
Internal medicine endocrine, DM Lec.4 Dr. Basim
Presenting problems in diabetes mellitus
Hyperglycaemia
▪ Symptoms of hyperglycaemia
▪ Thirst, dry mouth
▪ • Polyuria
▪ • Nocturia
▪ • Tiredness, fatigue, lethargy
▪ • Change in weight (usually weight loss)
▪ • Blurring of vision
▪ • Pruritus vulvae, balanitis (genital candidiasis)
▪ Headache
▪ • Hyperphagia; predilection for sweet foods • Mood change, irritability, difficulty in
concentrating, apathy
▪ Nausea
Rapid weight loss are prominent in type 1 diabetes but are often absent in patients with type 2
diabetes, many of whom are asymptomatic or have nonspecific complaints such as chronic
fatigue and malaise.
Uncontrolled diabetes is associated with an increased susceptibility to infection and patients
may present with skin sepsis (boils) or genital candidiasis, and complain of pruritus vulvae or
balanitis
Physical signs in patients with type 2 diabetes at diagnosis depend on the mode of presentation.
In Western populations, more than 80% are overweight and the obesity is often central (truncal
‘abdominal). Obesity is much less evident in Asians.
Hypertension is present in at least 50% of patients with
type 2 diabetes. Although dyslipidaemia is also common,
skin lesions such as xanthelasma and eruptive xanthomas
are rare.
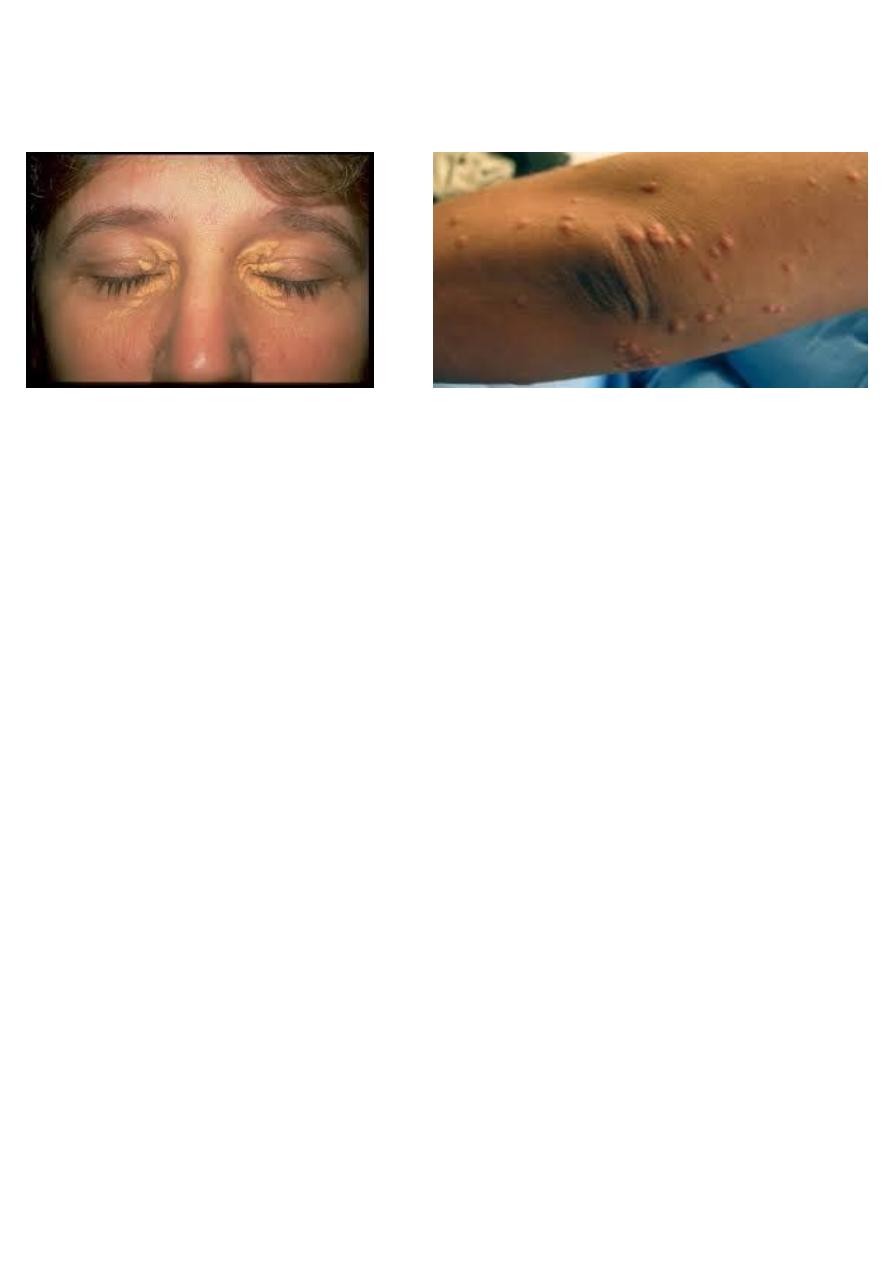
Xanthelasma Eruptive xanthoma
Presentation with the complications of diabetes
Patients with longstanding diabetes are at risk of developing a variety of complications and as
many as 25% of people with type 2 diabetes have evidence of diabetic complications at the time of
diagnosis.
