Injuries of the spine
Spinal injuries carry a double threat: damage to the vertebral column and damage to the
neural tissues. Therefore it is important to establish whether the injury is stable or unstable
and treating it as unstable until proved otherwise.
*Stable injury; is one in which the vertebral components will not be displaced by normal
movements; if the neural elements are undamaged, there is little or no risk of them
becoming damaged.
*An unstable injury; is one in which there is a significant risk of displacement and
consequent damage to the neural tissues.
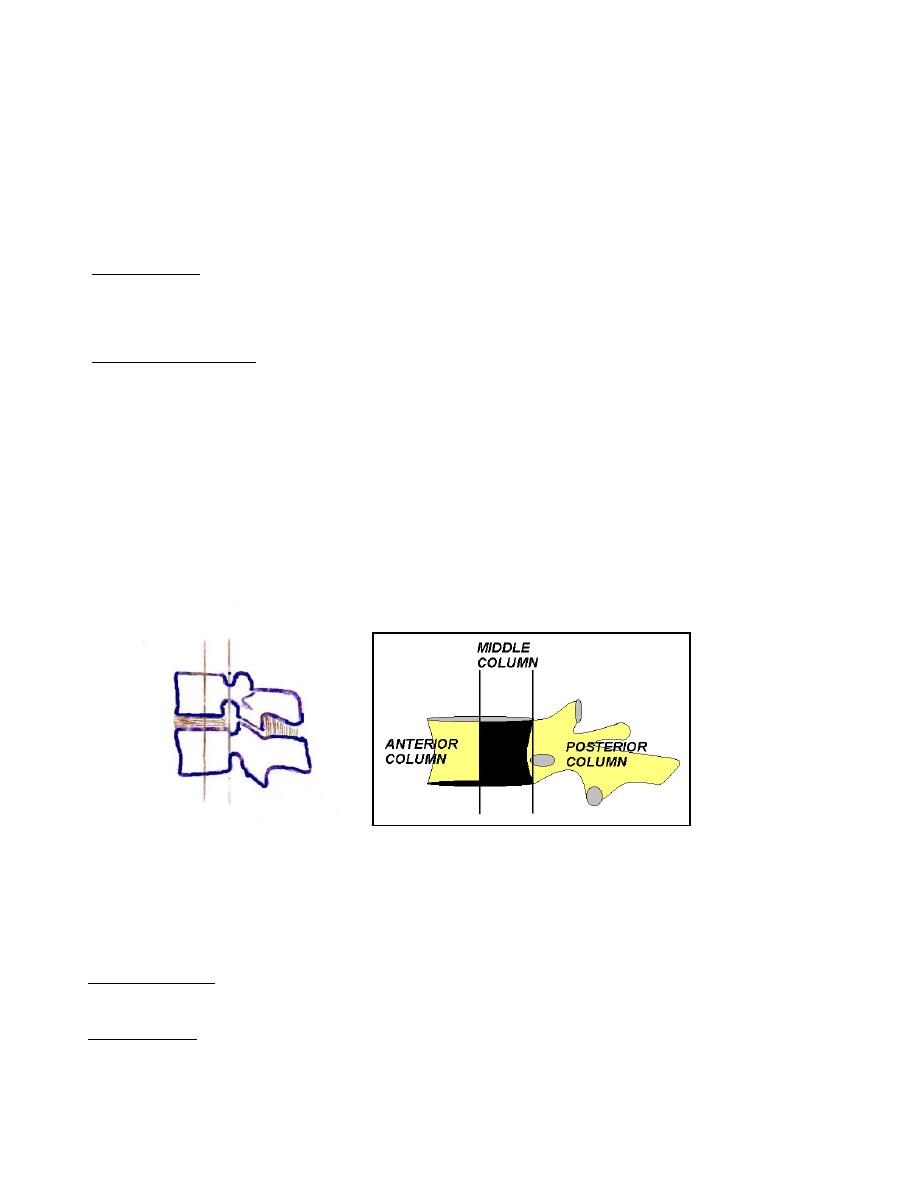
In assessing the stability of the spine, the spine is divided into three structural elements:
• The posterior osseoligamentous complex (posterior column) consisting of the pedicles,
facet joints, posterior bony arch, interspinous and supraspinous ligaments.
• The middle column consisting of the posterior half of the vertebral body, the posterior
part of the intervertebral disc and posterior longitudinal ligament.
• The anterior column composed of the anterior half of the vertebral body, the anterior
part of intervertebral disc and the anterior longitudinal ligament.
All fractures involving the middle column and at least one other column should be
regarded as unstable.
Mechanism of injury
1. Traction injury caused by resisted muscle contraction leading to avulsion of transverse
process in the lumbar spine and the spinous process in the cervical spine.
2. Direct injury caused by penetrating injury to the spine from knives other sharp objects.
3. Indirect injury this is the most common cause of spinal damage which typically occurs
in a fall from height and in road traffic accident, it caused by a variety of forces: axial
compression, flexion, extension, flexion-rotation, flexion-distraction, shear.
Early management
By resuscitation protocol (A, B, C)
A: air way with cervical spine control.
B: Breathing with adequate ventilation and oxygenation.
C: circulation and hemorrhage control.
This also helps to prevent secondary spinal cord injury. And because spinal injury
should be suspected in every patient with severe trauma, the spine should be
immobilized during the resuscitation;
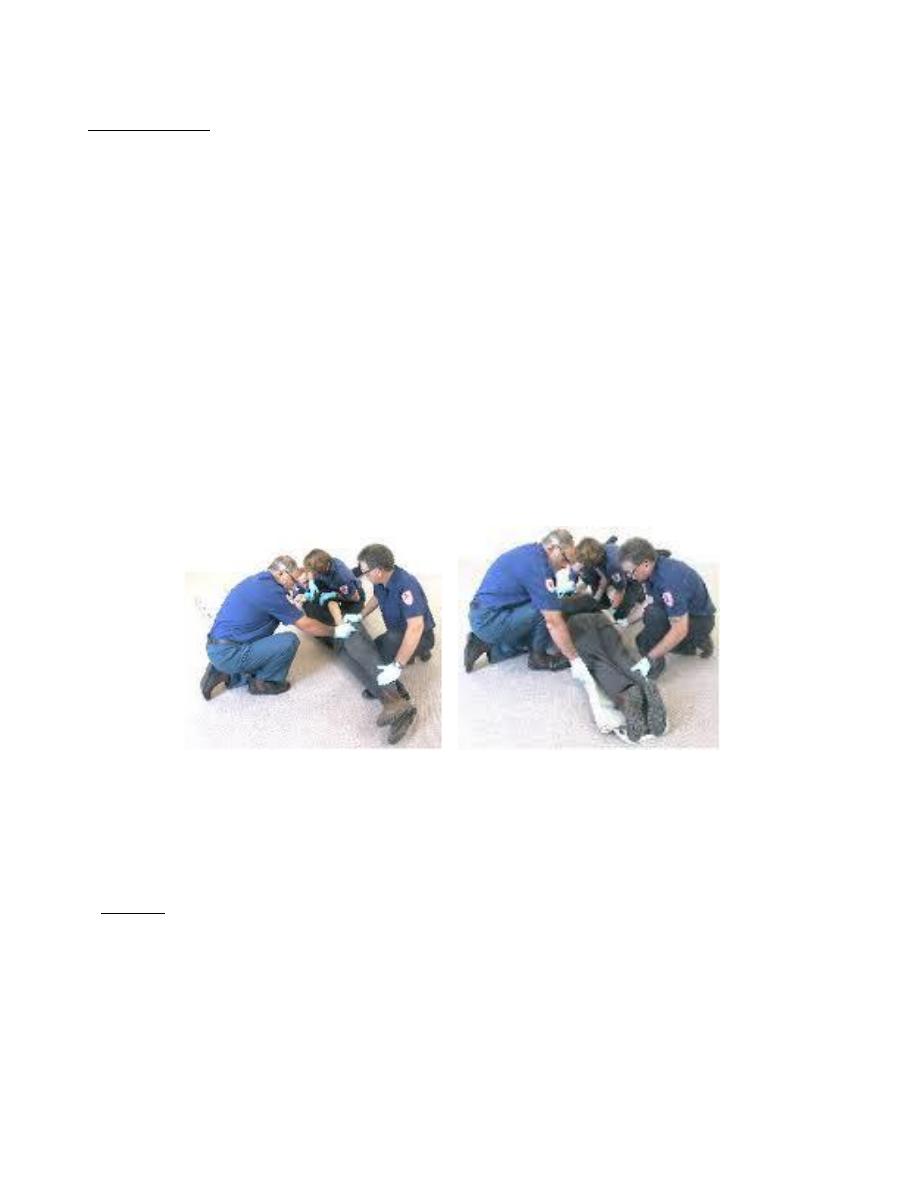
*for cervical spine either by in-line immobilization (the head and neck are supported
in the neutral position) or by quadruple immobilization (by using a backboard,
sandbags, a forehead tape and a semi-rigid collar).
