• بسم الله الرحمن الرحيم
Objectives
Knowledge of principles of functional neuro anatomy
Review the main functions of nervous system
Knowledge of physiological and pathophysiological principles of neurological examUnderstanding common neurological complaints and their common causes
Knowledge of the common neurological investigation and some of their indicationHow lumbar puncture is done and what is the normal picture of Cerebrospinal fluid.
المنهاج السنوي لمادة العصبية \ المرحلة الخامسةintroduction
Headache and facial pain
Cranial nerve disorders
epilepsy
Stroke and subarachnoid hemorrhage
Parkinson disease and parkinsonism
Movement disorders
Dementia
Inherited ataxias
Multiple sclerosis
Meningitis
Encephalitis and brain abscess
Raised ICP, IIH, SOL
Brain tumors and paraneoplastic syndromes
Peripheral neuropathies
Myopathy
Motor neuron disease
Myasthenia graves
Neurological manifestations of systemic diseases
Spinal cord disorders
Emergency neurology
Introduction to Clinical Neurology
FunctionsCells are:
1-neuron: functional unit2-glia (astrocyte, Oligodendrocyte, Microglia)
The nervous system works through1-the generation of an action potential
2-the conduction of an action potential
FUNCTIONAL ANATOMY OF THE NERVOUS SYSTEM:
NS = CNS + PNS
CNS = BRAIN, AND SPINAL CORD
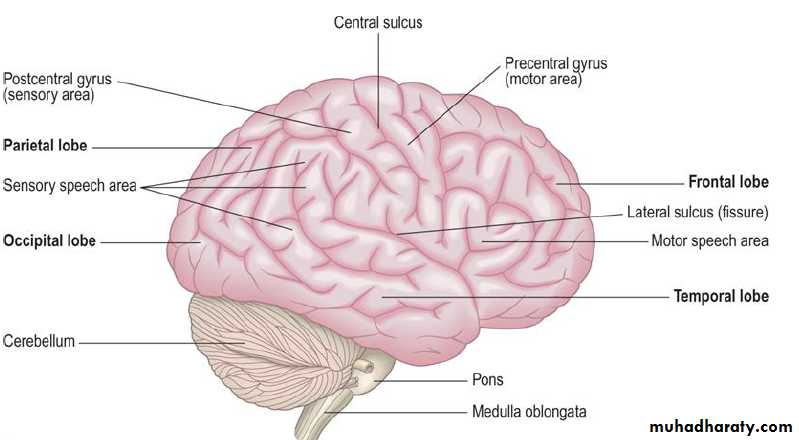
BRAIN= cerebrum + brainstem + cerebellum
CEREBRUM = dominant + non-dominant hemispheres
(dominant = language presentation )
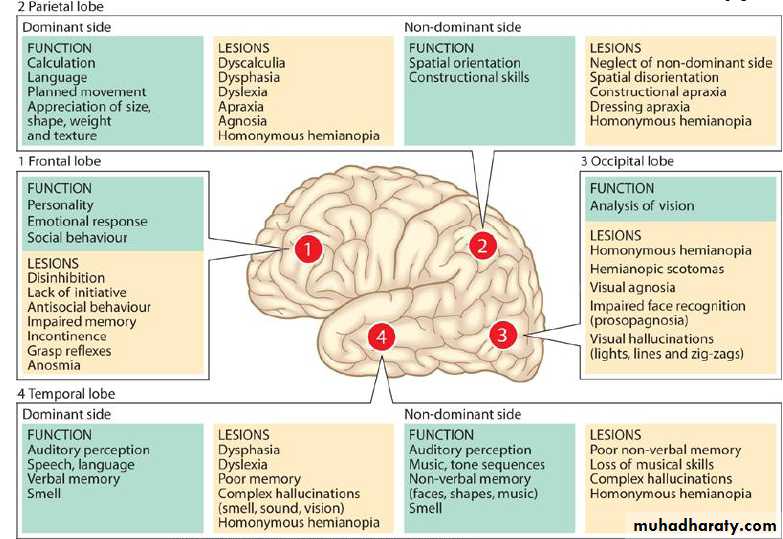
Each hemisphere= 4 functional lobes
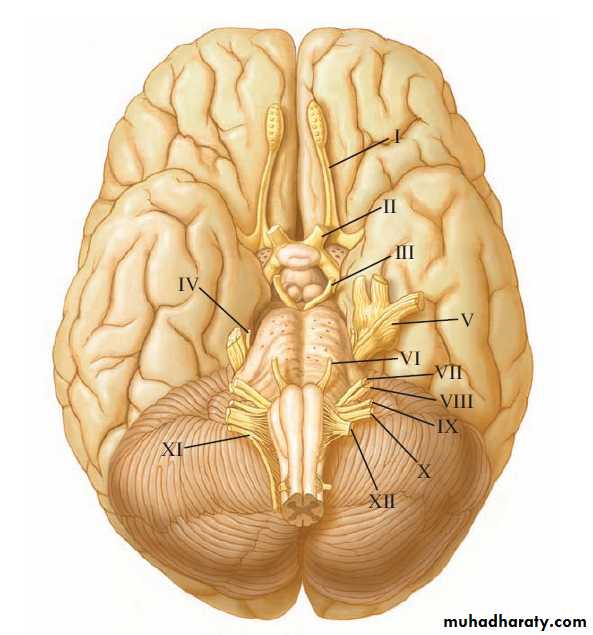
BRAINSTEM= cranial nerve nuclei, RAS, autonomic functions.