Diabetes may be first suspected when a patient visits an optometrist or podiatrist, or presents
with hypertension or a vascular event such as an acute myocardial infarction or stroke. Blood
glucose should therefore be checked in all patients presenting with such pathology.
Diabetes emergencies
1- Diabetic ketoacidosis
2- Hyperglycaemic hyperosmolar state
3- Hypoglycaemia
Diabetic ketoacidosis
⚫ Diabetic ketoacidosis (DKA) is a medical emergency and remains a serious cause of
morbidity, principally in people with type 1 diabetes. Mortality is low in the UK
(approximately 2%) but remains high in developing countries and among nonhospitalised
patients.
⚫ Mortality in DKA is most commonly caused in children and adolescents by cerebral oedema,
and in adults by hypokalaemia, acute respiratory distress syndrome and comorbid conditions
such as acute myocardial infarction, sepsis or pneumonia.
⚫ DKA is characteristic of type 1 diabetes and is often the presenting problem in newly
diagnosed patients . However , an increasing number of patients presenting with DKA have
underlying type 2 diabetes

In established type 1 diabetes, DKA may be precipitated by
1- an intercurrent illness because of failure to increase insulin dose appropriately to compensate
for the stress response.
2- Sometimes, there is no evidence of a precipitating infection and DKA develops because of
errors in self-management.
Clinical features of diabetic ketoacidosis Symptoms
• Polyuria, thirst
• Weight loss
• Weakness
• Nausea, vomiting
• Leg cramps
• Blurred vision
• Abdominal pain
Signs
• Dehydration
• Hypotension (postural or supine)
• Cold extremities/peripheral cyanosis
• Tachycardia
• Air hunger (Kussmaul breathing)
• Smell of acetone
• Hypothermia
• Delirium, drowsiness, coma (10%)
The diagnositic biochemical features are:
• hyperketonaemia (≥ 3.0 mmol/L) or ketonuria (more than 2+ on standard urine sticks)
• hyperglycaemia (blood glucose ≥ 11.1 mmol/L (approximately 200 mg/dL))
• metabolic acidosis (venous bicarbonate < 15 mmol/L and/ or venous pH < 7.3 (H+ > 50
nmol/L)).
• Abdominal pain and vomiting are sometimes a feature of DKA, particularly in children.
• Serum amylase may be elevated but rarely indicates coexisting pancreatitis.
• In infected patients, pyrexia may not be present initially because of vasodilatation secondary
to acidosis
Investigations
⚫ The following investigations are important but should not delay the institution of
intravenous fluid and insulin replacement:

⚫ •Venous blood: for urea and electrolytes, glucose, bicarbonate and acid–base status
⚫ •Urine or blood analysis for ketones
⚫ •Electrocardiogram (ECG)
⚫ •Infection screen: full blood count, blood and urine culture, C-reactive protein, chest X ray.
Although leucocytosis invariably occurs in DKA, this represents a stress response and does
not necessarily indicate infection.
أفضل الناس"
" أنفعهم للناس