In-line immobilization
*for thoracolumbar spine by scoop stretcher and spinal board.
Diagnosis
• History: every patient with a blunt injury above the clavicle, a head injury, a loss of
consciousness, neck pain and stiffness following trauma should be considered to have
cervical spine injury until proven otherwise.
Every patient who involve in a fall from height, high-speed deceleration accident or
with back pain following trauma should be considered to have a thoracolumbar spine
injury. Any neurological symptoms in the limbs should raise the possibility of spinal
injury.
• Examination:
1. Neck; look for any bruises in the head and face, any deformity or bruises or
penetrating injury in the neck. Palpate the neck for any tenderness or increased space
between spinous processes.
2. Back; look for any deformity, haematoma, bruises and penetrating injury. Palpate for
any tenderness or increased space between spinous processes.
3. Shock ; three types of shock may occur in patient with spinal injury:
*Hypovolaemic shock, characterized by tachycardia and hypotension *Neurogenic
shock, result from loss of sympathetic innervations to the heart and blood vessels
leading to hypotension, bradycardia and paralysis.
*Spinal shock, result from temporarily loss of spinal cord function following injury
characterized by flaccid paralysis and loss of reflexes and sensation.
4. Neurological examination.
• Imaging
X-ray: AP view including open mouth view, lateral and oblique views
CT: scan sees the full extent of the fracture
MRI: show any disc, cord and soft tissue damage.
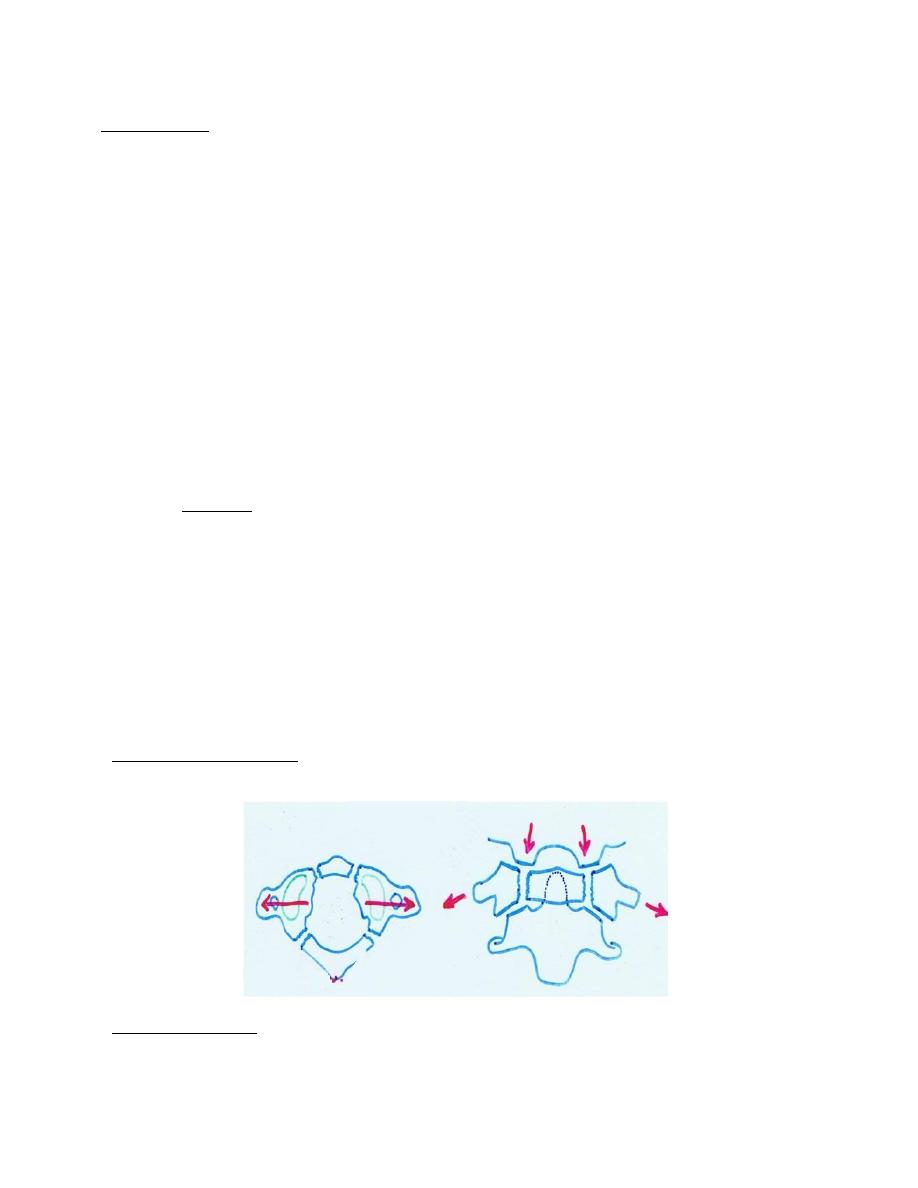
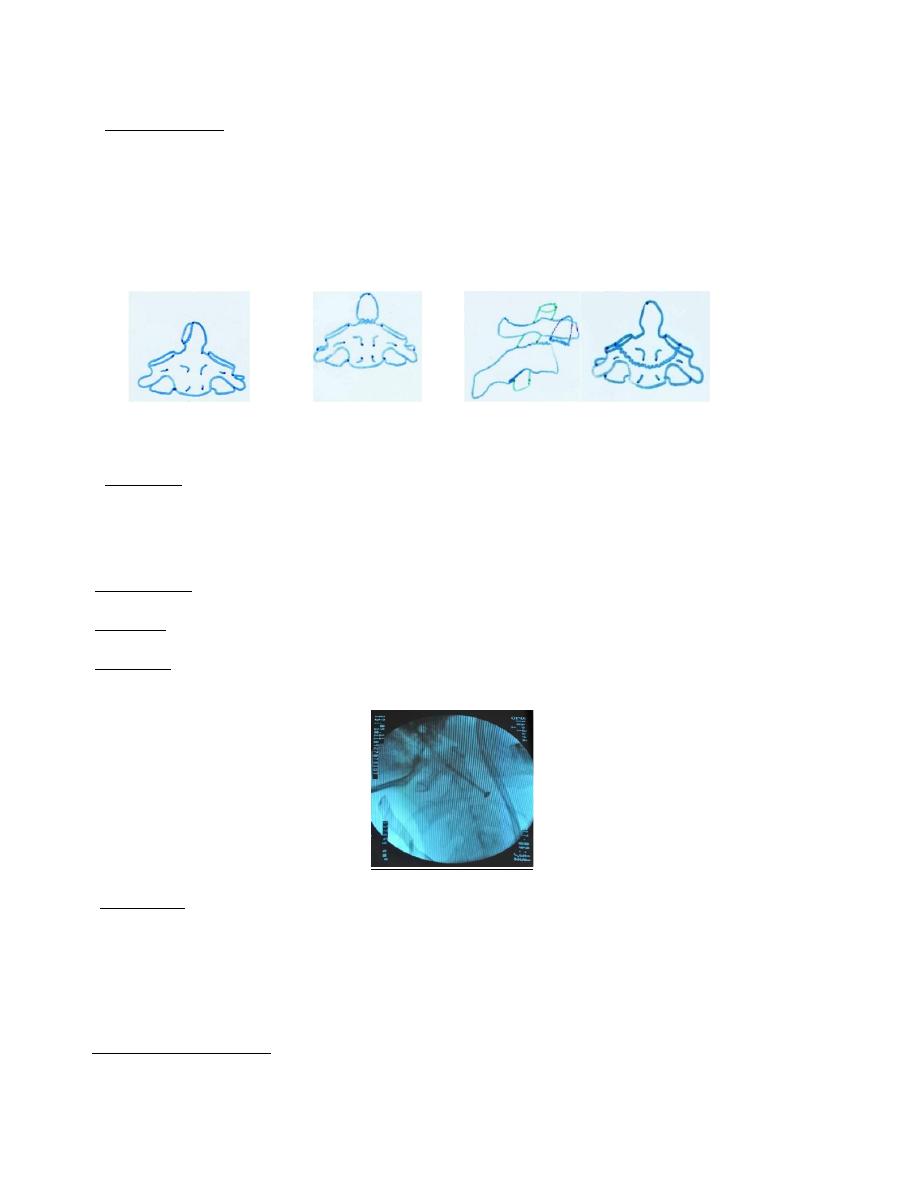
C1 Fracture (Jefferson’s fracture):
It is burst fracture of C1 ring
*Mechanism of injury: sudden severe load on the top of the head leading to
compression injury as in diving in shallow water.