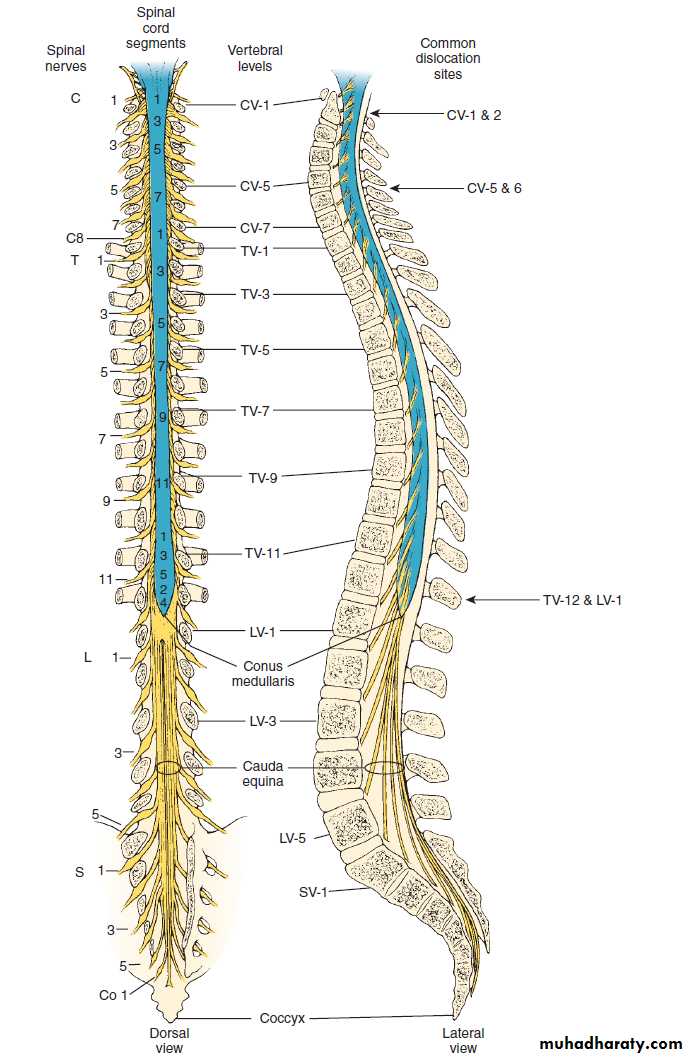
Spinal cord= pathways+sensory+motor neurons
It is divided into8 Cervical segments
12 thoracic
5 lumbar
5 sacral
1 coccygeal
PNS:
Nerve roots, peripheral nerves, NM junction, muscles.CLINICAL SYSTEMS AND THIER DISORDERS
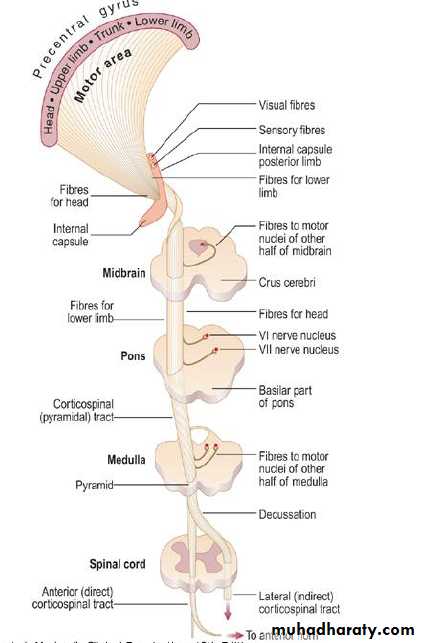
A-Motor system:1- pyramidal system: UMN LMN
2-extrapyramidal
3-cerebellar system
Types of limbs weakness• Pyramidal weakness
• Proximal weakness• Distal weakness
• Segmental weakness
signs
UMNLMN
Extrapyramidal
cerebellar
wasting
+/-
++
none
none
fasciculation
_
+
_
_
tone
spastic
Flaccid
Rigidity
Normal/reduced
• Reflexes
Increased
Reduced/absent
Normal
Normal
• Plantar response
Extensor
Flexor
Flexor
Flexor
• Coordination
Reduced by weakness
Reduced by weakness
Normal
Impaired
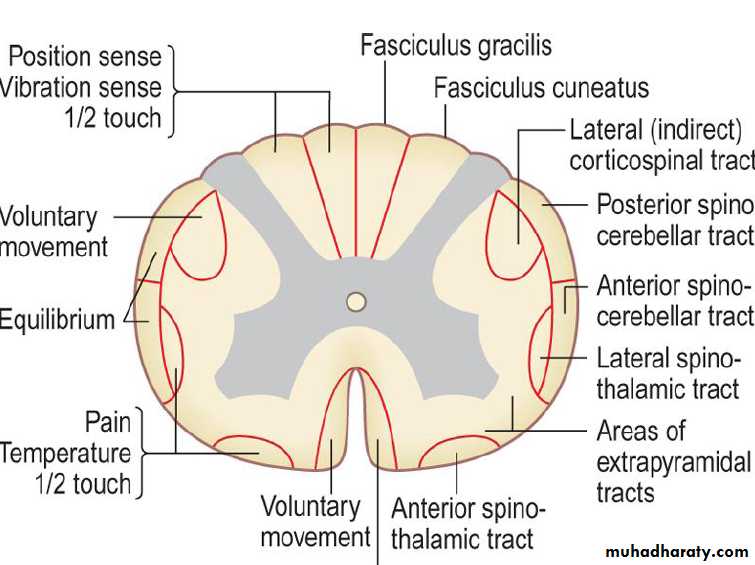
Sensory system
