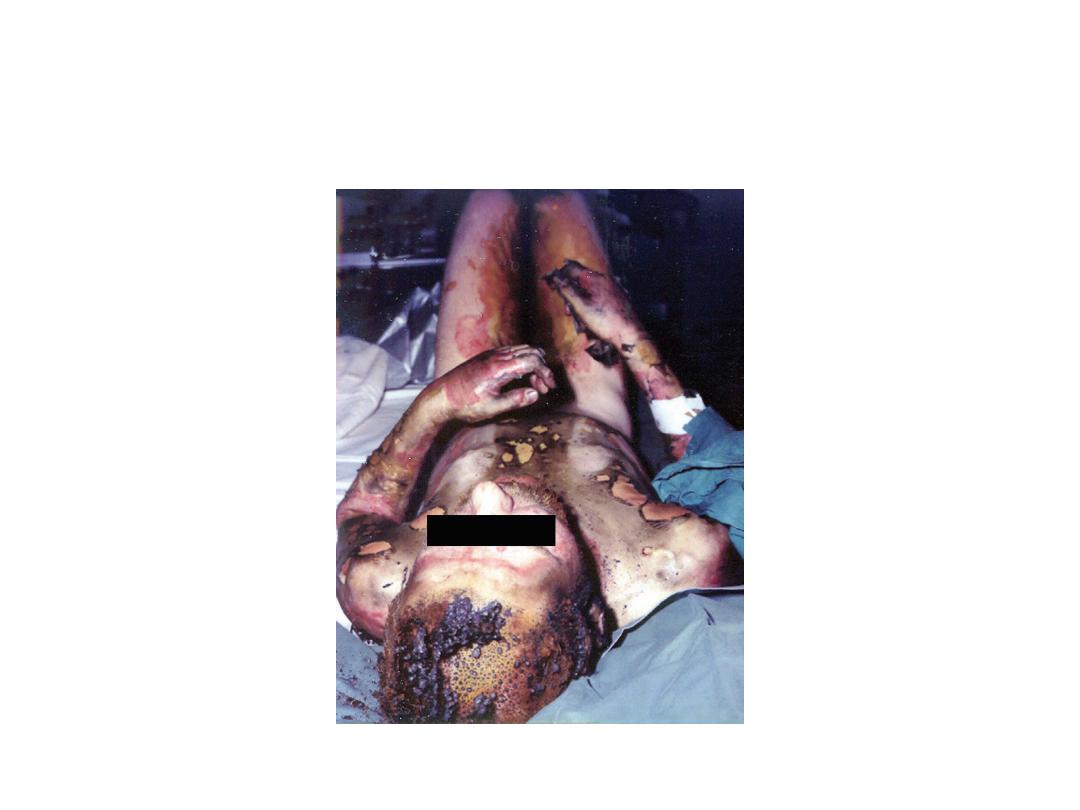
Second- and third-degree burns and singeing
of hair on a suicide who doused himself with petrol and set
himself on fire

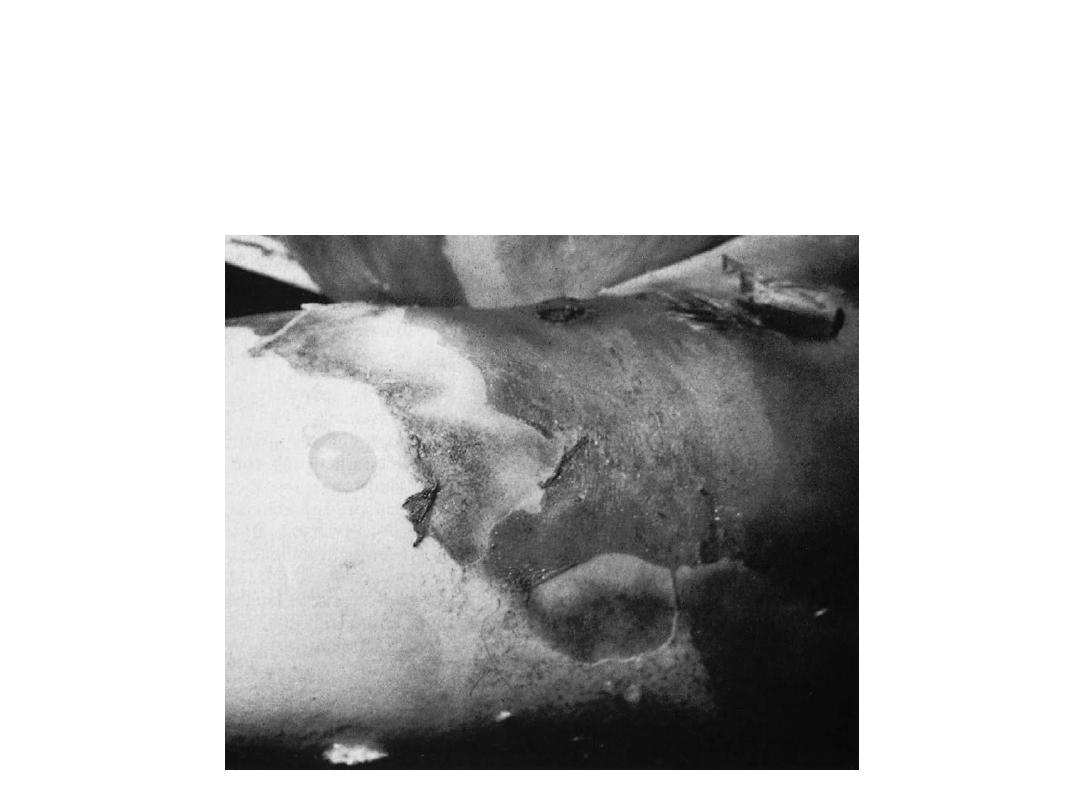
Post-mortem smoke soiling and superficial burns on the leg of a
house-fire victim who died of smoke inhalation. Note the complete
protection of the skin, which had been covered only by a sock.