*Clinical features: severe neck pain, stiffness, patient support his neck with his
hands, neck tenderness and usually no neurological damage.
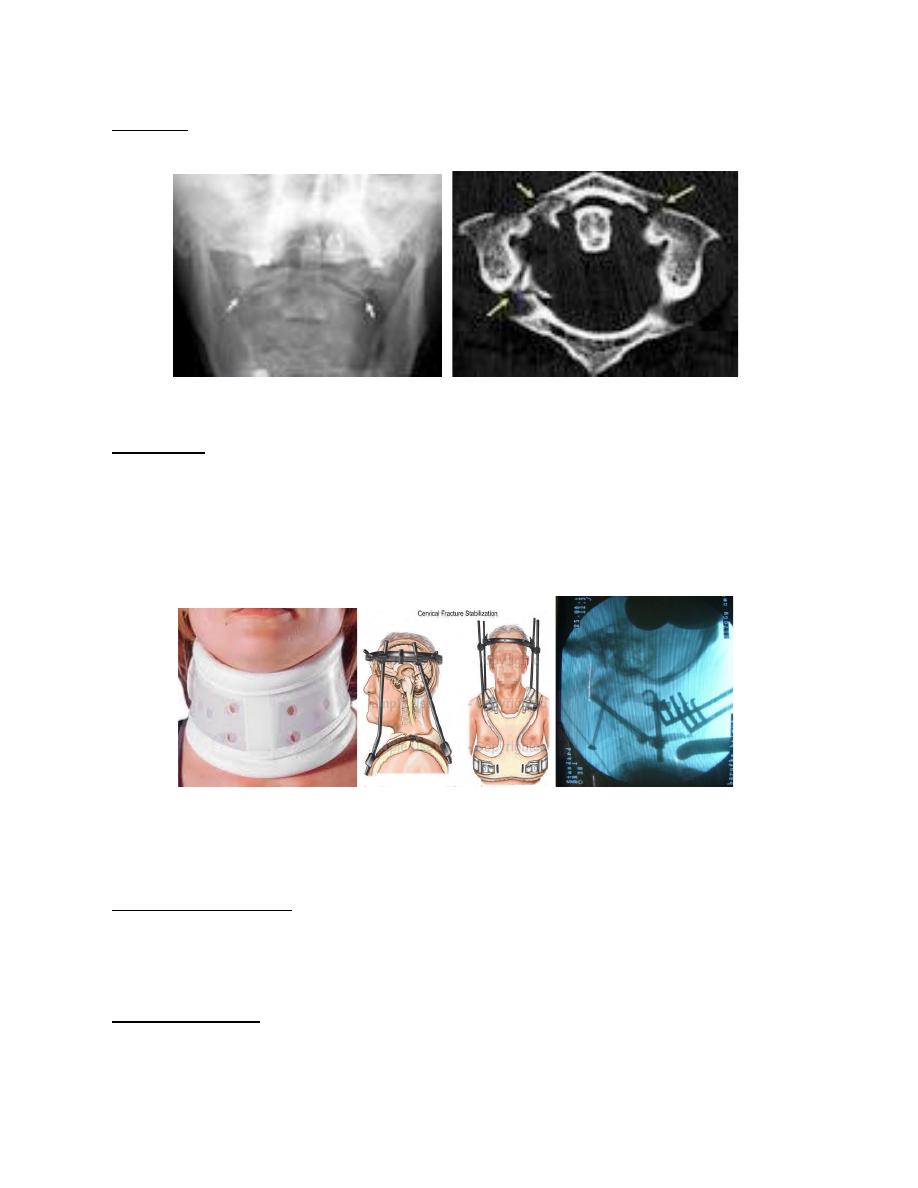
*Imaging: x-ray mainly open mouth and CT scan reveal the fracture which could be
undisplaced (stable) or displaced (unstable).
Open mouth view
*Treatment:
If the fracture undisplaced (stable) patient wear semi rigid collar or halo-vest until
the fracture unites.
If the fracture displaced then halo-vest for 6 weeks, if there is persistent instability
then a posterior C1/C2 arthrodesis.
Semi rigid collar halo-vest C1/C2 arthrodesis
Odontoid fracture (C2)
*Mechanism of injury: In young adult occur as flexion injury after high-velocity
accident, in elderly Osteoporotic people as hyperextension injury after low-energy
accident.A displaced fracture is a fracture-dislocation of atlanto-axial joint in which
the atlas is shifted forward or backward, taking the odontoid process with it.
*Clinical features: neck pain and stiffness from muscle spasm, neurological
symptoms occur in 20% of cases,
*classification:
• Type I-avulsion # of the tip of the odontoid process due to traction by the alar
ligaments, the # is stable and unites without difficulty.
• Type II-A # at the junction of the odontoid process and the body of the axis, this is
the most common &the most dangerous type, the # is unstable and prone to non-union.
• Type III- # through the body of the axis the # is stable & unites with immobilization.
Type I type II type II type III
*Imaging:
X-ray including AP &lat. Views, CT& tomography are helpful to show the full extent
of the # and MRI will show the neurological injury.
*Treatment:
Type I # need immobilization in a rigid collar until discomfort subside.
Type II # If undisplaced need halo-vest .Displaced # need reduction by traction &then
held by either operative fixation or by halo-vest immobilization.
Type III # if undisplaced need halo-vest .Displaced # need reduction by traction then
held by halo-vest immobilization.
