


INTERNAL RIGID FIXATION
The term internal rigid fixation has many definitions. One definition is “any form of bone fixation in which otherwise deforming biomechanical forces are either countered or used to advantage to stabilize the fracture fragments and to permit loading of the bone so far as to permit active motion”Examples of rigid fixation in the mandible are the use of two lag screws or bone plates across a fracture, the use of a reconstruction bone plate with at least three screws on each side of the fracture, and the use of a large compression plate across a fracture
ADVANTAGES
Prevention of interfragmentary mobility leading to a peculiar type of bone healing where no callus forms. The bonesinstead go on to heal by a process of haversian remodeling.
A remodeling phase then converts the entire area to morphologically normal bone. This type of bone healing is termed primary or direct bone union, and it requires absolute
immobilization between the osseous fragments, and minimal
distance (gap) between them.
Fractures of the angle under most functional situations
tend to “open” at the superior border.Champy miniplate technique functions extremely well for this fracture and consists of a 2.0 mm miniplate applied with monocortical screws along the superior border. Because metallic plates have high tensile strength, even thin plates work adequately at the angle to prevent the tendency for a gap to form at the superior border under function.
The advantages to using the Champy method include a decreased risk of infection, shorter operating time, and more rapid return to form and function when compared with other more rigid techniques.
Isolated fractures of the mandibular body behave similarly under function,with a tendency for a gap to form at the superior surface, but the more anterior the fracture, the more tendency for torquing of the fragments to occur, causing mediolateral misalignment of the inferior border. A plate or lag screws on the body of the mandible is necessary to prevent the mediolateral displacement that accompanies the torquing motion under function.
For isolated body fractures, this can be a relatively small plate, such as a 2.0 mm miniplate or even a single lag screw combined
with a solid arch bar.

