


1
The Dental Analysis
This part of the analysis is designed to confirm the clinical observations already made
and to determine the position of the dentition with respect to their respective bony
bases and to each other.
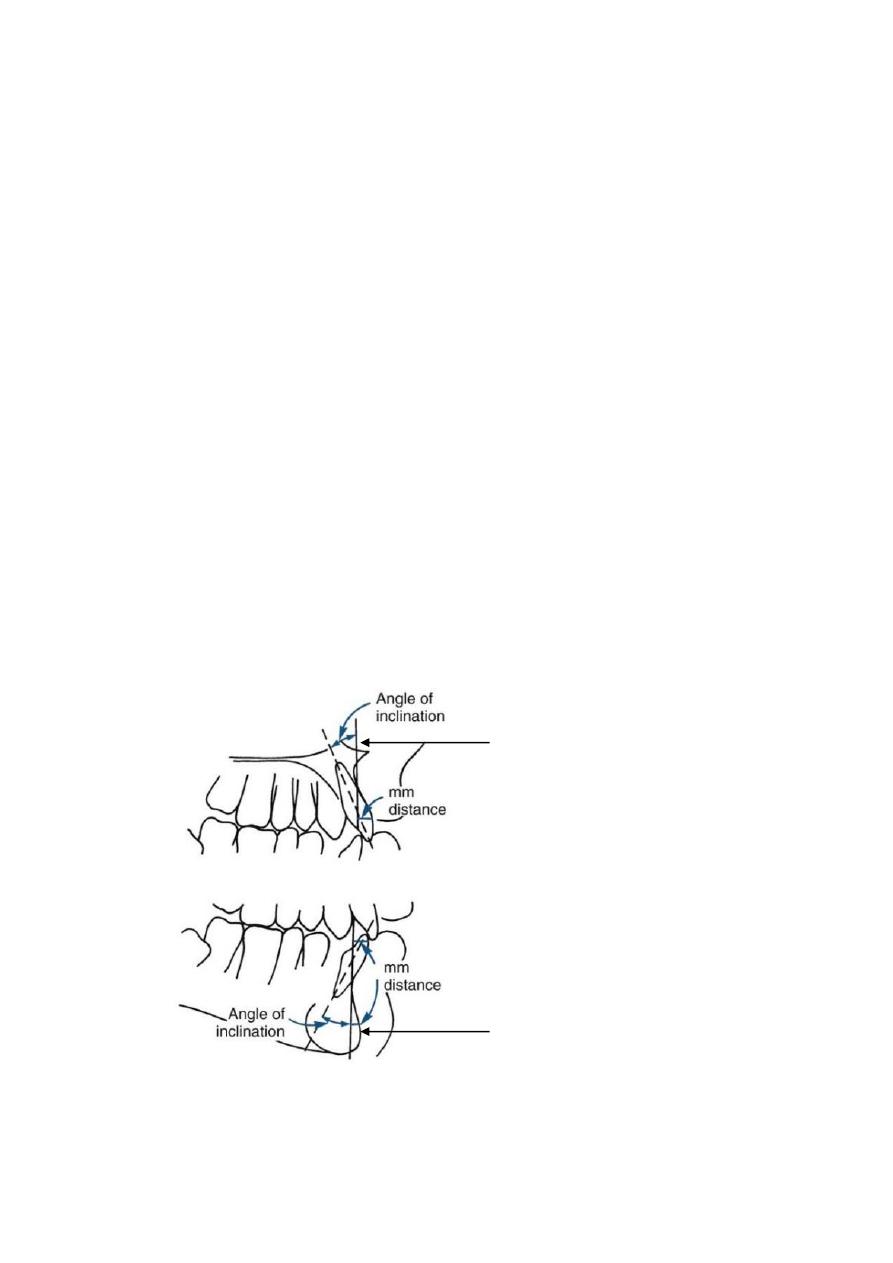
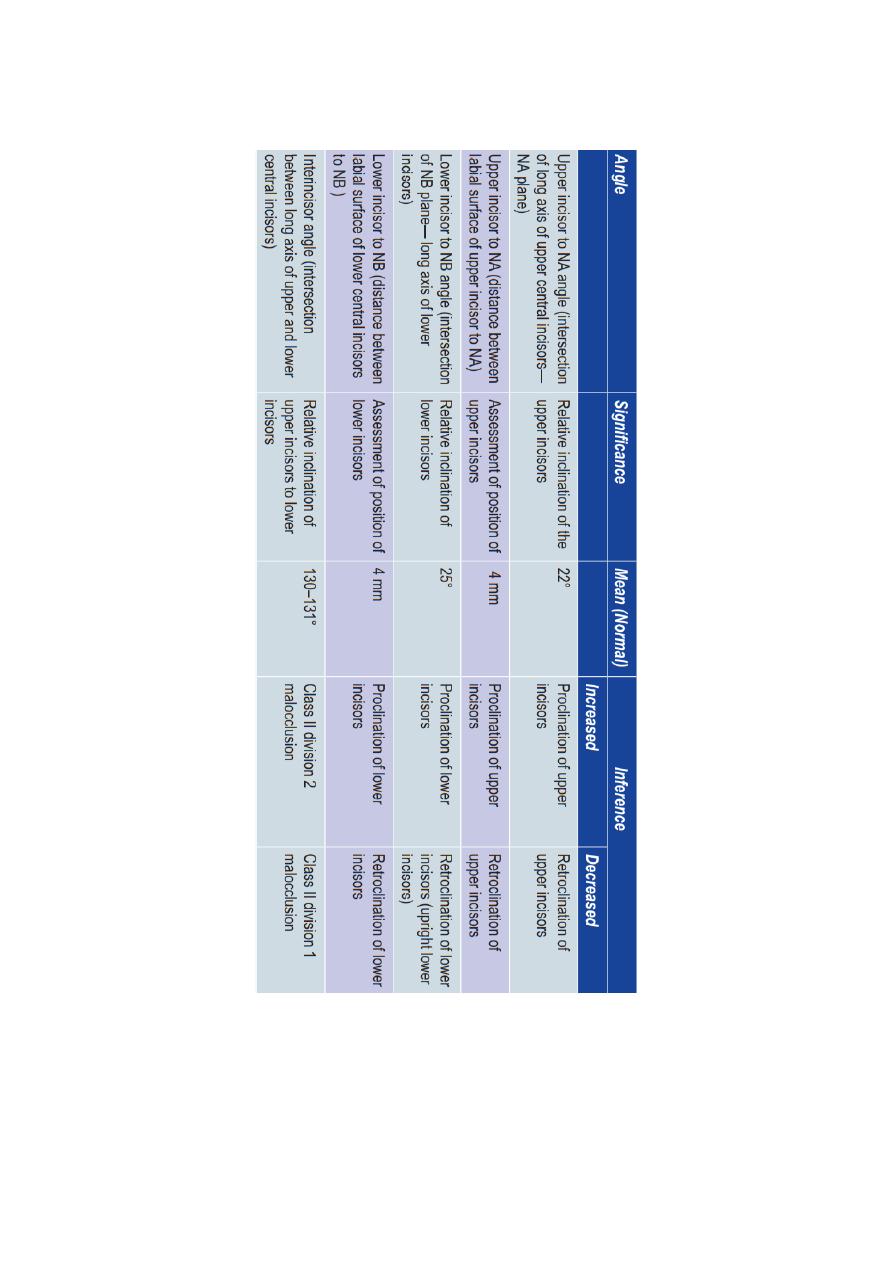
incisor position
The relative antero-posterior linear position and angulation of the lower incisor teeth
is determined by relating the most protruding incisor tooth to the N-B line.
The
maxillary incisor is related to the N-A plane both by angular as well as linear measurements.
The upper incisor to N-A reading in degrees indicates the relative angular relationship of the
upper incisor teeth, whereas the upper central incisor to N-A reading in millimeters provides
information on the relative forward or backward positioning of the incisor teeth to the N-A
line The upper central incisors should relate to the N-A line in such a way that the most
anteriorly placed point of its crown is 4 mm (but may range up to 7 mm) in front of the N-A
line and its axial inclination bears a 22° angle to the line. To precisely determine the relative
anteroposterior position of the incisors, it is necessary to measure the distance of the most
labial surface of the incisor to the N-A line.
The lower incisor to N-B line measurement in millimetres shows the relative forward
or backward positioning of these teeth to the N-B line. In degrees indicates the
relative axial inclination of these teeth. The most labial portion of the crown of the
lower incisor teeth should be located 4 mm ahead of the N-B line, and the axial
inclination of this tooth to the N-B line should be 25°.