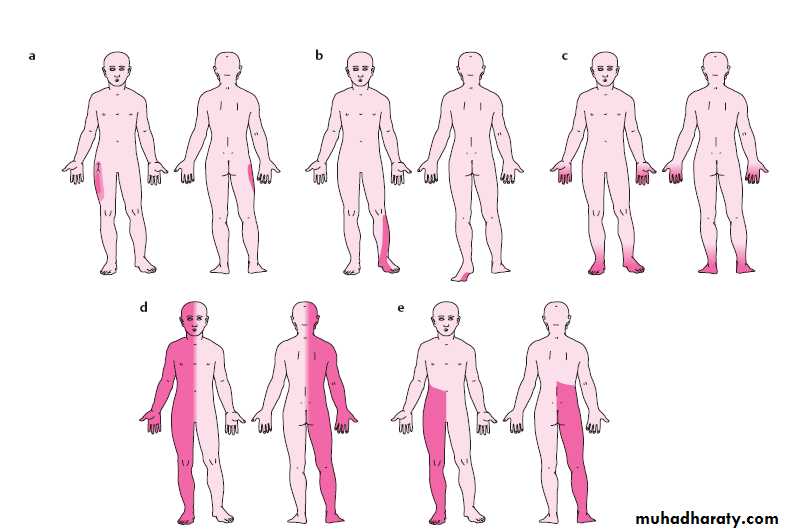
Lesion produces either the negative sensation of numbness or positive symptoms.Sensory impairment distribution could be:
• 1-Hemianasthesia = thalamic lesion2-Glove-stock sensory impairment = peripheral neuropathy
3-Sensory level = transverse myelopathy
4-Segmental = root lesion
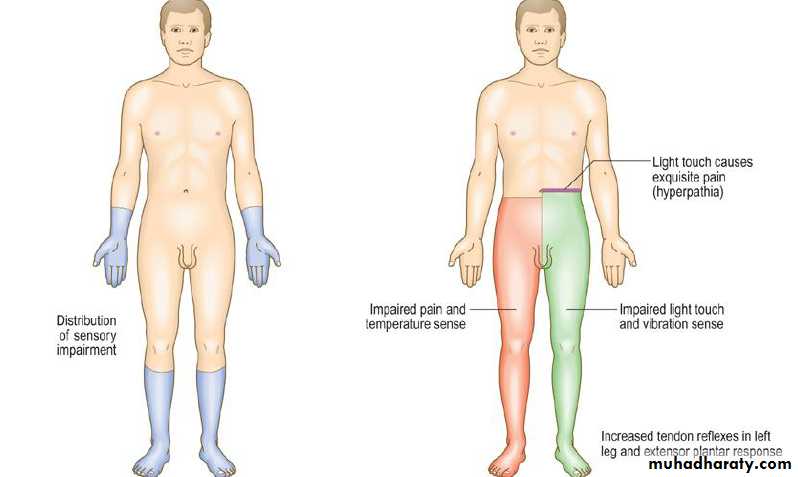
5-Unilateral cord lesion (Brown-Séquard syndrome)= hemisection of spinal cord
6-Cape distribution(central cord syndrome)= syringomyelia
7-Dissociated sensory loss = anterior spinal artery stroke

SPEECH AND LANGUAGE DISTURBANCE
Speech is the process of articulation.Pathway is cerebral cortex-brainstem-cranial nerves(mainly IX, X, XII,VII)-bulbar and tongue muscles.
1-Dysphonia vocal cord disorders
2-Dysartheria spastic speech, nasal speech, monotonus speech.
Language is the art of communication between people.