The anterior mandible undergoes shearing and torsional (twisting) forces during functional activities. Application of fixation devices must therefore take these factors into consideration.
This is why most surgeons advocate two points of fixation in the symphysis: either two bone plates, two lag screws, or possibly one plate or lag screw combined with an arch bar
MID-FACIAL FRACTURES
AnatomyThe maxilla, palate, nasal bones, and zygomas comprise most of the midfacial skeleton. The ethmoids, greater wing of the sphenoid, and frontal bone comprise elements of the bony orbit and connect the anterior facial skeleton to the cranial base.
Forces directed onto the midfacial skeleton are absorbed and transmitted through vertical and horizontal buttresses. These buttresses constitute areas of dense, thick bone that support the maxilla and are more resistant to deformation when forces are applied. They are not only important in protecting the vital structures of the midface but they are also essential landmarks used during reconstruction. The buttresses provide higher quality bone for internal fixation and guide reconstruction of facial height, width, and projection.
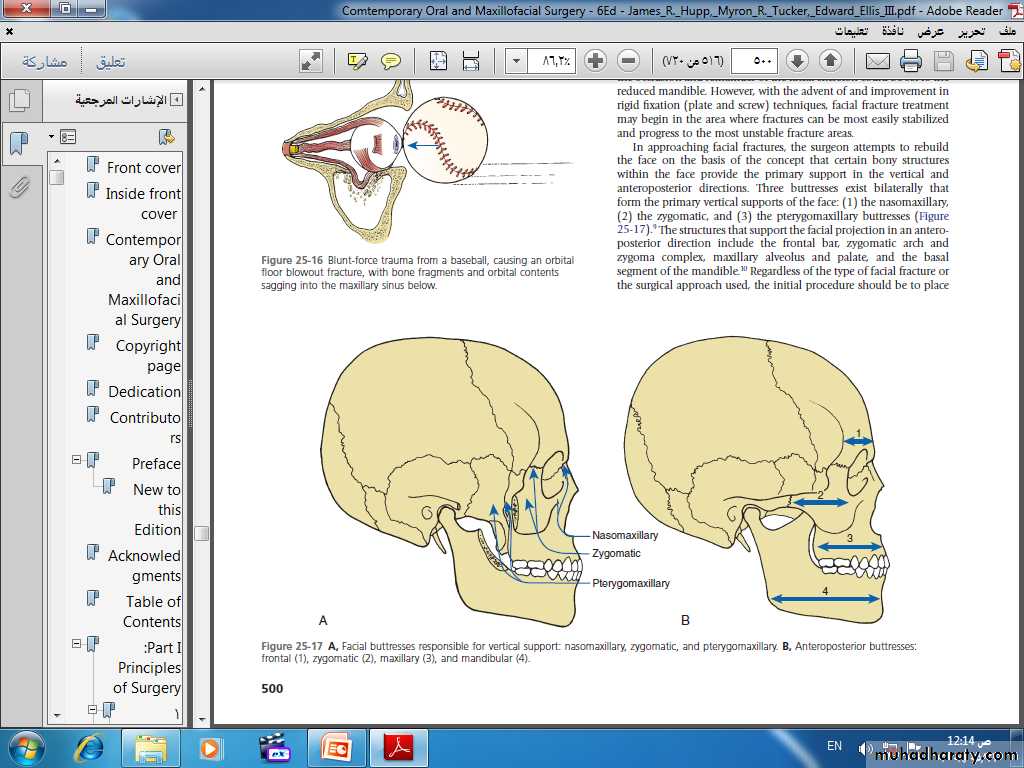
MIDFACIAL BUTTRESSES
The midface is more resistant to vertical forces than horizontal and shear forces. This resistance is because of the strength of the vertical buttresses:Nasomaxillary (medial)
Zygomaticomaxillary (lateral)
Pterygomaxillary (posterior)
Antero-posterior buttresses:
frontal (1),zygomatic (2), and
maxillary (3).
Although the horizontal buttresses have less impact on force dissipation, they are important for the restoration of facial width. The horizontal buttresses include:
Superior orbital rims (superior)
Inferior orbital rims/zygomatic arch (central)
Maxillary alveolus (inferior)
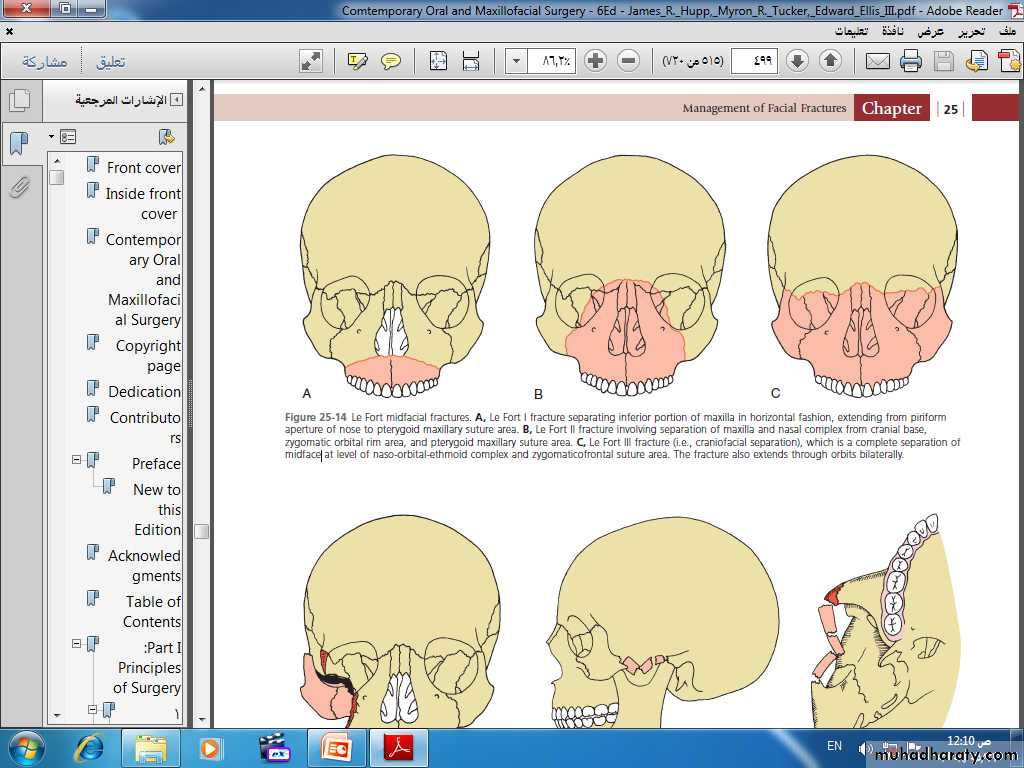
MAXILLARY FRACTURES
Le Fort I LevelMaxillary fractures at the Le Fort I level traverse the lateral antral wall, the lateral nasal wall, and the lower third of the septum, and they separate at the pterygoid plates. Thus, the entire mobilized segment consists of the maxillary alveolar bone, the palatine bone, the lower third of the nasal septum, and the lower third of the pterygoid plates. The superior two-thirds of these bones remain associated with the face.