Fractured pedicle(s) of C2 (Hangman’s fracture)
It is # of pedicle of C2 (axis) and damage of C1\C2 disc
*Mechanism of injury:
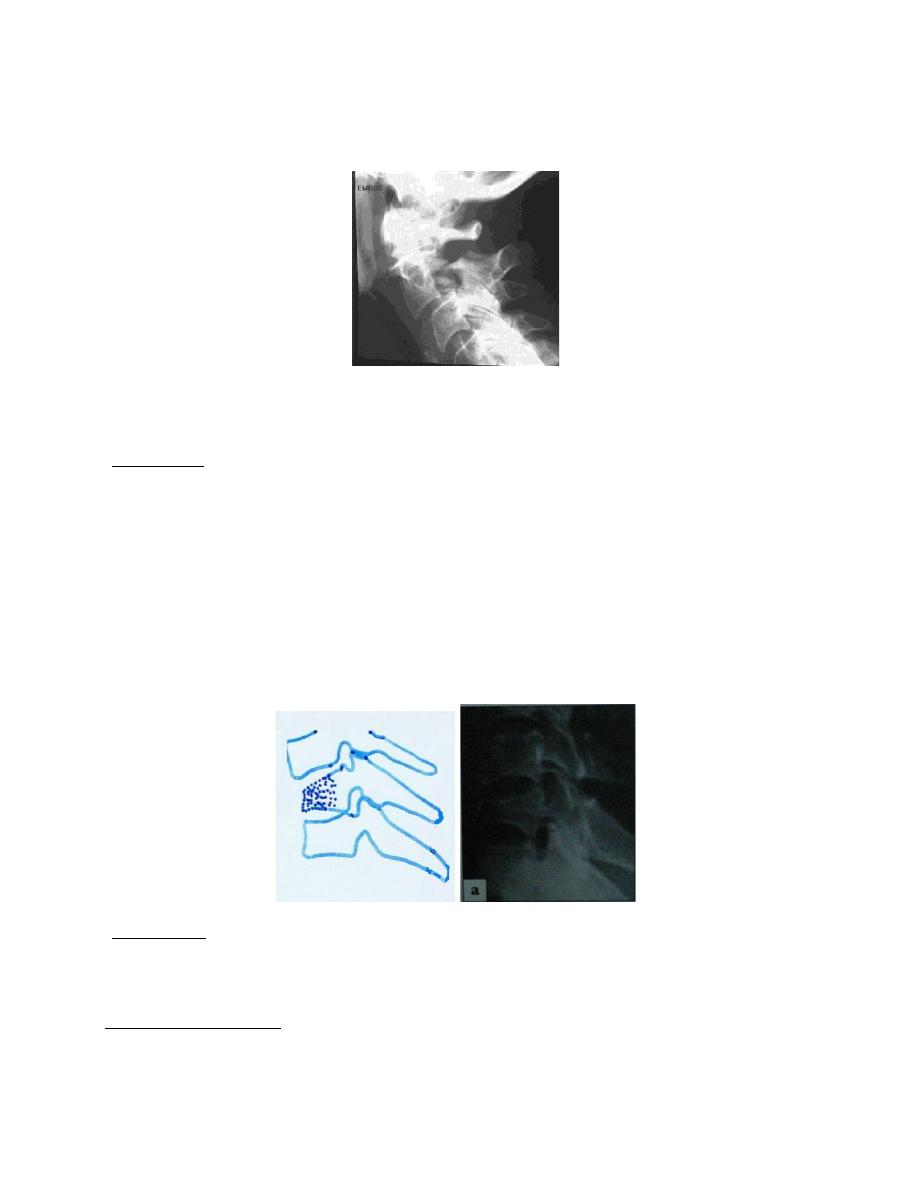
Hyperextension with distraction, in civilian injuries the mechanism involve varying
degrees of extension, compression and flexion.
The # is potentially unstable but neurological damage is unusual because the # of the
posterior arch tend to decompress the spinal cord.
*Treatment:
Undisplaced # which is stable treated in a semi-rigid collar or halo-vest for 12 weeks.
Displaced # needs either closed reduction with halo-vest or, if this fails, open
reduction &internal fixation.
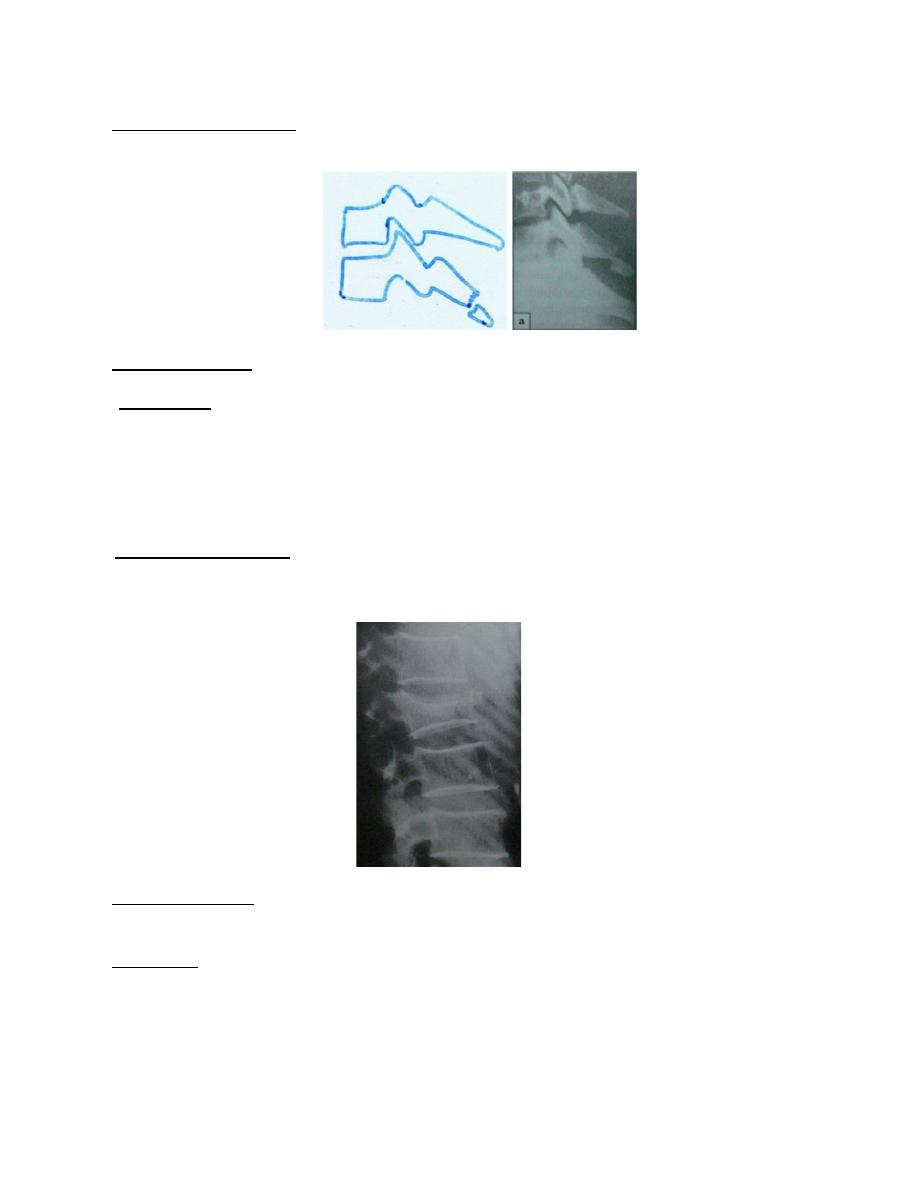
Wedge compression #
*Mechanism of injury: it is caused by pure flexion injury results in a wedge
compression # of the anterior part of vertebral body, the middle and posterior column
remain intact therefore the injury is stable.
*Treatment: Soft collar for few weeks.
Posterior ligament injury
*Mechanism of injury : It is caused by sudden flexion of mid-cervical spine leading
to damage to posterior ligament complex (the interspinous ligament ,facet capsule and

supraspinous ligament ) the upper vertebra tilt forwards on the one below ,opening up
the interspinous space posteriorly.
*Clinical features: neck pain and localized tenderness posteriorly.
*X-ray: reveals increased gap between the adjacent spines, but if the neck held in
extension this gap can be missed, so it is advisable to obtain a lateral view with the
neck in the neutral position.
If the angulation of the vertebral body with its neighbor exceed 11 degrees, if there
is anterior translation of one vertebral body upon the other of more than 3.5 mm or if
the facets are fractured or displaced then the injury is unstable.
*Treatment: Stable injury treated by semi-rigid collar for 6 weeks, if the injury is
unstable then posterior fixation and fusion.