Heat flexures of the limbs, part way towards the ‘pugilistic attitude’
formed when the arms are raised higher. The elbows, knees and
wrists are strongly flexed because muscle contraction is stronger in
the flexor groups.
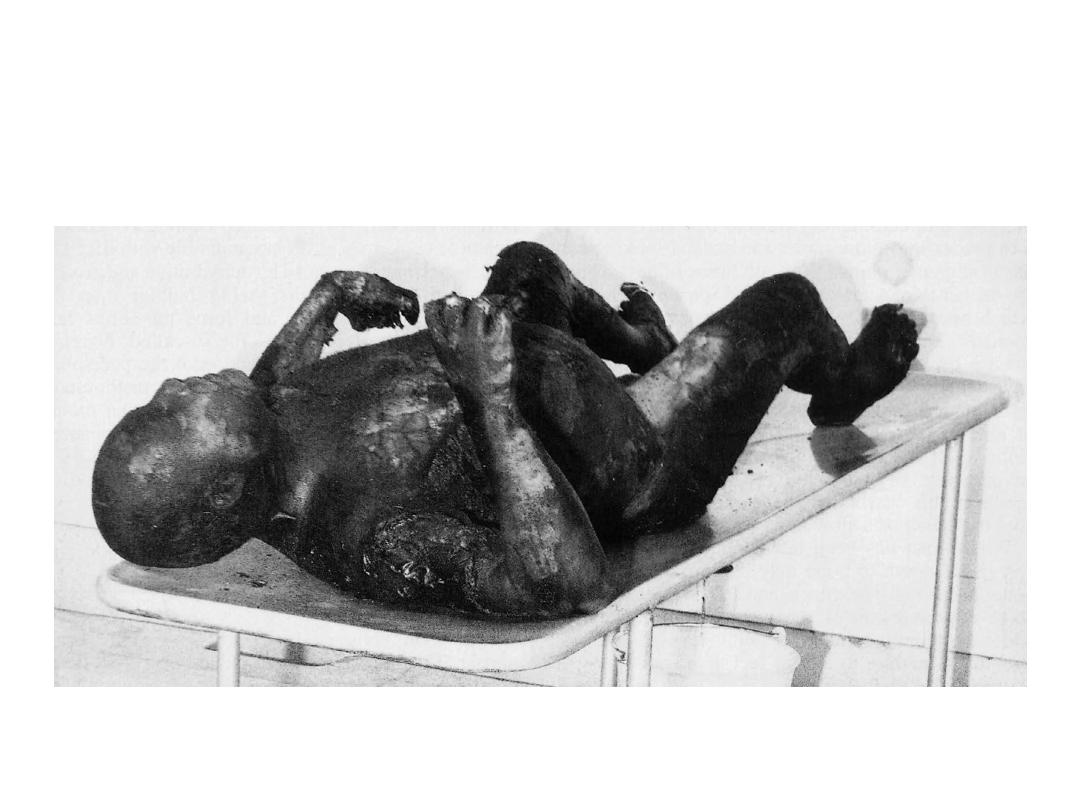
Charred body at the scene of a fire showing the
pugilistic attitude’ and post-mortem skin splits on
the chest.