Le Fort II Level
Unlike the horizontal separation noted in the Le Fort I fracture, the Le Fort II fracture is pyramidal in shape. The fracture extends from below the nasofrontal suture through the nasal bones along the maxilla to the zygomatico-maxillary suture and includes the medial inferior third of the orbit. The fracture then continues along the zygomatico-maxillary suture to and through the pterygoid plates. The septum is also separated superiorly. The segments may be intact below this line of fracture, but they are most often comminutedLe Fort III Level
Fractures at the Le Fort III level involve the nasal bones, the zygomas, the maxillae, the palatine bones, and the pterygoid plates. These fractures essentially separate the face along the base of the skull. The fracture line extends from the nasofrontal suture along the medial wall of the orbit through the superior orbital fissure. It then extends along the inferior orbital fissure and the lateral orbital wall to the zygomatico-frontal suture. The zygomatico-temporal suture is also separated. The fracture then extends along the sphenoid bone, separating the pterygoid plates. The septum becomes separated at the cribriform plate of the ethmoid. Le Fort III fractures are most often comminuted.CLINICAL PRESENTATION
Soft tissue lacerations, edema, nasal bleeding, pain, ecchymosis, and bony steps along the fractures lines may be appreciable on visual inspection and palpation. In addition, a change in occlusion is often found.For LeFort I fractures: maxillary mobility may be present. However, the absence of mobility does not preclude a fracture. If the maxilla has been impacted, there may be no mobility and the anterior facial height may be decreased. There is typically an anterior open bite.
Ecchymosis in the region of the greater palantine foramen, or Guerin sign, and ecchymosis in the buccal vestibule also indicate a LeFort I fracture. Cracked-pot sound on percussion of upper teeth.
LeFort II fractures typically present with periorbital and subconjunctival ecchymosis in addition to the findings outlined earlier.
* A bony step at the infraorbital rim may also be detectable.
* Disruption of the infraorbital nerve leads to anesthesia of the upper teeth, gingiva, upper lip, and lateral aspects of the nose.
* Diplopia with restricted superior gaze.
* If the nasal bones and maxilla are mobile, a LeFort II fracture should be suspected.
* A dish-faced appearance may be present as a result of decreased nasal projection.
* CSF rhinorrhea may be present, suggesting a basilar skull fracture.
LeFort III fractures involve mobility of the maxilla, nasal bones, and zygomas as a single unit.
A palpable bony step may be present at the zygomaticotemporal or zygomaticofrontal suture.
As with LeFort II fractures, bilateral periorbital edema (raccoon eyes) and CSF rhinorrhea may be present.
Lengthening of the facial height, orbital hooding, and enophthalmos are also typically present.
Tenderness and deformity of the zygomatic arches.
Tilting of the occlusal plane with gagging on one side.
Ecchymosis over the mastoid region (Battle sign) may be present, in addition to CSF otorrhea and hemotympanum.
MODALITIES OF TREATMENT
1. Closed reduction and IMF2. Open reduction and direct fixation: Plating or wiring
3. Suspension wiring: Circumzygomatic, Fronto-zygomatic, Infraorbital rim wire, Piriform fossa wire, Circumpalatal
4. External fixation: Head frame, Halo-frame, Plaster of Paris head cap
5. K-wire or Steinman pin
In cases involving fractures with minimal displacement and no change in occlusion, no treatment other than a nonchew diet for approximately 4 weeks may be indicated. However, these cases are rare.