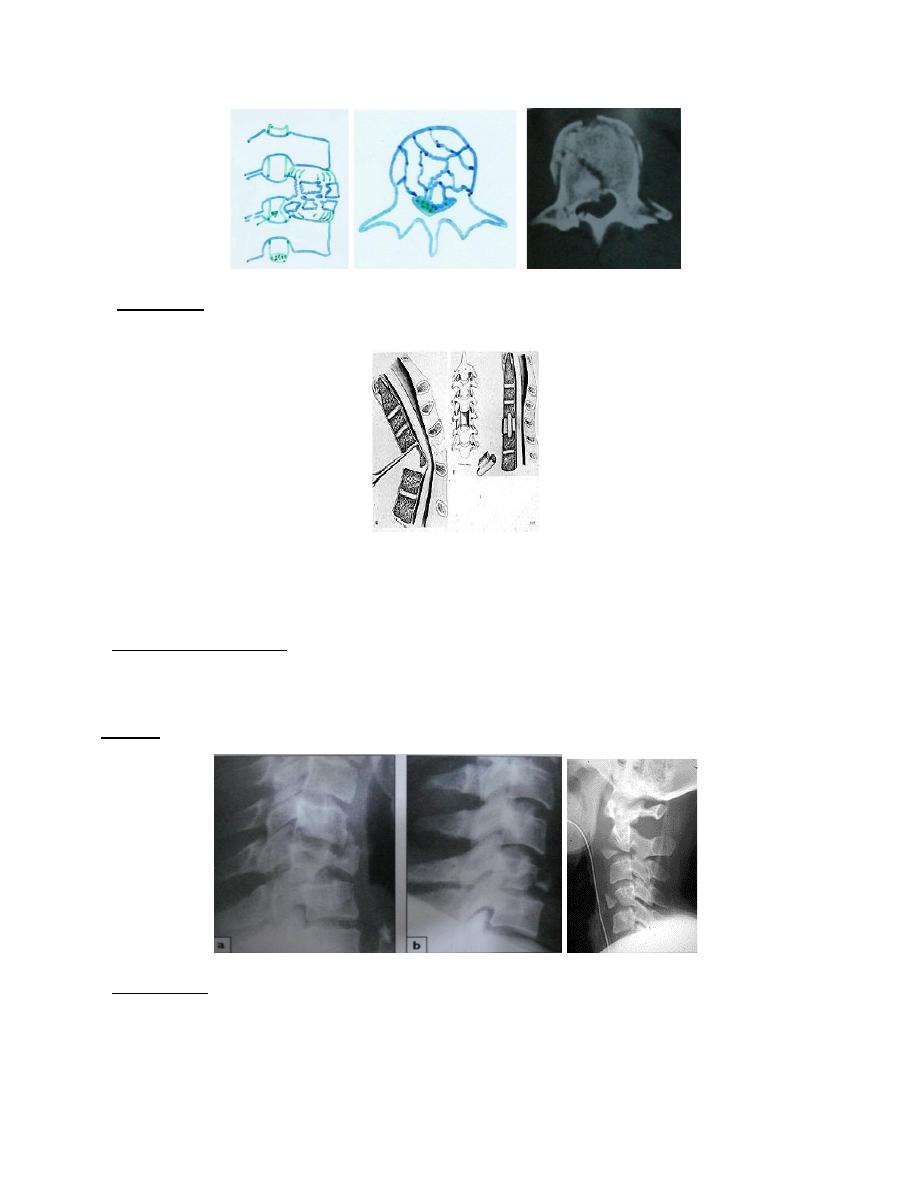
Burst fracture
*Mechanism of injury: axial compression of cervical spine, usually in diving or
athletic accident. Neurological injury is common.
*X-ray: show a comminuted fracture of the vertebral body including middle column.
CT scan: may reveal retropulsion of large bony fragment into the spinal canal.
*Treatment: If there is no neurological deficit, the injury is treated by immobilization
in a halo-vest. If there is any neurological deficit then urgent anterior decompression.
Anterior decompression
Tear –drop fracture
*Mechanism of injury: caused by combined axial compression & flexion, an antero-
inferior fragment of vertebral body is sheared off. The middle & posterior column
may be damaged making it a very unstable injury.
*X-ray: may show that the greater part of vertebral body is displaced posteriorly.
*MRI & CT: will show the full extent of the # and any encroachment on the cord.
*Treatment: If there is no damage of the middle & posterior column, the injury is
stable & can be treated by semi-rigid collar or halo-vest. But if there is damage of the
middle & posterior column the injury should be managed by anterior & posterior
stabilization.
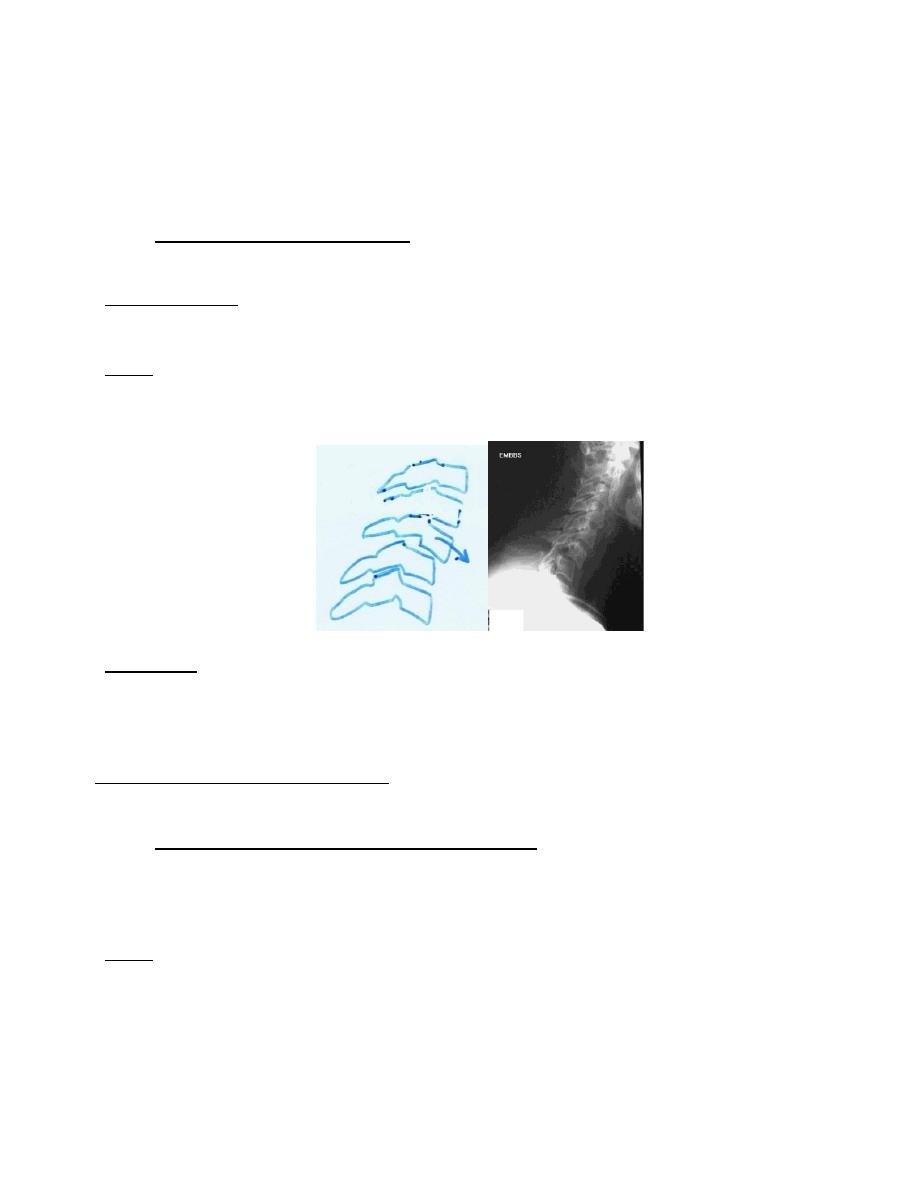
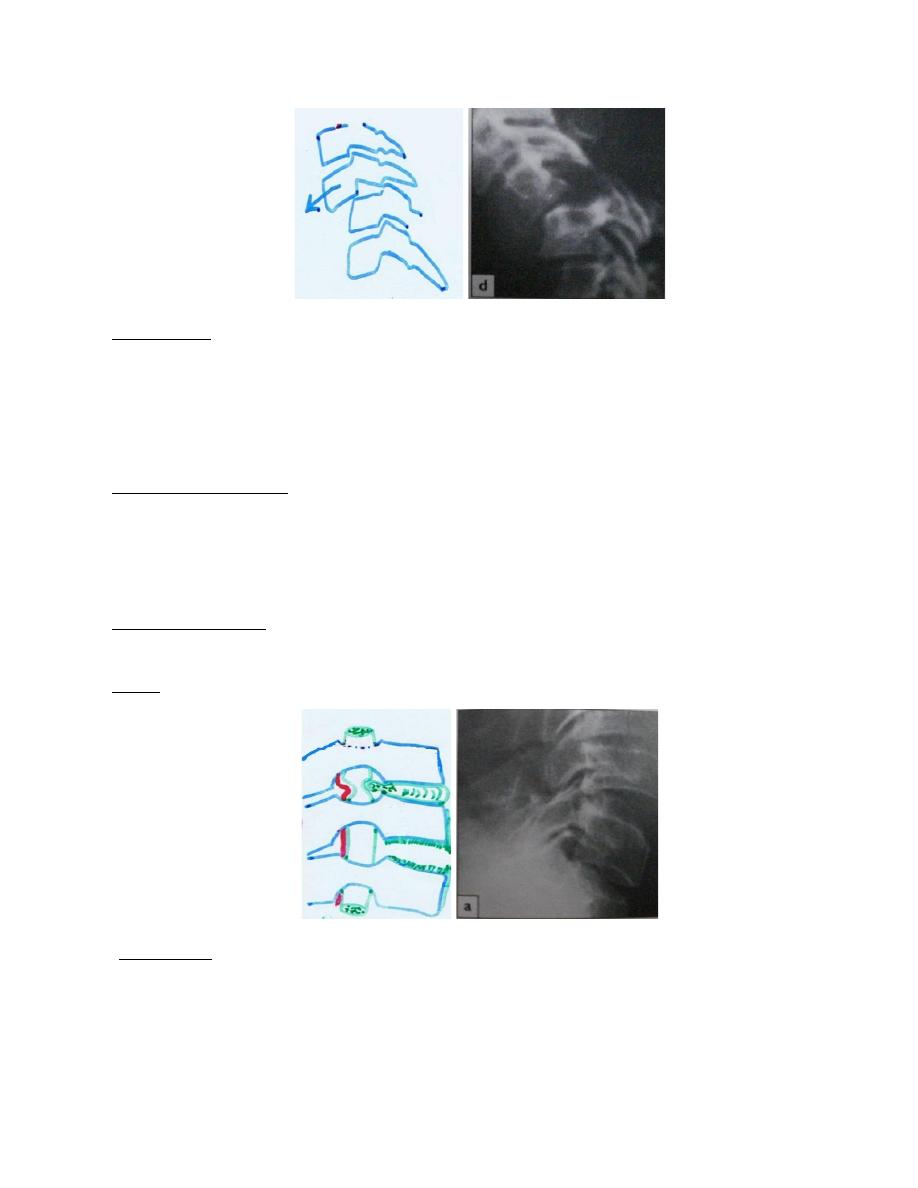
Flexion-rotation injuries
•
Unilateral facet dislocation: This is a flexion-rotation injury but only one
facet joint is dislocated, there may be an associated # of the facet.
*Clinical feature: neck pain, stiffness, deformity and localized tenderness, cord
damage is unusual as the injury is stable.
*X-ray: On the lateral view the vertebral body appears to be partially displaced (less
than one-half of its width), on AP view the alignment of the spinous process is
disrupted.
*Treatment :The dislocation is reduced by skeletal traction ,starting with 5kg & then
increasing up to about one third of body weight ,when the reduction is achieved the
traction is reduced to maintain reduction. If this fail then reduction by manipulation,
after reduction the neck immobilized in a halo-vest for 6-8 weeks.
Indications of operative treatment: (1) failure of closed reduction (2) facet joint # (3)
recurrent dislocation in the halo-vest.
•
Bilateral facet dislocation or # -dislocation :these injuries result from severe
flexion & rotation, the articular facet ride forward over the facet below, one or both
of the facet is fractured ,the posterior ligaments are ruptured &the spine is unstable,
cord damage is usual .
*X-ray: the lateral view show forward displacement of a vertebra on the one below of
greater than one-half its width.
*Treatment : The dislocation is reduced by skull traction ,starting with 5kg & then
increasing up to 30 Kg with intravenous muscle relaxant, if dislocation is reduced
then it is held by ;skull traction for 6 weeks then halo-vest for another 6 weeks or
halo-vest for 12 weeks or by posterior fusion .
Hyperextension injury
*Mechanism of injury: hyperextension of the cervical spine leading to compression
