
Dr.Mushtaq Talib Hussein
F.I.B.M.S(Ortho.)- C.A.B.O(Ortho.)
COLLES’ FRACTURE
The injury that Abraham Colles described in 1814 is a transverse fracture of the radius
just above the wrist, with dorsal displacement of the distal fragment. It is the most
common of all fractures in older people, the high incidence being related to the onset of
postmenopausal osteoporosis. Thus the patient is usually an older woman who gives a
history of falling on her outstretched hand.
Force is applied in the length of the forearm with the wrist in extension. The bone
fractures at the corticocancellous junction and the distal fragment collapses into
extension, dorsal displacement, radial tilt and shortening.
Clinical features
We can recognize this fracture (as Colles did long before radiography was invented) by
the ‘dinner-fork’ deformity, with prominence on the back of the wrist and a depression
in front.
Treatment
UNDISPLACED FRACTURES
If the fracture is undisplaced (or only very slightly displaced), a dorsal splint is applied
for a day or two until the swelling has resolved, then the cast is completed.
DISPLACED FRACTURES
Displaced fractures must be reduced under anaesthesia(haematoma block, Bier’s block
or axillary block).
The hand is grasped and traction is applied in the length of the bone (sometimes with
extension of the wrist to disimpact the fragments); the distal fragment is then pushed
into place by pressing on the dorsum while manipulating the wrist into flexion, ulnar
deviation and pronation. The position is then checked by x-ray. If it is satisfactory, a
dorsal plaster slab is applied.
At 7–10 days fresh x-rays are taken; re-displacement is not uncommon and should be
treated,
The fracture unites in about 6 weeks and, even in the absence of radiological
proof of union, the slab may safely be discarded and exercises begun.
IMPACTED OR COMMINUTED COLLES’ FRACTURES
With substantial impaction or comminution in osteoporotic bone, manipulation and
plaster immobilization alone may be insufficient.
In these cases ,surgical intervention is better choice in which an percutaneous k- wire
fixation, locking plate, or cross wrist external fixator can be used to fix the fracture.
Complications
EARLY
Circulatory problems The circulation in the fingers must be checked; the bandage
holding the slab may need to be split or loosened.
Nerve injury Direct injury is rare, but compression of the median nerve in the carpal
tunnel is fairly common.
Reflex sympathetic dystrophy This condition is probably quite common, but
fortunately it seldom progresses to the full-blown picture of Sudeck’s atrophy.

LATE
Malunion Malunion is common, either because reduction was not complete or because
displacement within the plaster was overlooked.
Stiffness Stiffness of the shoulder, elbow and fingers from neglect is a common
complication.
Tendon rupture Rupture of extensor pollicis longus occasionally occurs a few weeks
after an apparently trivial undisplaced fracture of the lower radius.
SMITH’S FRACTURE
Smith (a Dubliner, like Colles) described a similar fracture about 20 years later.
However, in this injury the distal fragment is displaced anteriorly (which is why it is
sometimes called a ‘reversed Colles’). It is caused by a fall on the back of the hand.
The patient presents with a wrist injury, but there is no dinner-fork deformity. Instead,
there is a ‘garden spade’ deformity.
DISTAL FOREARM FRACTURES IN CHILDREN
The distal radius and ulna are among the commonest sites of childhood fractures. The
break may occur through the distal radial physis or in the metaphysis of one or both
bones. Metaphyseal fractures are often incomplete or greenstick.
The usual injury is a fall on the outstretched hand with the wrist in extension; the distal
fragment is forced posteriorly (this is often called a ‘juvenile Colles’ fracture’).
FRACTURED RADIAL STYLOID
This injury is caused by forced radial deviation of the wrist and may occur after a fall, or
when a starting handle ‘kicks back’ – the so-called ‘chauffeur’s fracture‘.The fracture line
is transverse, extending laterally from the articular surface of the radius;
If there is displacement it is reduced, and the wrist is held in ulnar deviation by a plaster
slab round the outer forearm extending from below the elbow to the metacarpal necks.
Failure of perfect reduction need surgical intervention.
BARTON’S FRACTURE
The true Barton’s injury is a volar fracture of the distal radius associated with volar
subluxation of the carpus.(volar type).
a ‘dorsal Barton’s fracture’. Here the line of fracture runs obliquely across the dorsal lip
of the radius and the carpus is carried posteriorly.