Closed reduction techniques involving (IMF) for a period of 4 to 6 weeks can be used. In cases in which there is displacement of the maxilla with an occlusal discrepancy, Rowe disimpaction forceps can be used to mobilize and reduce the maxilla.
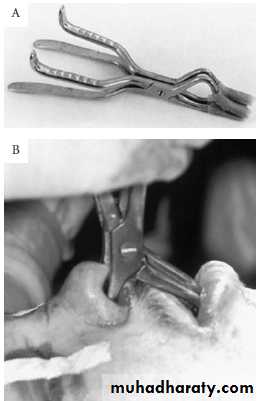
A, Rowe disimpaction forceps.
B, Application of the forceps.

The most common treatment of maxillary and LeFort fractures remains open reduction with internal fixation. The general treatment approach involves:
Exposure of the fractures
Mobilization and reduction of fracture segments
Establishment of occlusal relationships (IMF)
Rigid or semirigid fixation
Bone grafting when necessary
Resuspension/repair of soft tissue injuries
The most common approach for exposure of a LeFort I level fracture is the buccal vestibular incision
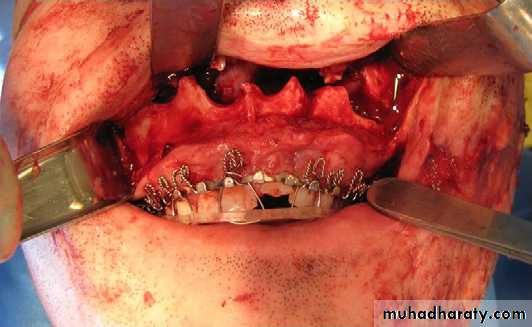
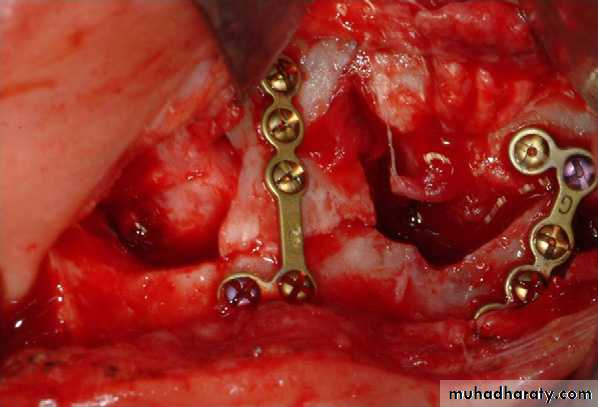
Next, the fractures are fixated with either bone plates or interosseous wiring. The fixation pattern and method are dependent on the specific fracture location and bone available. The most common method is to use 4-point fixation at the zygomaticomaxillary and nasomaxillary buttresses with 1.5-mm to 2.0-mm miniplates. If bony gaps exist, autogenous grafting can be used.
Suspension wiring is sometimes used in addition to direct wiring or bone plating. The purpose of suspension wiring is to provide stabilization of fractured bones by suspending them to a more stable bone superiorly. The use of direct and suspension wire fixation does have significant limitations in many cases.
The limited rigidity of wires may make it difficult to reconstruct and maintain the appropriate anatomic contours. Rigid fixation using plating systems for the most part has eliminated the need for suspension wires.
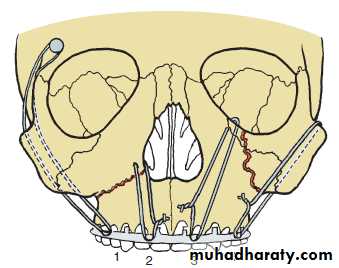
Suspension wiring techniques:
1, Frontal bone suspension.2, Piriform rim wiring.
3, Inferior orbital rim suspension.
4, Circumzygomatic suspension
The severely comminuted midface injury may create a challenge for open reduction. In patients who cannot undergo autogenous grafting or for those who do not tolerate IMF because of medical or psychological reasons, external fixation with a halo head frame can be used.