N-A line
N-B line
2
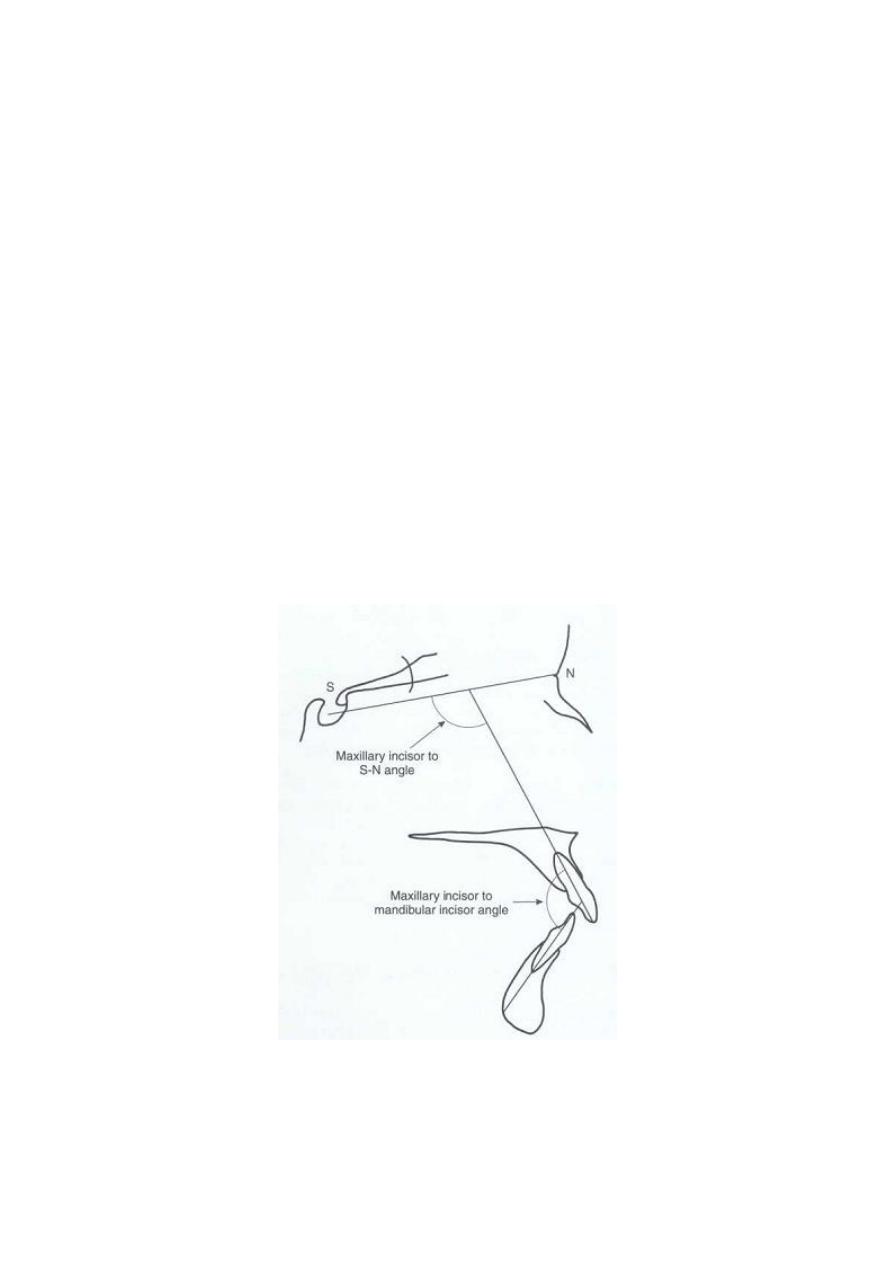
Maxillary incisor to S-N plane angle
It is formed by intersection of the line passing through the incisal edge and apex of the
root of the most labially upper central incisor to the S-N line (102° ±5).