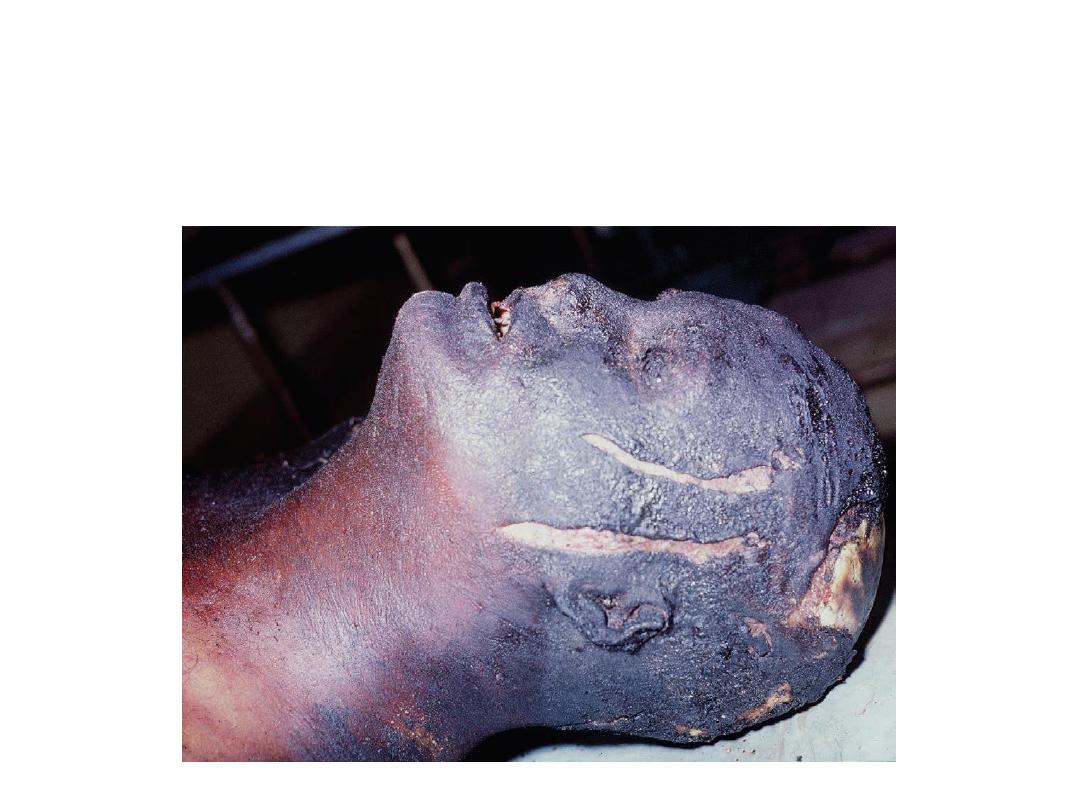
Post-mortem injuries caused by heat simulating head injuries. The fire service were
concerned about an apparent preconflagration assault, but such skin splits are
commonly seen as a result of heat contracture of the tissues. The scalp on the top of
the head has been burned through and the skull is charred. Beneath this is a
spurious ‘heat haematoma’, sometimes confused with a traumatic extradural
