GIT system
INGESTION OF FOODThe amount of food that a person ingests is determined principally by an intrinsic desire for food called hunger. The type of food that a person preferentially seeks is determined by appetite. These mechanisms are extremely important for maintaining an adequate nutritional supply for the body and in relation to nutrition of the body.
Mechanisms of food ingestion:
• Mastication ( chewing)
The teeth are admirably designed for chewing. The anterior teeth (incisors) provide a strong cutting action, and the posterior teeth (molars) provide a grinding action. All the jaw muscles working together can close the teeth with a force as great as 55 pounds on the incisors and 200 pounds on the molars.Most of the muscles of chewing are innervated by the motor branch of the fifth cranial nerve, and the chewing process is controlled by nuclei in the brain stem. Stimulation of specific reticular areas in the brain stem taste centers will cause rhythmical chewing movements. In addition, stimulation of areas in the hypothalamus, amygdala, and even the cerebral cortex near the sensory areas for taste and smell can cause chewing.
Much of the chewing process is caused by a chewing reflex. The presence of a bolus of food in the mouth at first initiates reflex inhibition of the muscles of mastication, which allows the lower jaw to drop. This action automatically raises the jaw to cause closure of the teeth, but it also compresses the bolus again against the linings of the mouth, which inhibits the jaw muscles once again, allowing the jaw to drop and rebound another time; this process is repeated again and again.
Chewing is important for digestion of all foods, but it is especially important for most fruits and raw vegetables because they have indigestible cellulose membranes around their nutrient portions that must be broken before the food can be digested. Furthermore, chewing aids the digestion of food for another simple reason: Digestive enzymes act only on the surfaces of food particles; therefore, the rate of digestion is dependent on the total surface area exposed to the digestive secretions.
2. Swallowing (Deglutition)
Swallowing is a complicated mechanism, principally because the pharynx subserves respiration and swallowing. The pharynx is converted for only a few seconds at a time into a tract for propulsion of food. It is especially important that respiration not be compromised because of swallowing..In general, swallowing can be divided into
• a voluntary stage, which initiates the swallowing process;• a pharyngeal stage, which is involuntary and constitutes passage of food through the pharynx into the esophagus; and