CARPAL INJURIES
Fractures and dislocations of the carpal bones are common. They vary greatly in type
and severity. These should never be regarded as isolated injuries; the entire carpus suffers,
and sometimes, long after the fracture has healed, the patient still complains of pain and
weakness in the wrist.
FRACTURED SCAPHOID
Scaphoid fractures account for almost 75 per cent of all carpal fractures although they
are rare in the elderly and in children.
The combination of forced carpal movement and compression, as in a fall on the
dorsiflexed hand, exerts severe stress on the bone and it is liable to fracture.
The blood supply of the scaphoid diminishes proximally. This accounts for the fact that 1
per cent of distal third fractures, 20 per cent of middle third fractures and 40 per cent of
proximal fractures result in non-union or avascular necrosis of the proximal fragment.
Clinical features
The appearance may be deceptively normal, but the astute observer can usually detect
fullness in the anatomical snuffbox; precisely localized tenderness in the same place is
an important diagnostic sign.
Proximal pressure along the axis of the thumb may be painful.
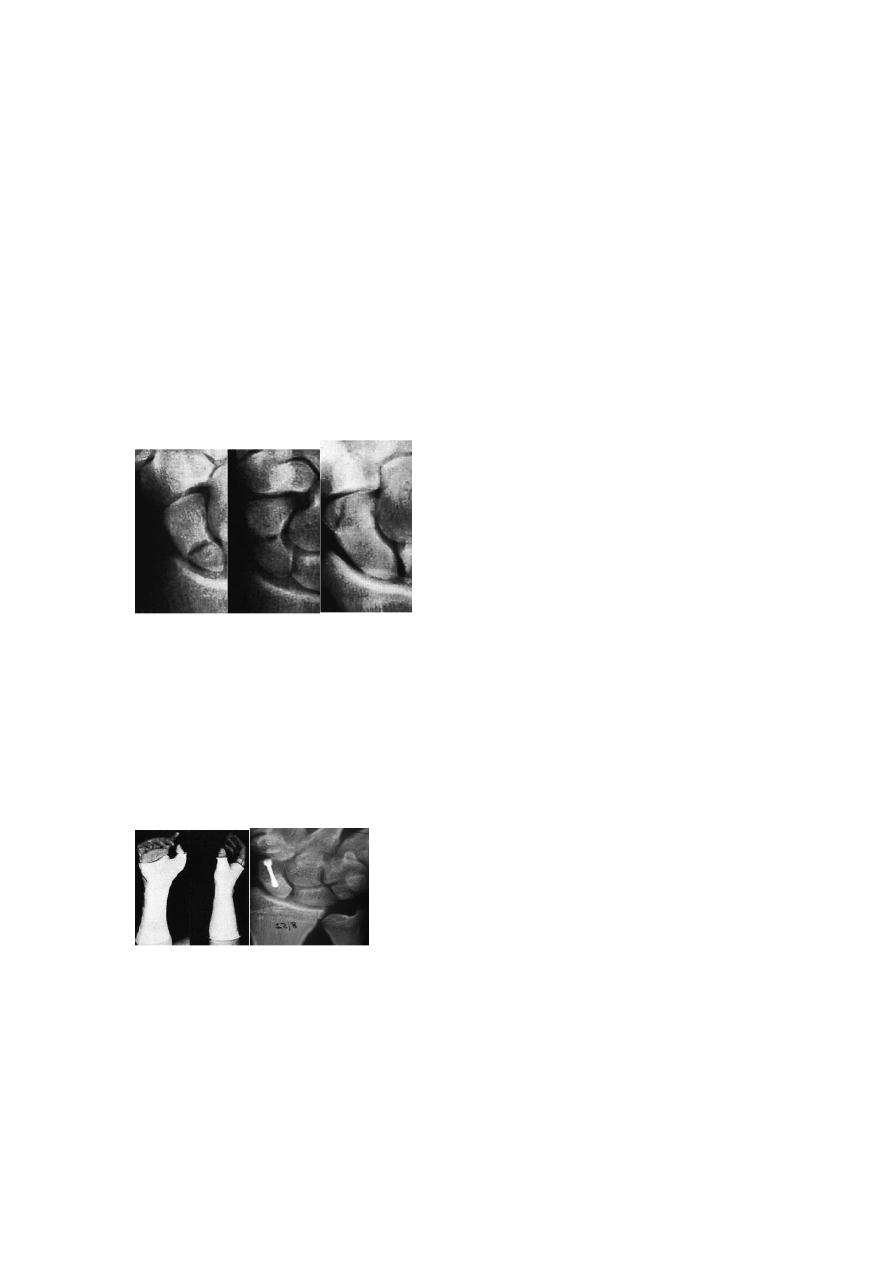
X-ray
Anteroposterior, lateral and oblique views are all essential; often a recent fracture
shows only in the oblique view. Usually the fracture line is transverse, and through the
narrowest part of the bone (waist), but it may be more proximally situated (proximal
pole fracture). Sometimes only the tubercle of the scaphoid is fractured. A few weeks
after the injury the fracture may be more obvious; if union is delayed, cavitation appears
on either side of the break. Old, un-united fractures have ‘hard’ borders, making it seem
as if there is an extra carpal bone. Relative sclerosis of the proximal fragment is
pathognomonic of avascular necrosis.