haemorrhage

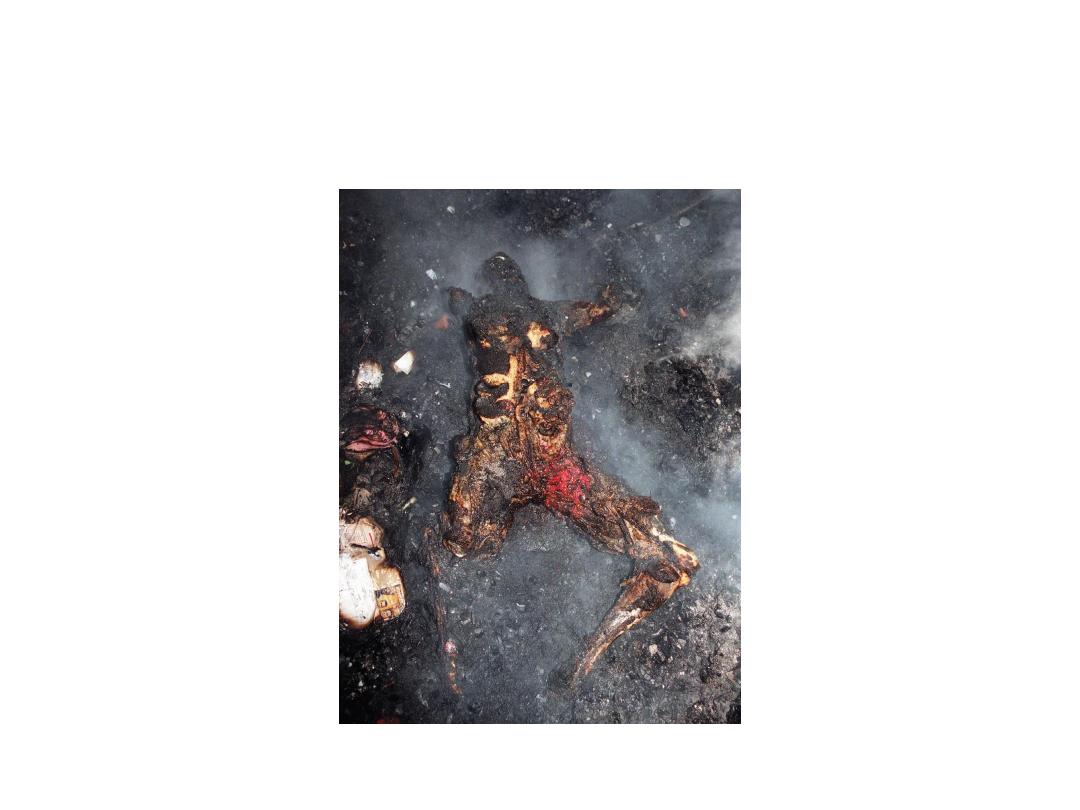
Post-mortem burns in a victim recovered from a house fire. Note the raised
right arm caused by heat contractures. The left forearm has burnt up to the
elbow and there is extensive skin splitting on the left brachium and
shoulder area. The left side is charred but the pelvis has been better
protected by clothing.