of the posterior bony elements which may be fractured &the anterior structures fail
in tension, with tearing of the anterior longitudinal ligament or an avulsion # of the
antero-superior or antero-inferior edge of the vertebral body, opening up the anterior
part of disc space, fracture of the back of the vertebral body &\or damage to the disc.
*Clinical features: pain, stiffness, facial bruising, laceration &tenderness,
neurological deficit may occur due to pressure by disc or ligamentum flavum.
*X-ray: may show gap between the vertebral bodies anteriorly in extension.
*Treatment: collar in neutral position for 6 weeks.
Avulsion injuries of the spinous process:
It usually affects C7 or T1 spinous process.
*Mechanism of injury: severe contraction of the muscles at the back of neck, it is
known as the clay-shoveller’s #.
*Clinical features: pain, tenderness at the back of the neck.
*Treatment: It is harmless and need only symptomatic treatment with neck exercise
when symptoms permit.
Thoracic spine injuries
* Mechanism of injury: It is caused by hyper flexion leading to wedge -compression
# but #-dislocation also occur. The # is usually stable because the rib cage & sternum
tend to stabilize the entire thoracic segment except the lower two or three segments.
*Clinical features: pain &localized tenderness, neurological deficit not uncommon
because spinal canal is relatively narrow in the thoracic spine.
*Treatment: (1) if there is no neurological deficit and kyphosis < 30 degrees need
symptomatic treatment only, if kyphosis > 30 degrees needs either bracing or
posterior fusion.
(2)If there is cord damage, if damage is complete treatment by bed rest for 6 weeks
followed by bracing, if damage is partial treatment by transthoracic decompression
& stabilization.
Thoracolumbar & lumbar spine injuries
These injuries are classified by Denis into:
•
Minor injuries:
I. Fracture of the transverse processes. These # caused by sudden muscle activity, It
need only symptomatic treatment.
II. Extension injuries .These injuries caused by extension of thoracolumbar spine
leading to # of the spinous process, facets, lamina &pars interarticularis .These
injuries usually occur in weight lifter & gymnast. The injury is stable &need only
symptomatic treatment.
• Major injuries :
I. Wedge Compression #
*Mechanism of injury: It is caused by flexion injury leading to compression # of
the anterior part of vertebral body, the posterior ligament &the middle column
remain is intact so the injury is stable.
* Clinical features: pain is usually marked but neurological injury is rare.
*X-ray: the lateral view reveal # of the anterior part of vertebral body.
*CT-scan: will show that the middle part of vertebral body is intact.
*Treatment :By bed rest for 1-2 weeks ,if wedging is minimal (<10 degrees) no
support is needed, if wedging (10-40 degrees) then support with thoracolumbar
brace or plaster jacket for 3 months, if wedging >40 degrees then anterior
reconstruction and posterior fusion.