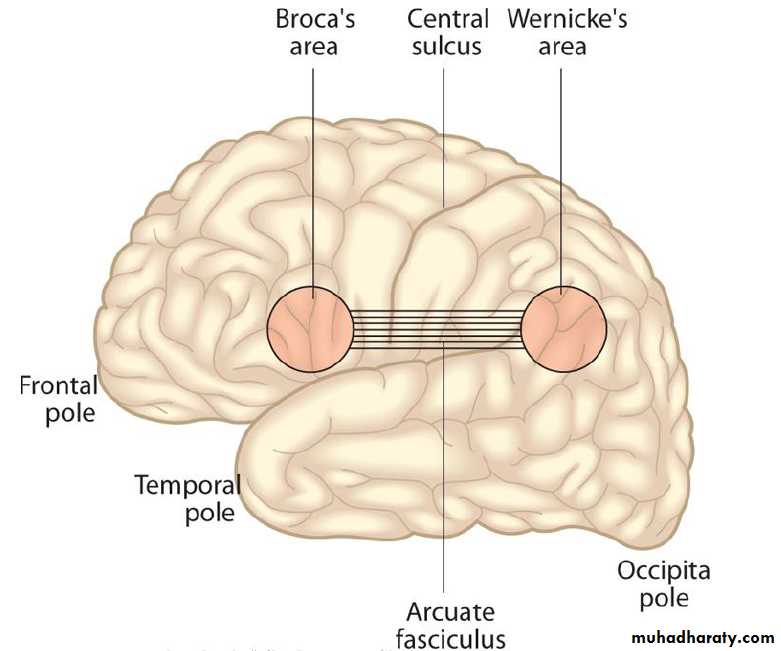
Types of aphasia: mainly divided into fluent and non-fluent
1- Expressive (Broca) aphasia
2-Receptive (Wernicke) aphasia
3-Conduction aphasia
4-Global aphasia
VISUAL DISTURBANCE
Positive symptoms, and negative symptoms.Visual loss is divided into sudden v gradual or transient v permanent or unilateral v bilateral.
Sudden visual loss:
1-Migraine visual aura2- Transient retinal ischemia (amaurosis fugax).
3-optic neuritis
4-Retinal artery occlusion
5-Anterior ischemic optic neuropathy.
6-Retinal vein occlusion
7-Traumatic optic neuropathy
Gradual visual loss
1-Cataract
2-Glaucoma
3-Age-related macular degeneration
4-Optic nerve or chiasm compression by tumours
Visual field defects
Disorders of the pupilPLR is the result of a combination sympathetic and parasympathetic activity.