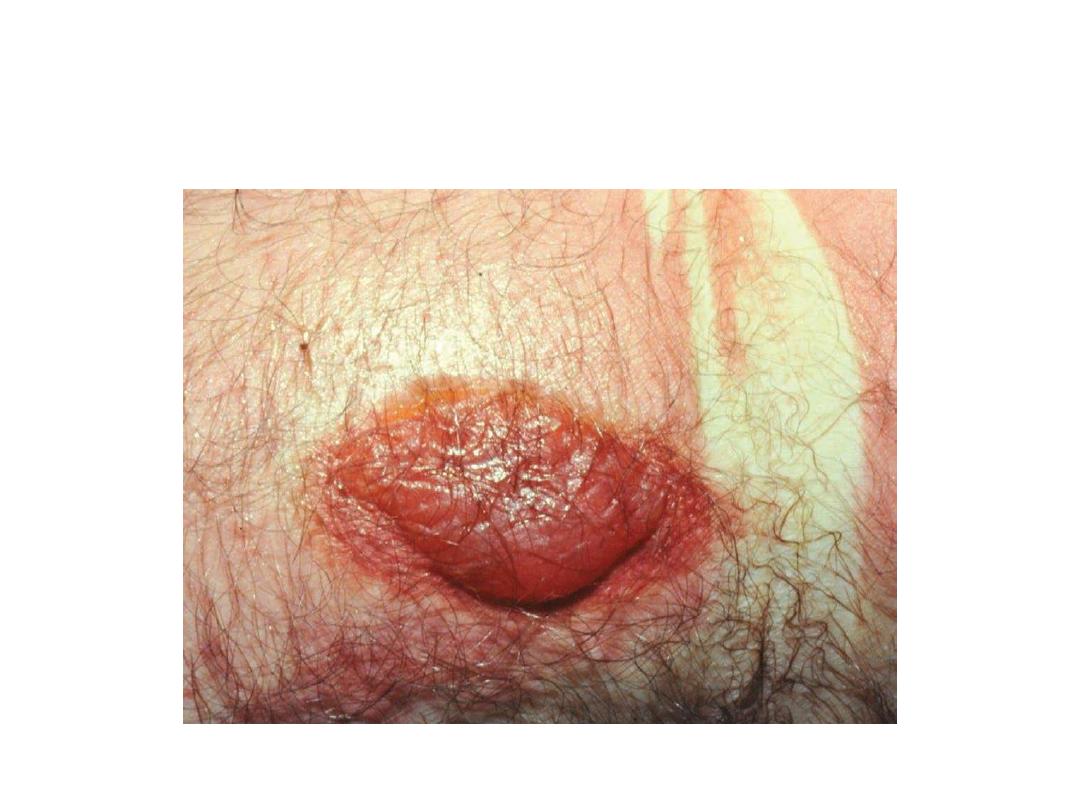
It can be difficult or impossible to differentiate between ante-mortem and
post-mortem burns when they are sustained near to the time of death. Here
the blister with no erythema at the base could either be post-mortem or
ante-mortem, as reddening of the margins and adjacent skin can occur for
at least 1 hour after death. It is preferable to call doubtful lesions ‘peri-
mortal’.

Post-mortem burn on the arm and chest caused by a hot-water bottle being left over
the heart in an attempt at resuscitation. The lesion is sharp-edged, there is no
erythematous margin, and the surface is brown and leathery from post-mortem
drying.