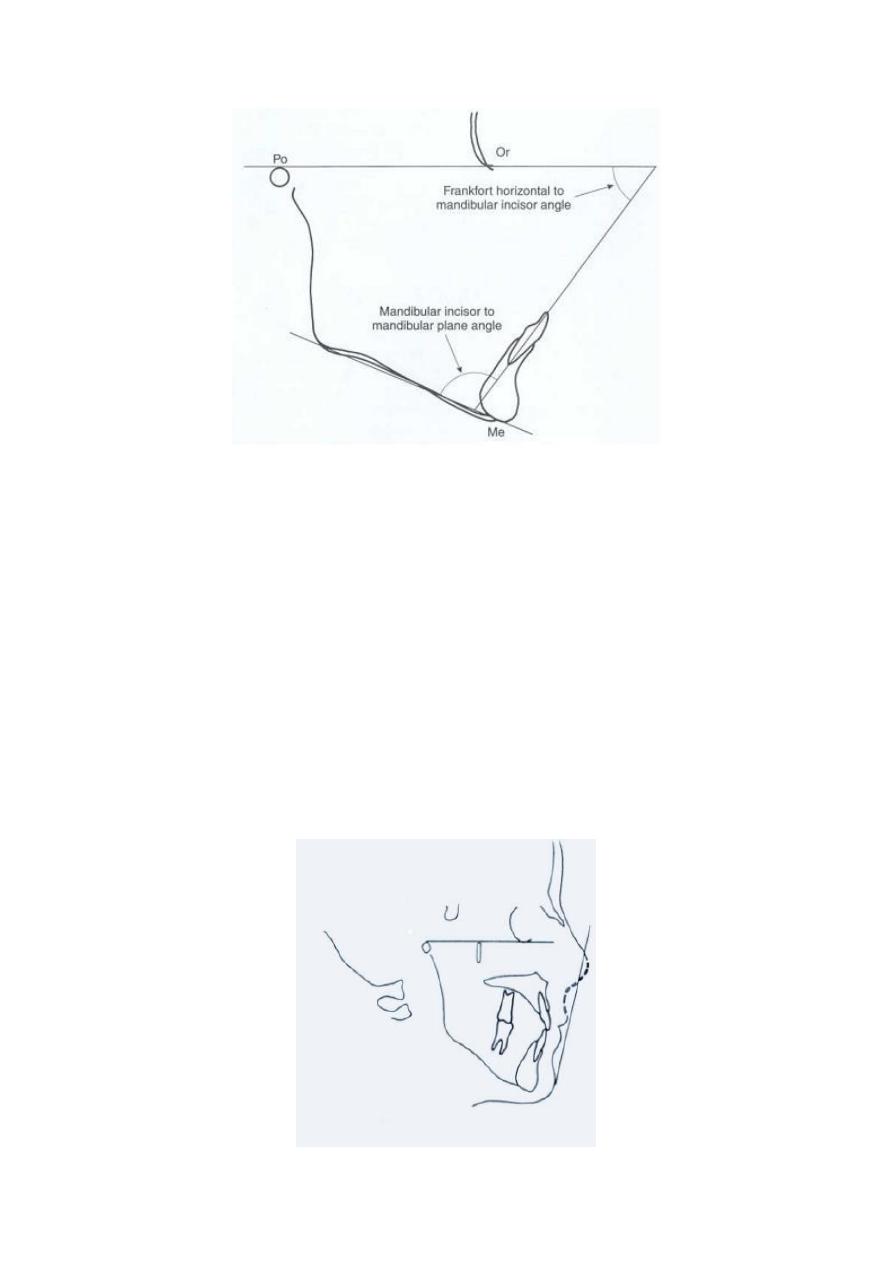
Mandibular incisor mandibular plane angle
It is formed by the intersection of the mandibular plane with a line passing through
the incisal edge and apex of the root of the mandibular central incisor (95° ± 6).
Inter-incisal angle
The inter-incisal angle relates the relative position of the upper incisor to that of the
lower incisor. If the angulation is more acute or less than the mean of 130°, then the
anteriors are considered to be proclined. Hence, the upper and/ or lower teeth may
require up-righting or need to be retracted. Conversely, if the angle is greater than
130° or more obtuse, the upper and / or lower incisors may require advancing
anteriorly or correction of their axial inclinations. The chin forms one of the most
important landmarks on the profile.
Upper incisor angle to the anterior cranial base and inter incisal angle.
3
Mandibular incisor angles to the mandibular and Frankfort horizontal planes.
The soft tissue analysis
The analysis laid emphasis on the soft tissue profile as well as the underlying skeletal
structure. The profile was mainly affected by the chin, nose and the lips. The shape
and posture of the lips is partially governed by the underlying dentition and thus can
be modified orthodontically. The thickness of the tissue over the symphysis and the
nasal structure also contributes to the prominence of the lower face and attention
should be paid to the same when as it may camouflage the underlying malocc1usion.
lip line
Steiners lip analysis reference point is the centre of the s shaped curve between the
tip of nose and sub nasale reference line extends from this point to the soft tissue
pogonion lips behind this point are said to be flat (retrusive) lips ahead of this line are
said to be too prominent ( protrsive).