Causes of dilated pupil
1- 3rd nerve palsy
2- Adrenergic drops
3-Anticholinergic drops
4-Adie pupil
Causes of small pupil
1-Horner's syndrome2-Argyll Robertson pupil
3-cholinergic drugs
4- opiate drugs
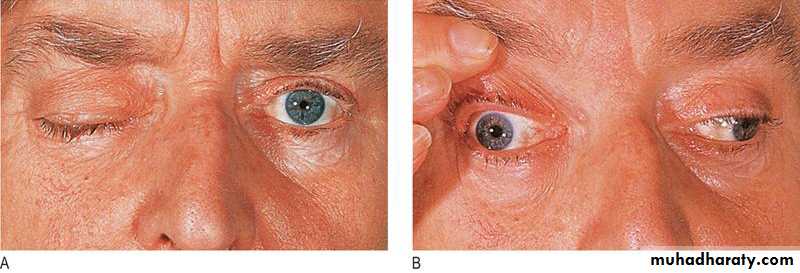
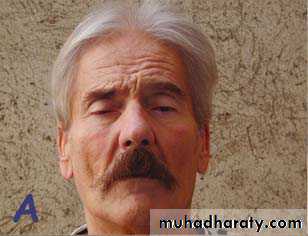
Ptosis: is drooping of the upper eyelid, may be complete or partial.
1-neurogenic : 3rd nerve palsy, Horner's syndrome.
2- myogenic :myotonic dystrophy, hypothyroidism.3-Neuromuscular junction: Myasthenia gravis
4-mechanical :Eyelid tumour, trauma, degenerative.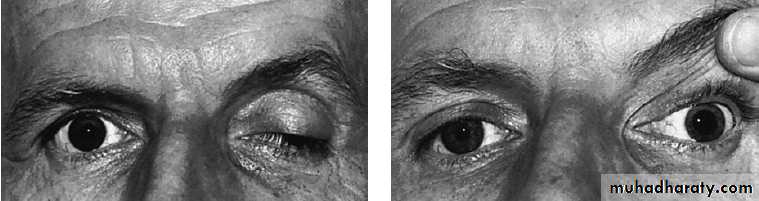


Optic disc swelling :
There are several causes of swelling of the optic discA- Raised intracranial pressure ( SOL, IIH) called papilloedema
B- Obstruction of ocular venous drainage
C-Systemic disorders affecting retinal vessels ( HT,hypercapnea)D- others (Demyelination , Infiltration of optic disc)
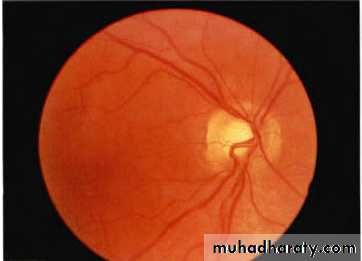
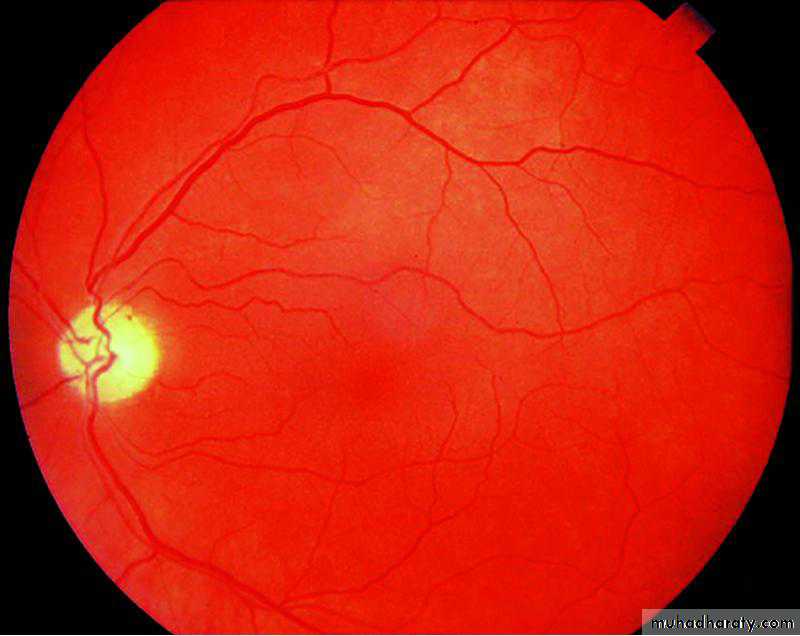
Normal fundus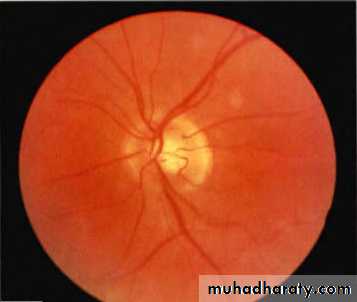
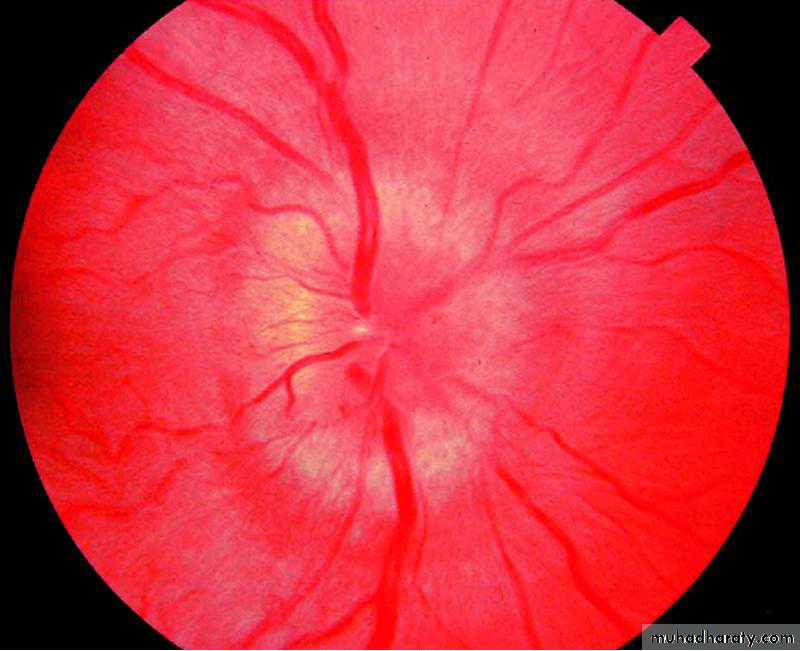
PAPILLEDEMA
Optic atrophyLoss of nerve fibres causes the optic disc to appear pale, as the choroid becomes visible.
1-previous optic neuritis
2-ischaemic damage,
3-long-standing papilloedema,
4-optic nerve compression
5-trauma
6-degenerative conditions (e.g. Friedreich's ataxia)
optic atrophy
Nystagmus:
Nystagmus is an involuntary oscillation of the eyes that is often rhythmical, with both eyes moving synchronously.