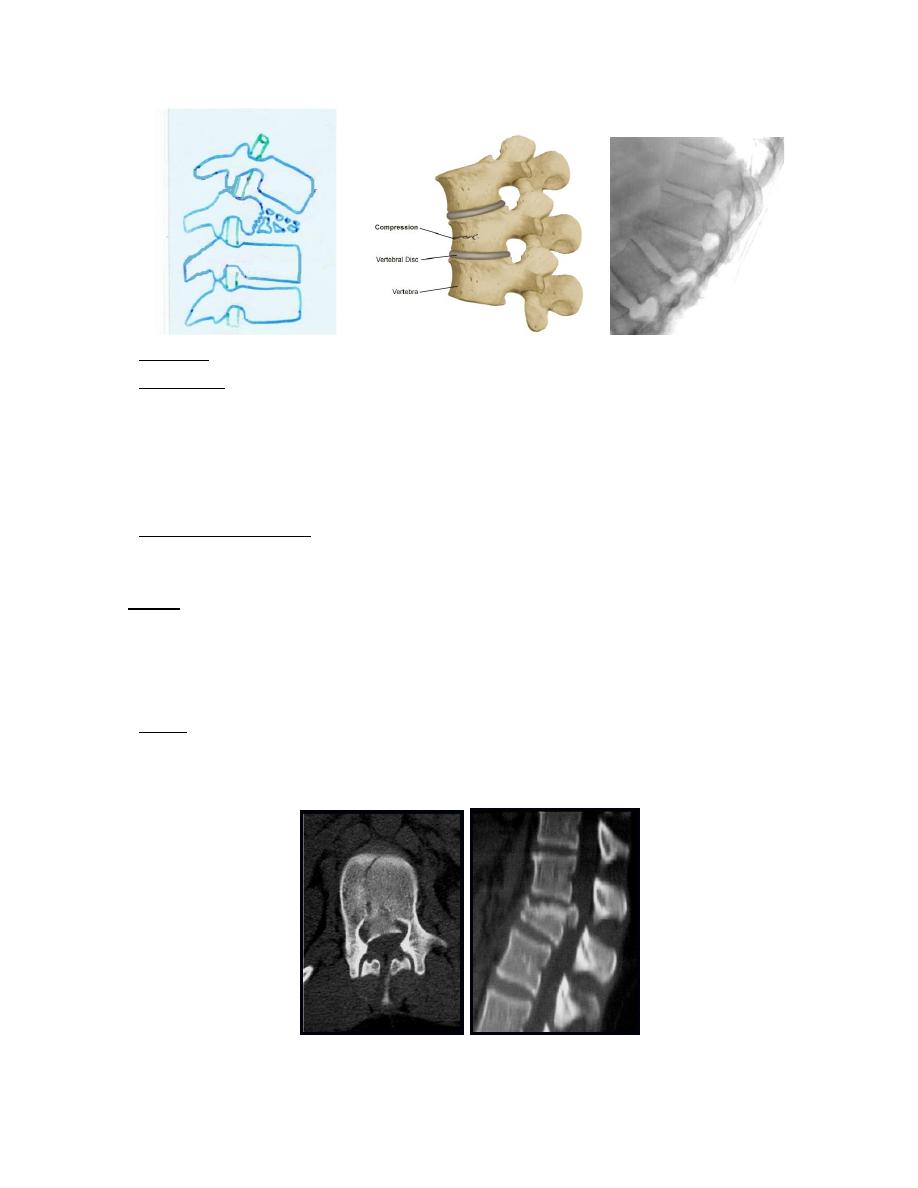
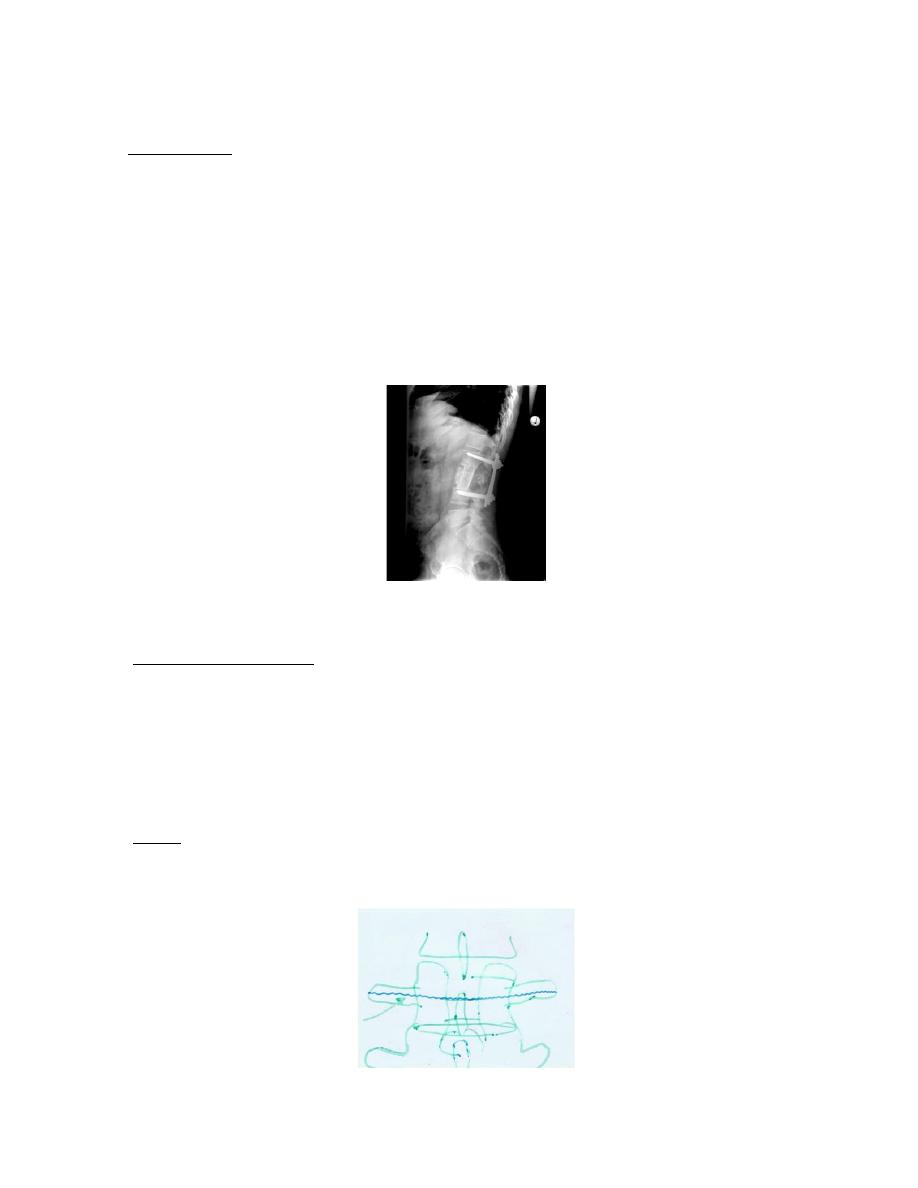
II. Burst injury
*Mechanism of injury: It is caused by severe axial loading lead to explosion of the
vertebral body, with failure of both the anterior &middle columns but the posterior
column usually undamaged.
Note: the L1 vertebra is the most common site of burst # because;
• Its transitional position between inflexible thoracic spine & the mobile lumbar
spine.
• Its horizontal location, neutral location, between thoracic kyphosis &lumbar
lordosis makes it less resistant to axial loading.
*X-ray: AP view may show spreading of vertebral body with an increase of the
interpedicular distance.
*CT scan: it will reveal the posterior displacement of bone fragment into spinal
canal (retropulsion).
*Treatment:
-If there is no or minimal retropulsion, the patient is kept in bed until the acute
symptoms settle &then mobilized in thoracolumbar brace or plaster jacket for 12
weeks.
-If there is retropulsion of bone fragment, the patient is kept in bed for 6 weeks
&then mobilized in thoracolumbar brace or plaster jacket for 6 weeks.
-If there is neurological deficit then operative treatment by anterior decompression
& stabilization.