• an esophageal stage, another involuntary phase that transports food from the pharynx to the stomach.
• Voluntary Stage of Swallowing.
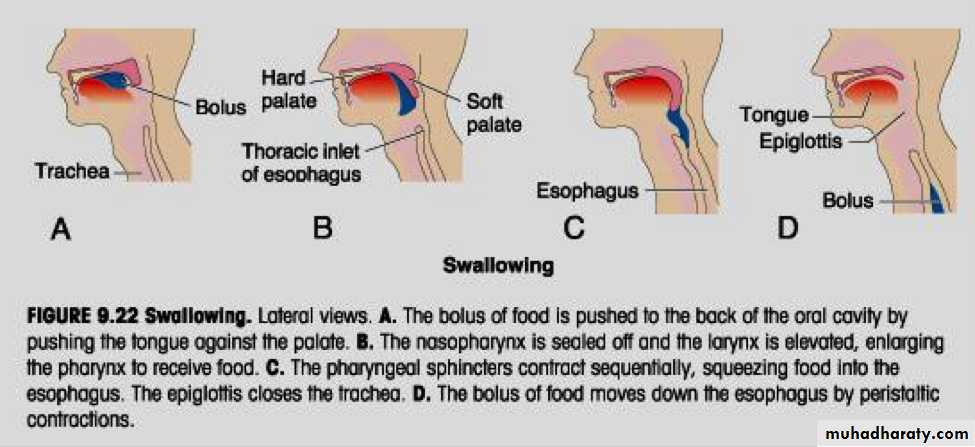
When the food is ready for swallowing, it is “voluntarily” squeezed or rolled posteriorly into the pharynx by pressure of the tongue upward and backward against the palate, as shown in Figure.2. Involuntary Pharyngeal Stage of Swallowing
As the bolus of food enters the posterior mouth and pharynx, it stimulates epithelial swallowing receptor areas all around the opening of the pharynx, especially on the tonsillar pillars, and impulses from these areas pass to the brain stem to initiate a series of automatic pharyngeal muscle contractions as follows: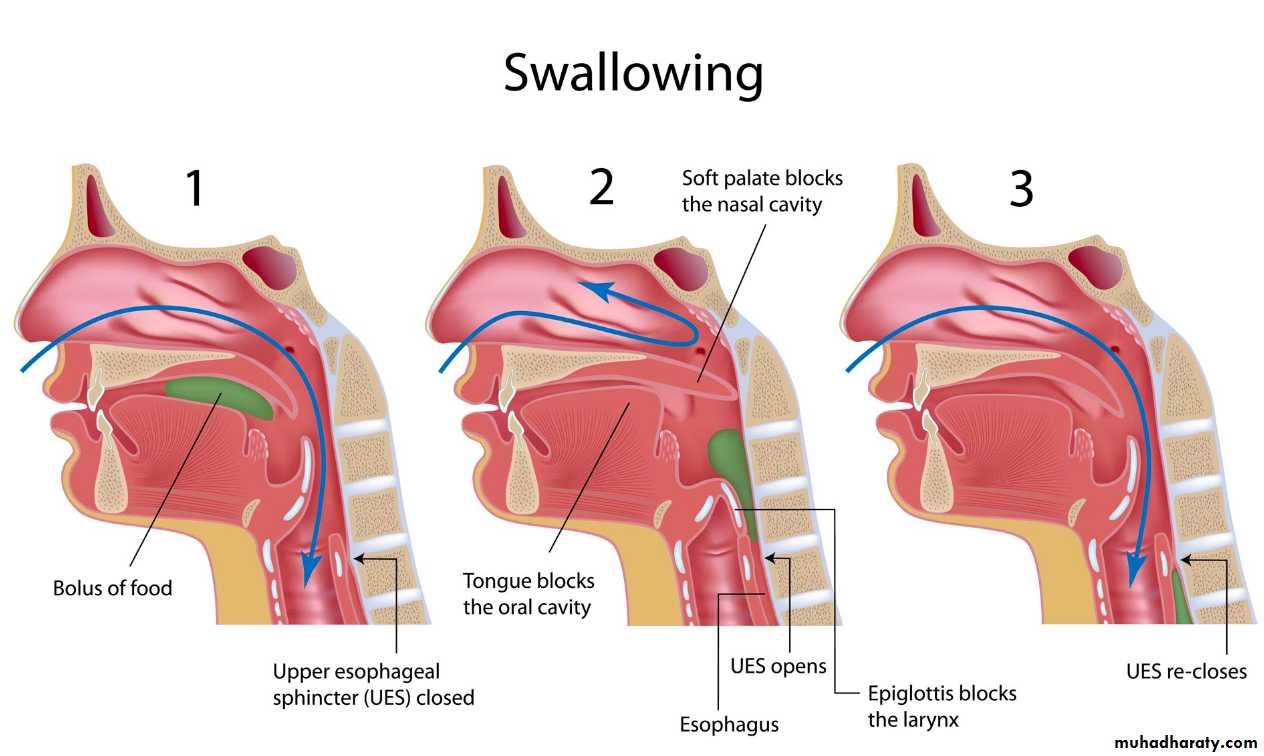
1. The soft palate is pulled upward to close the posterior nares to prevent reflux of food into the nasal cavities.
2. The palatopharyngeal folds on each side of the pharynx are pulled medially to approximate each other. In this way, these folds form a sagittal slit through which the food must pass into the posterior pharynx. This slit performs a selective action, allowing food that has been masticated sufficiently to pass with ease. Because this stage of swallowing lasts less than 1 second, any large object is usually impeded too much to pass into the esophagus.
3. The vocal cords of the larynx are strongly approximated, and the larynx is pulled upward and anteriorly by the neck muscles. These actions, combined with the presence of ligaments that prevent upward movement of the epiglottis, cause the epiglottis to swing backward over the opening of the larynx. All these effects acting together prevent passage of food into the nose and trachea
4. The upward movement of the larynx also lifts the glottis out of the main stream of food flow, so the food mainly passes on each side of the epiglottis rather than over its surface; this action adds still another protection against entry of food into the trachea
5. Once the larynx is raised and the pharyngoesophageal sphincter becomes relaxed, the entire muscular wall of the pharynx contracts, beginning in the superior part of the pharynx, then spreading downward over the middle and inferior pharyngeal areas, which propels the food by peristalsis into the esophagus. To summarize the mechanics of the pharyngeal stage of swallowing: The trachea is closed, the esophagus is opened, and a fast peristaltic wave initiated by the nervous system of the pharynx forces the bolus of food into the upper esophagus, with the entire process occurring in less than 2 seconds.