1-pendular nystagmus :Oscillations occurring at the same speed and over the same range about a central point .
2-jerky nystagmus : slow & fast phases.
The direction of the fast phase is usually designated as the direction of the nystagmus because it is easier to see.Nystagmus is seen as a physiological phenomenon, however; There are, however, many different causes of pathological nystagmus, the most common being disorders of the vestibular system (peripheral and central components) and brain-stem/cerebellar lesions.
Vertigo
defined as an abnormal perception of movement of the environment or self(Sense of spinning)
Hx. and examination are vital to differentiate between central and peripheral vertigo
Central vertigo occurs due to brainstem and/or cerebellar pathology
Central vertigo is usually persistent and associated with brainstem signs and symptoms.
Causes include stroke, encephalitis, demyelinating diseases, tumors, etc.
Peripheral vertigo occurs due to imbalance between labyrinths
Peripheral vertigo is usually paroxysmal and more severe and disabiling than central vertigo
Causes include benign paroxysmal positional vertigo, vestibular neuritis, Meniere‘s disease, and vestibular migraine.
Fainting (funny turn):
Episodic lost or altered consciousnessIt needs elucidation (What does the patient mean?)
Syncope versus seizureSyncope : brief alteration of consciousness due to temporary loss of blood supply to the whole brain.
Symptoms may include darkening of vision, distal tingling, nausea and sweating. The patient recovers quickly.