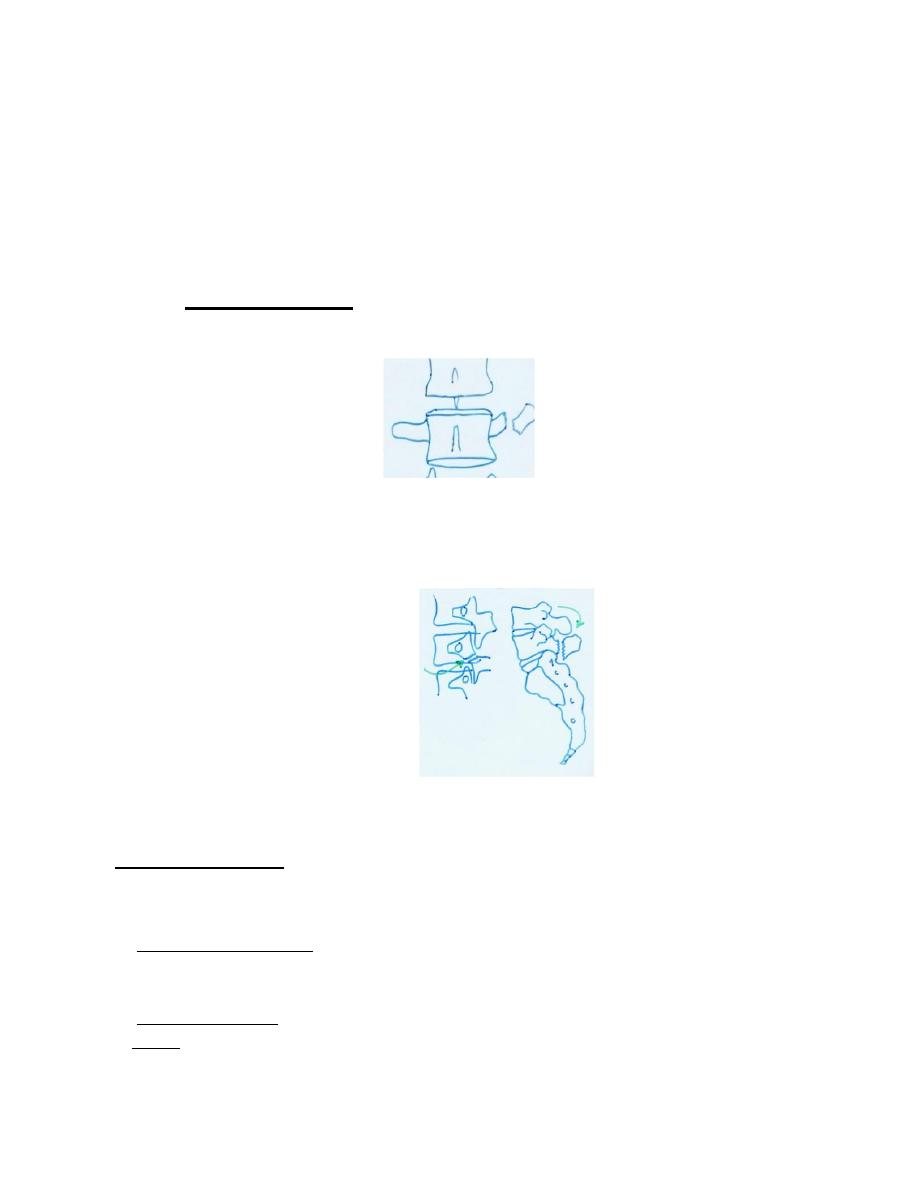
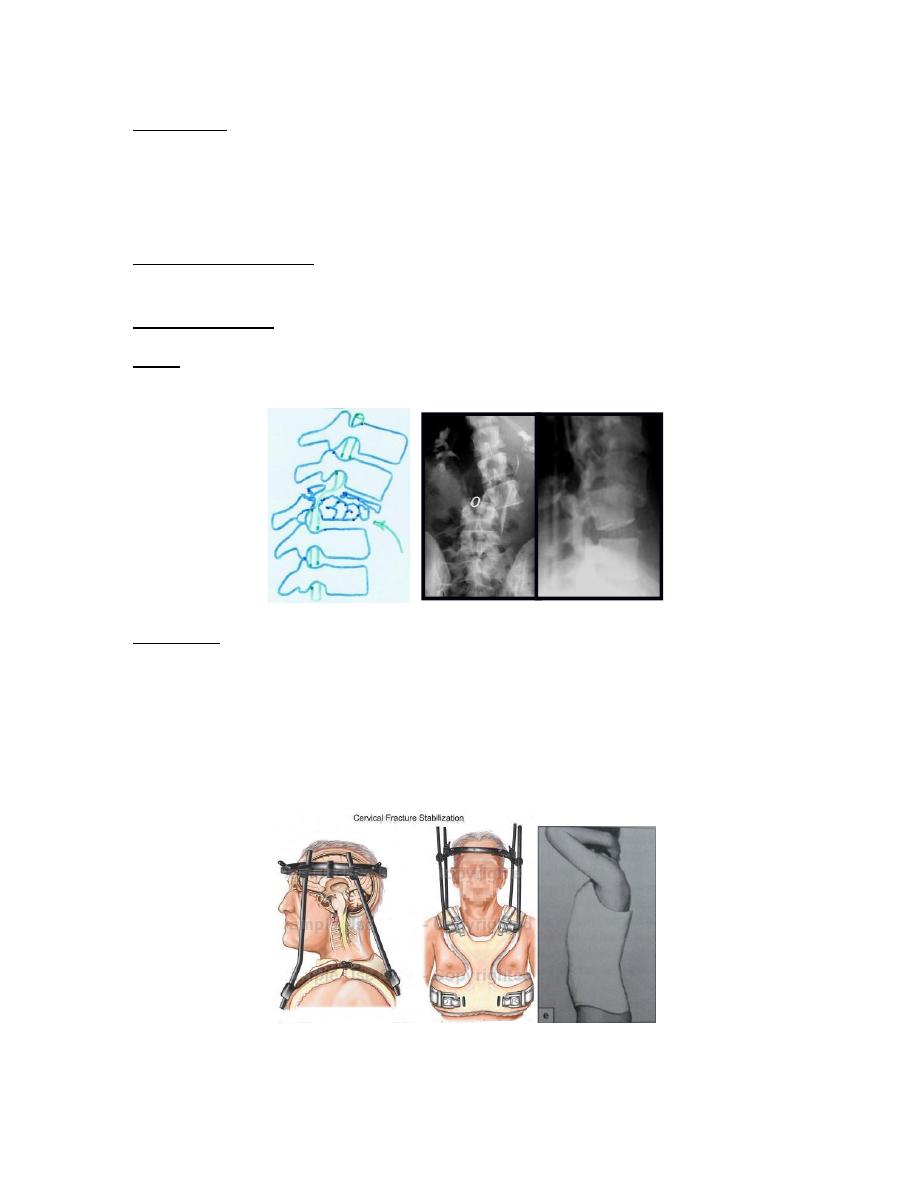
III. Jack-knife injury
*Mechanism of injury: It is caused by flexion &distraction injury of the mid-
lumbar spine which typically occurs in lap seat-belt injuries where the body is
thrown forward against restraining strap. The posterior &middle column fail in
distraction, thus these injuries are unstable in flexion. The most common
associated injury is injury to small bowel.
The tear passes transversely through the bones or the ligament structures or both.
*X-ray: may show the Chance #, in which the split runs through the spinous
process, the transverse processes, the pedicles &the vertebra body. In the AP view
the apparent height of vertebral body may be increased.
*Treatment: Chance # because it is bony injury heals rapidly & require 3 months
immobilization in plaster jacket or thoracolumbar brace. Severe ligamentous
injuries require posterior spinal fusion.
IV. Fracture-dislocation
*Mechanism of injury: It is caused by a combination of flexion, compression,
rotation& shear. All 3 columns are displaced & the spine is grossly unstable.
*Clinical features: usually there is lower cord or cauda equine damage.
*X-ray: Show # through body, pedicles, lamina, and articular processes, with
subluxation or dislocation. *CT-scan: to see the degree of canal occlusion.
*Treatment: If there is no neurological deficit or there is complete paraplegia, the
treatment is conservative by bed rest followed by thoracolumbar brace or plaster
jacket.
If there is partial neurological, the treatment is by surgical decompression
&stabilization.
Halo-vest Plaster jacket