3. The Esophageal Stage of Swallowing Involves Two Types of Peristalsis.
The esophagus functions primarily to conduct food rapidly from the pharynx to the stomach, and its movements are organized specifically for this function. The esophagus normally exhibits two types of peristaltic movements: primary peristalsis and secondary peristalsis. Primary peristalsis is simply continuation of the peristaltic wave that begins in the pharynx and spreads into the esophagus during the pharyngeal stage of swallowing.This wave passes all the way from the pharynx to the stomach in about 8 to 10 seconds. Food swallowed by a person who is in the upright position is usually transmitted to the lower end of the esophagus even more rapidly than the peristaltic wave itself, in about 5 to 8 seconds, because of the additional effect of gravity pulling the food downward. If the primary peristaltic wave fails to move all the food that has entered the esophagus into the stomach, secondary peristaltic waves result from distention of the esophagus itself by the retained food; these waves continue until all the food has emptied into the stomach.
The secondary peristaltic waves are initiated partly by intrinsic neural circuits in the myenteric nervous system and partly by reflexes that begin in the pharynx and are then transmitted upward through vagal afferent fibers to the medulla and back again to the esophagus through glossopharyngeal and vagal efferent nerve fibers. The musculature of the pharyngeal wall and upper third of the esophagus is striated muscle. Therefore, the peristaltic waves in these regions are controlled by skeletal nerve impulses from the glossopharyngeal and vagus nerves
In the lower two thirds of the esophagus, the musculature is smooth muscle, but this portion of the esophagus is also strongly controlled by the vagus nerves that act through connections with the esophageal myenteric nervous system. When the vagus nerves to the esophagus are cut, the myenteric nerve plexus of the esophagus becomes excitable enough after several days to cause strong secondary peristaltic waves even without support from the vagal reflexes. Therefore, even after paralysis of the brain stem swallowing reflex, food fed by tube or in some other way into the esophagus still passes readily into the stomach.
Function of the Lower Esophageal Sphincter (Gastroesophageal Sphincter).
At the lower end of the esophagus, extending upward about 3 centimeters above its juncture with the stomach, the esophageal circular muscle functions as a broad lower esophageal sphincter, also called the gastroesophageal sphincter. This sphincter normally remains tonically constricted with an intraluminal pressure at this point in the esophagus of about 30 mm Hg, in contrast to the midportion of the esophagus, which normally remains relaxed.When a peristaltic swallowing wave passes down the esophagus, “receptive relaxation” of the lower esophageal sphincter occurs ahead of the peristaltic wave, which allows easy propulsion of the swallowed food into the stomach. Rarely, the sphincter does not relax satisfactorily, resulting in a condition called achalasia.
stomach secretions are highly acidic and contain many proteolytic enzymes.
The esophageal mucosa, except in the lower one eighth of the esophagus, is not capable of resisting the digestive action of gastric secretions for long. Fortunately, the tonic constriction of the lower esophageal sphincter helps prevent significant reflux of stomach contents into the esophagus except under abnormal conditions
Additional Prevention of Esophageal Reflux by Valvelike Closure of the Distal End of the Esophagus.
Another factor that helps prevent reflux is a valvelike mechanism of a short portion of the esophagus that extends slightly into the stomach. Increased intraabdominal pressure caves the esophagus inward at this point. Thus, this valvelike closure of the lower esophagus helps to prevent high intra-abdominal pressure from forcing stomach contents backward into the esophagus. Otherwise, every time we walked, coughed, or breathed hard, we might expel stomach acid into the esophagus
https://www.youtube.com/watch?v=YQm5RCz9Pxc&feature=share
http://www.primalonlinelearning.com/digestive_system.aspxhttps://www.youtube.com/watch?v=wqMCzuIiPaM&feature=share