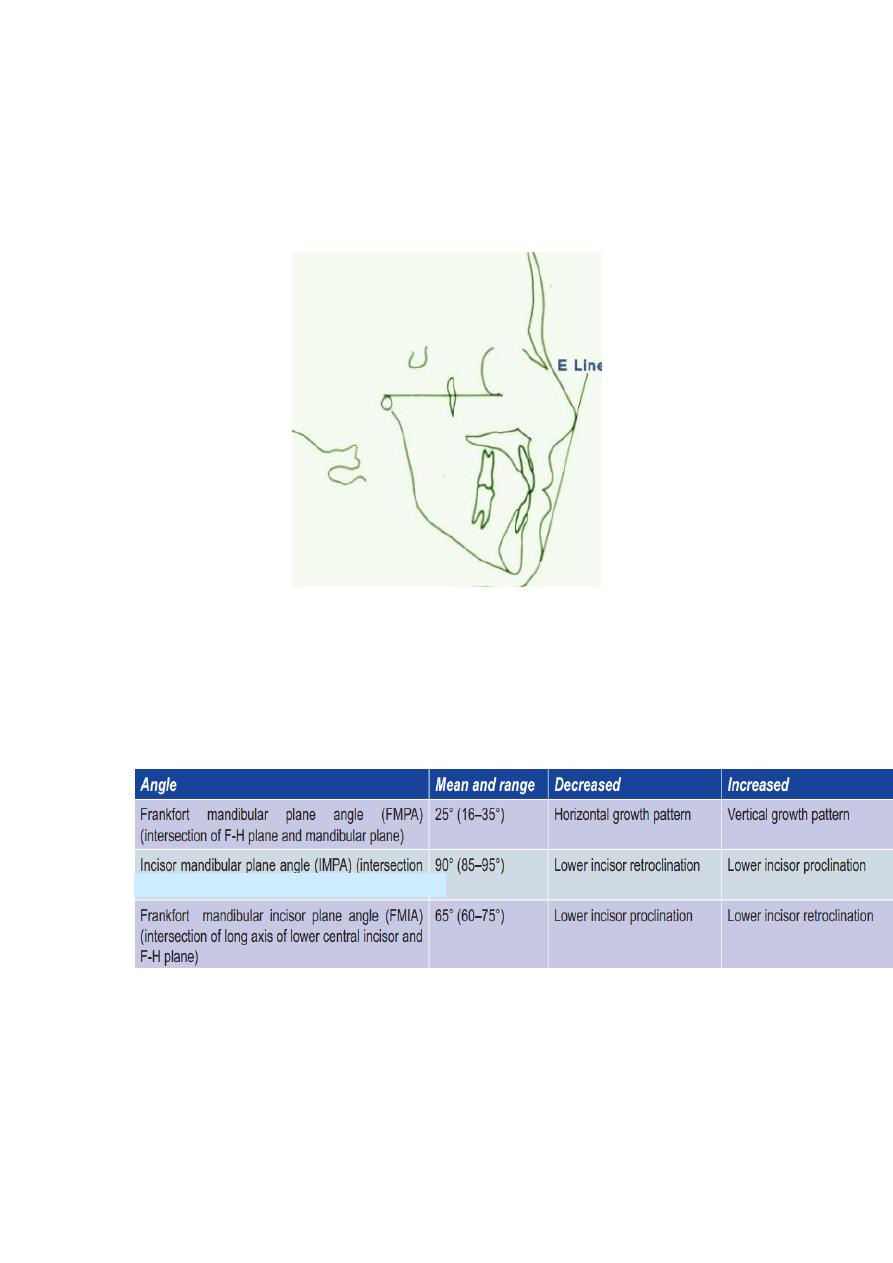
4
Rickets lip analysis reference line connects nose tip to soft tissue pogonion - e line
lips are analysed e line depending on the distance e of the lips from this line normal
values upper : 2-3 mm lower : 1-2 mm.