Proximal waist tubercle
Treatment
Fracture of the scaphoid tubercle needs no splintage and should be treated as a wrist
sprain; a crepe bandage is applied and movement is encouraged.
Undisplaced fractures need no reduction and are treated in plaster; 90 per cent of
waist fractures should heal. The cast is applied from the upper forearm to just short of
the metacarpo-phalangeal joints of the fingers, but incorporating the proximal phalanx
of the thumb.
The wrist is held dorsiflexed and the thumb forwards in the ‘glass-
holding’ position.(8 weeks)
Displaced fractures
can also be treated in plaster, but the outcome is less predictable. It
is better to reduce the fracture openly and to fix it with a compression screw.
Complications
Avascular necrosis The proximal fragment may die, especially with proximal pole
fractures, and then at 2–3 months it appears dense on x-ray.
Non-union By 3 months it may be obvious that the fracture will not unite. Bone grafting
should be attempted, especially in the younger, more vigorous type of patient, because
this probably reduces the chance of later, symptomatic osteoarthritis.
Osteoarthritis Non-union or avascular necrosis may lead to secondary osteoarthritis of
the wrist.

FRACTURES OF OTHER CARPAL BONES
Triquetrum
Avulsion of the dorsal ligaments is not uncommon; analgesics and splintage for a few
days are all that is required.
Hamate
A fracture of the hook of hamate follows a direct blow to the palm of the hand. These
fractures cannot be seen on routine x-rays; a carpal tunnel view, CT or MRI is needed.
Lunate
Fractures of the lunate are rare and follow a hyperextension injury to the wrist. There is a real
risk of nonunion; undisplaced fractures should be immobilized in a cast for 6 weeks; displaced
fractures should be reduced and fixed with a screw.
ULNAR-SIDE WRIST INJURIES
The distal radio-ulnar joint is often injured with a radial fracture; it can also be damaged
in isolation, particularly after hyperpronation. The triangular fibrocartilage complex
(TFCC) can be torn, the ulnar styloid avulsed or the articular surfaces of the ulnocarpal
joint or distal radio-ulnar joint damaged.
There is tenderness over the distal radio-ulnar joint and pain on rotation of the forearm.
The distal ulna may be unstable; the piano-key sign is elicited by holding the patient’s
forearm pronated and pushing sharply forwards on the head of the ulna.
CARPAL DISLOCATIONS, SUBLUXATIONS AND INSTABILITY
The wrist functions as a system of intercalated segments or links, stabilized by the
intercarpal ligaments and the scaphoid which acts as a bridge between the proximal and
distal rows of the carpus. Fractures and dislocations of the carpal bones, or even simple
ligament tears and sprains, may seriously disturb this system so that the links collapse
into one of several well-recognized patterns.
LUNATE AND PERILUNATE DISLOCATIONS
A fall with the hand forced into dorsiflexion may tear the tough ligaments that normally
bind the carpal bones.
SCAPHO-LUNATE DISSOCIATION
A wrist sprain may be followed by persistent pain and tenderness over the dorsum just
distal to Lister’s tubercle.
RADIO-CARPAL DISLOCATION
The most common injuries of this type involve a fracture of the anterior or posterior rim
of the distal radius (Barton’s fracture).
TRIQUETRO-LUNATE DISSOCIATION
A medial sprain followed by weakness of grip and tenderness distal to the head of the
ulna should suggest disruption of the triquetro-lunate ligaments.
MIDCARPAL DISLOCATION
The extrinsic ligaments which bind the proximal to the distal row can rupture (there are,
by definition, no intrinsic ligaments between these two rows). The diagnosis is difficult
but is more readily suggested in those with generalized ligament laxity and a chronic
wrist problem.