History of neurological problems
several important points should be included1- clarification of patient symptom
2- Onset
a-sudden hemorrhage
b-acute ischemic
c- subacute infection/ inflammatoryd-chronic or insidious neoplastic/ degenerative/ hereditary
3- course of illnessimproving , deteriorating, stationary, paroxysmal (relapsing-remitting)
4- associated features
headache, vision, continence, convulsion, consciousness,Weakness, sensory loss or impaired sensation, swallowing
INVESTIGATION OF NEUROLOGICAL DISEASE
CLINICAL NEUROPHYSIOLOGY includes1- EEG: recording of electrical activity over the brain. The most important use of EEG is in the management of epilepsy.
2-NCS&EMG
NEUROIMAGINGX-rays (plain X-rays, computed tomography (CT), myelography and angiography), magnetic resonance (MR imaging-MRI, or MR angiography-MRA), ultrasound (Doppler imaging of blood vessels), and radioisotopes (single photon emission computed tomography-SPECT, and positron emission tomography-PET).
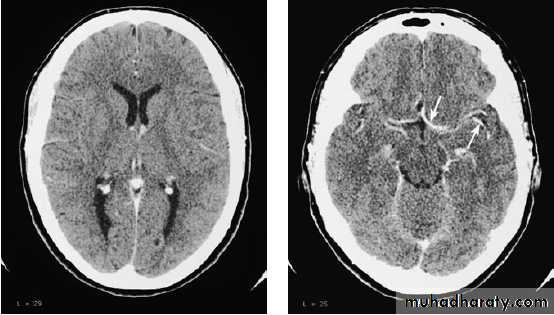
A- CT scan


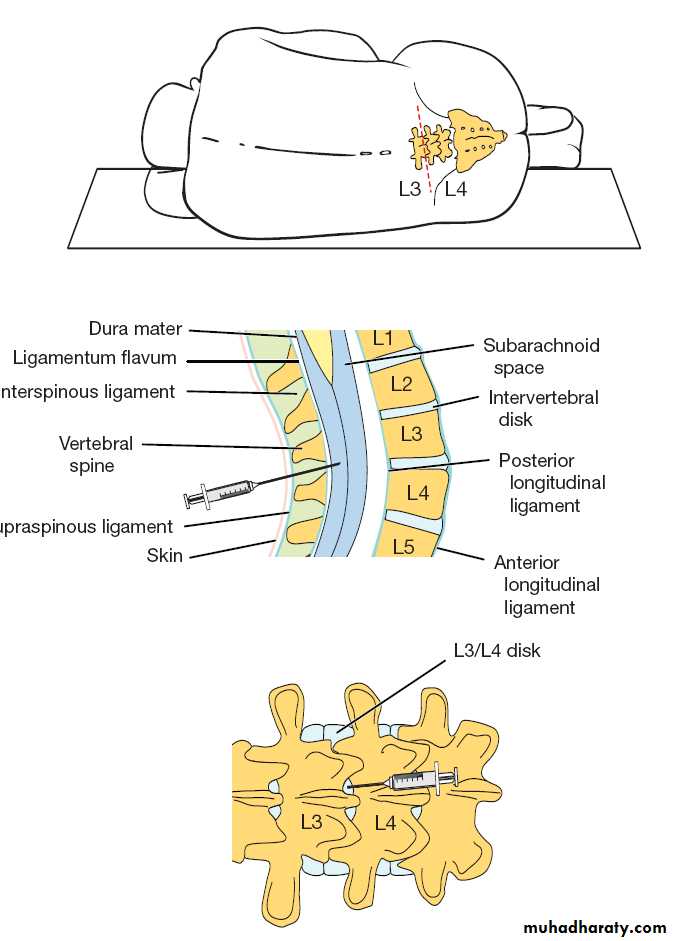
CEREBROSPINAL FLUID ANALYSIS AND LUMBAR PUNCTURE
Indications1- suspected CNS infection
2-intrathecal therapy
3-CSF pressure measure
4-part of the procedure of myelography
5- therapeutic CSF aspirate
Lumbar puncture should not be performed in
1- known or suspected intracranial or spinal mass because of the potential for herniation and neurologic compromise with a shift in intracranial pressure.
2- overlying skin infection
3- on anticoagulant
• PRESSURE
• 50-180 mm water• colour
• clear
• RBC
• 0-4
• WBC
• 0-4
• GLUCOSE
• <60% OF BLOOD LEVEL
• PROTIEN
• 45mg/100ml
• Microbiology
• sterile
NORMAL CSF PARAMETERS