Tweed’s triangle
The Tweed’s triangle makes use of three planes that form a diagnostic triangle called Tweed’s triangle.
of long axis of lower incisor and mandibular plane)
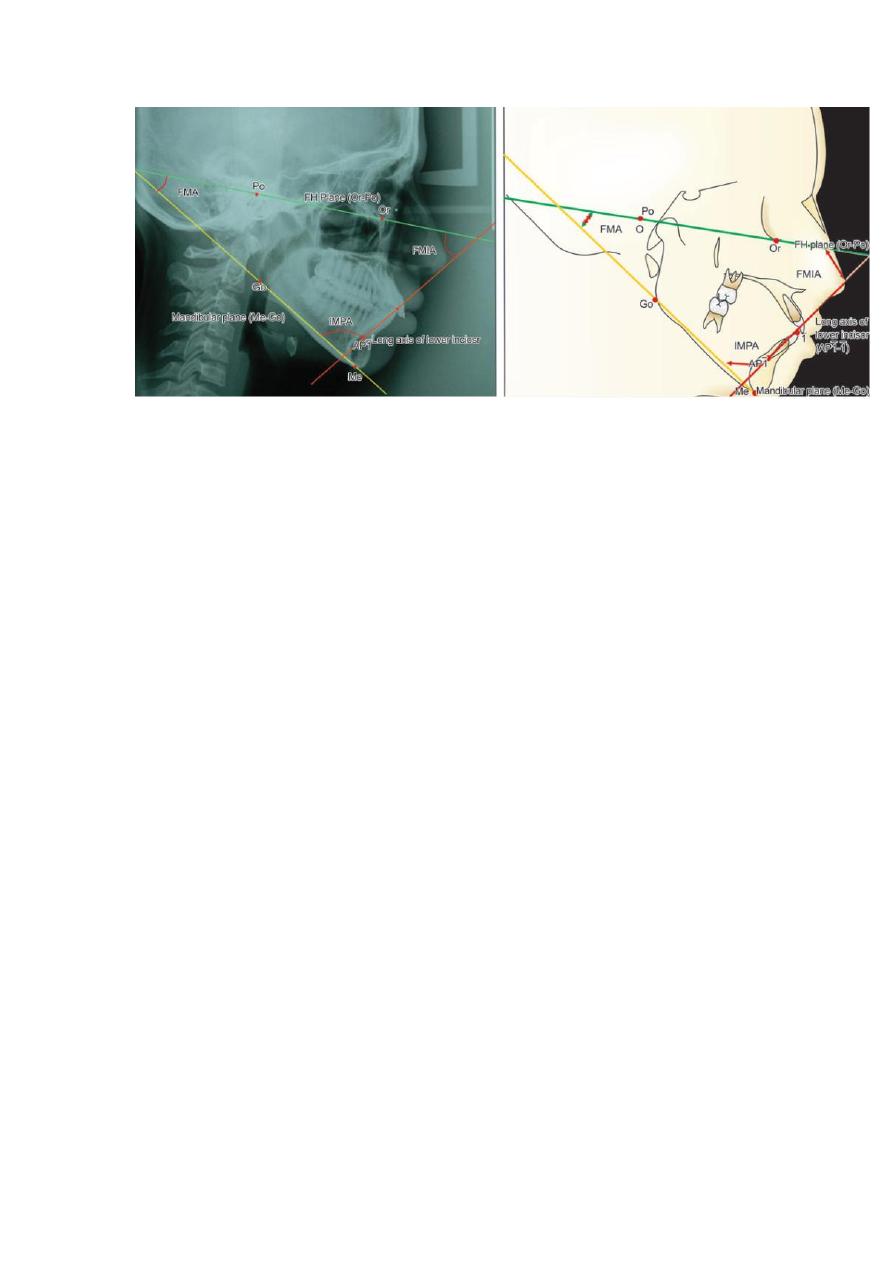
5
6
Steiner 'dental analysis

7
Steiner’s skeletal analysis
8
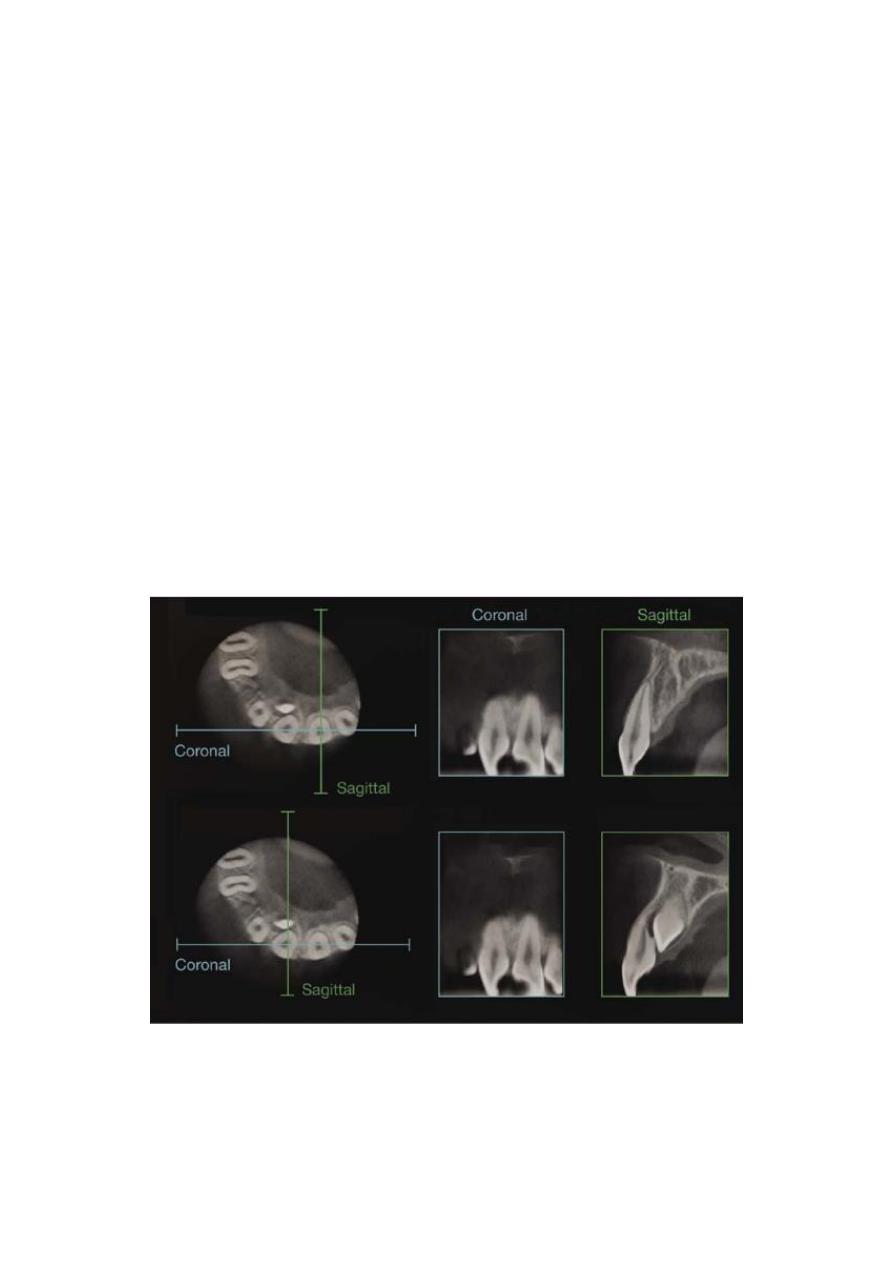
Three-dimensional imaging
Plain film and cephalometric radiography are invaluable for accurate diagnosis and
treatment planning, but they only provide a two-dimensional image of a three
dimensional structure, with all the associated errors of projection, landmark
identification, measurement and interpretation. A number of three-dimensional
imaging techniques have been developed over the past decade, which help to
overcome some of these shortcomings and give the orthodontist greater information
for diagnosis, treatment planning and research. Imaging of the hard tissues composing
the jaws and dentition using computed tomography (CT) had remained impractical
until relatively recently, due to the high radiation dosage, lack of vertical resolution
and cost. However, with the introduction of cone-beam computed tomography
(CBCT), doses have been reduced and resolution increased, and although not yet used
for routine orthodontic diagnosis, this technique is proving a very valuable tool in
certain circumstances, particularly the diagnosis of impacted and ectopic teeth. It can
also be very useful in airway analysis, assessment of alveolar bone height and volume
prior to implant placement and imaging of temporomandibular joint morphology.

9
Other less invasive techniques for generating three-dimensional images of the facial
soft tissues have also been developed. Optical laser scanning utilizes a laser beam,
which is captured by a video camera at a set distance from the laser and produces a
three-dimensional image. Stereo photogrammetry involves taking two pictures of the
facial region simultaneously, which creates a three-dimensional model image using
sophisticated stereo triangulation algorithms. These techniques have been used to
study facial growth and soft tissue changes in normal populations and following
orthodontic and surgical treatment.