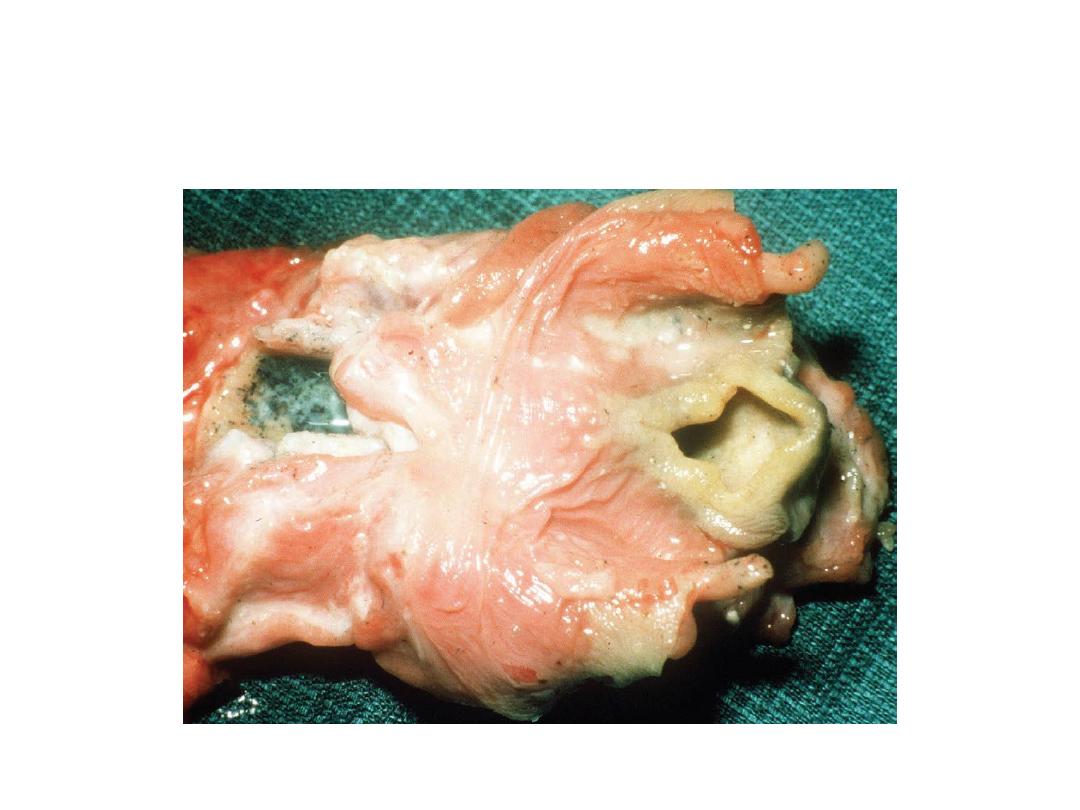
Larynx of a house-fire victim showing heat blanching of the epiglottis and
glottal entrance from breathing hot gas. The lower cut end of the trachea
shows copious soot-containing mucus, also indicating respiration during the
fire.
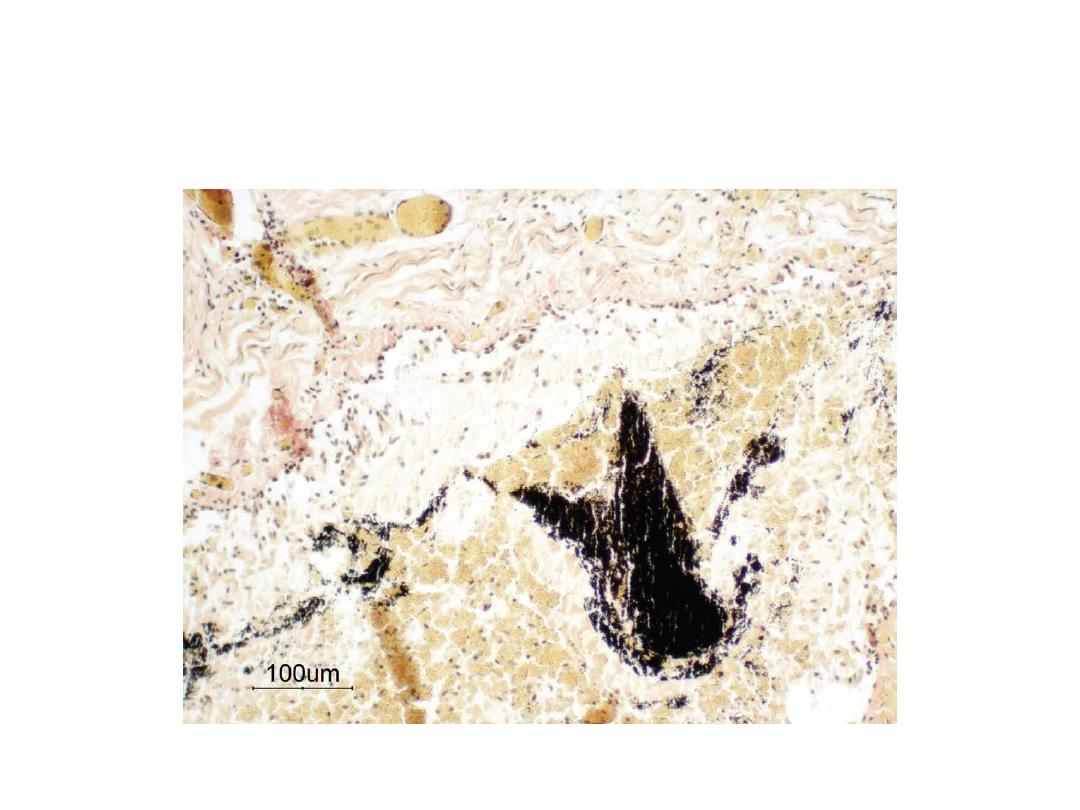
As small bronchus from a fire victim, showing histological evidence of
soot deposition, together with desquamation of the epithelium and
plugging with cellular
Soot in the tracheal mucus, a sign of breathing while the fire was in progress. Though
soot can passively reach the glottis after death if the mouth is open, it cannot reach
the lower air passages in any significant quantity. Histology of the smaller bronchi
offers complete proof of active respiration.

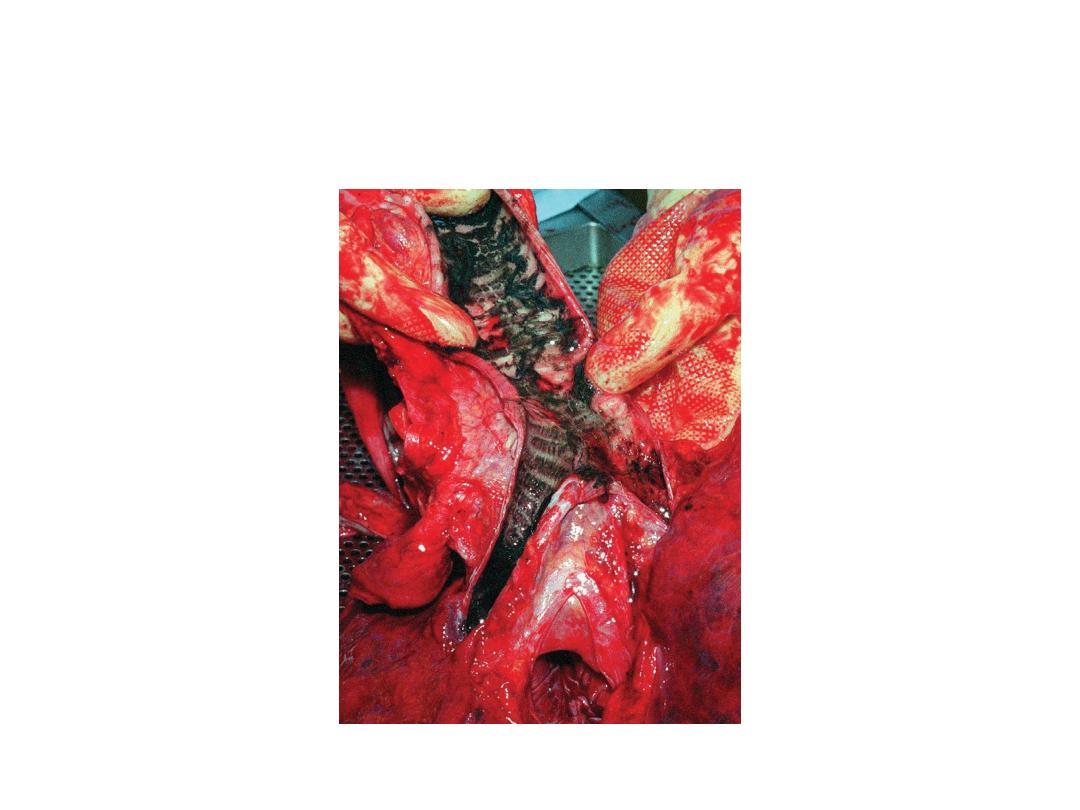
Soot in oesophagus of a house-fire victim indicating respiration
during the fire.




