Coll. Medicine \3rd stage
ParasitologyProf.Dr. Amal KH. KH.
Lec. 3
Other intestinal amoebae
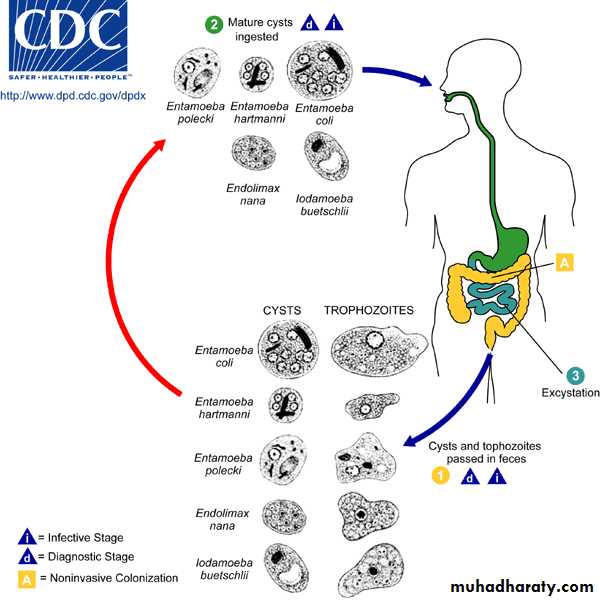
Entamoeba coli:-Is usually the most common amoebic parasitic of man . Although it is a harmless in the lumen of the caecum and lower levels of the large intestine , its presence is concrete evidence that the host has ingested fecal material.
All typical life-cycle stages are found in Entamoeba coli as, trophozoite, precyst, cyst and metacystic stages.
The trophozoite is a sluggish , quite viscous protoplast . The pseudopodia are broad , short and do not typically extend any considerable distance from the main mass of protoplasm .nucleus with peripheral karyosome. Bacteria and other enteric microbes , which are seen within food vacuoles , constitute the food of E. coli . Trophozoites of E. coli and other amoeba are rarely seen in the stool except when it is frankly diarrheic .
The cyst is usually larger than that of E. histolytica . When first formed the cyst has a single nucleus but as it matures it passes through successive stages with 2 to 8 nuclei , occasionally reaching the extraordinary number of 16 to 32 or more . However, there are usually one or more dense masses of glycogen with foggy edges and sharp- ended chromatoidal splinters. There is no clinical indication for treatment since Entamoeba coli is harmless.
Endolimax nana:-
It is found in the lumen of the caecum and lower levels of the large intestine and produced no lesions, but like E. coli its presence indicates that polluted material has been ingested . As the species name nana (dwarf) suggests, this amoeba is small compared with E. histolytica .The trophozoite has endoplasm that is finely granular with numerous minute vacuoles , so that it has a foggy appearance . In contrast, the ectoplasm, with one or more short finger- like pseudopodia when the organism displays activity , is hyaline and almost transparent . The nucleus is ovoidal or sub spherical . There is a relatively large karyosome , consisting of a mass of granules , commonly eccentric in position ,
In preparation for encystation Endolimax nana discards all undigested inclusions and consolidates into an ovoidal or sub spherical mass. A delicate cyst wall is then secreted . The mature cyst contains four nuclei . Masses of glycogen with a hazy margin may obscure the nuclei. Chromatoidal bodies , if present in the cytoplasm are coccoid or short curved rods.


Iodamoeba buetschlii:-


it is a harmless commensal living in the lumen of the large intestine .
The trophozoite is sluggish , with little evidence of pseudopodial extension and the thin layer of ectoplasm is not easily distinguished from the endoplasm except that the latter is denser and has a more viscous , granular composition . This trophozoite has a diameter of 8 to 20 microns . The nucleus is spherical , has a rather thick membrane , a karyosome which is central or somewhat eccentric in position and contains an inner chromatic granule surrounded by achromatic globules , all anchored to the nuclear membrane by radial filaments . Minute chromatin granules have also been described as lining the nuclear membrane. In addition to food- containing vacuoles this amoeba is unique in its trophozoite stage in having in its cytoplasm one or two distinct rounded masses of glycogen. When the organism encysts it discharges undigested material, becomes somewhat condensed and secretes a cyst wall.The cyst is irregularly rounded and usually contains only one .The clearly outlined glycogen mass which stains a deep mahogany brown with iodine readily differentiates Iodamoeba buetschlii from the other intestinal amoeba.
Extra- intestinal amoebae
Entamoeba gingivalis:-
It is a parasite of the mouth of man and is most commonly found as a phagocyte in diseased gums and tonsils. Only the trophozoite stage has been described; the only plausible method of transmission is through droplet spraying of saliva or during more intimate oral contact.
E. gingivalis is closely resembles E. histolytica, with a few to several finger-like pseudopodia, finely granular endoplasm and clear ectoplasm. the nucleus contains a small karyosome which is central or slightly eccentric in position and is surrounded by a thin halo .
Facultative amoeba parasites
Naegleria fowleriThis free living amoeba exist as either an amoeboid trophozoite , a biflagellate trophozoite, and a cyst . it multiplies in the amoeboid trophozoite form , the only form found in human being . the amoeboid trophozoite appears elongate . this form is actively motile , that this, it moves more than two body length per minute. The cytoplasm shows a pulsating vacuole . the nucleus is visible only in the stained preparation . it has a large central karyosome . this soil amoeba convert from amoeboid trophozoite to a biflagellate trophozoite when it reaches water . this non feeding , non dividing , biflagellate form helps the spread of Naegleria fowleri to fresh pools when it rains . the biflagellate form not multiply . it has convert back to amoeboid form for multiplication . a smooth walled cystic stage occurs only in the external environment . cysts never form in human body.
Life cycle :
The entire life cycle of Naegleria fowleri completed in the external environment . excystation occur in favorable condition . the amoeboid trophozoite form multiply by binary fission . this form encyst under unfavorable condition . the biflagellate trophozoite form helped in the spread of Naegleria fowleri to new water bodies . human primarily contract this amoeba by swimming in contaminated water . the amoeboid form enter human body through nasal mucosa and often migrate to the brain , causing rapid tissue destruction . some infection result by inhaling dust contaminated with Naegleria fowleri cysts .
Pathogenesis and clinical features :
The disease is common in young adults and children . the parasite reach the brain through the cribriform plate, along the olfactory nerves after initial lodgment in the nose . the incubation period ranges from 2 to 15 days . the amoeboid trophozoite form multiplies in the gray matter of the brain . the patient has sever headache , cranial nerve palsies and signs of meningism . most patients die within a week . A few patients have survived after treatment with Amphotericin B and rifampicin .Naegleria fowleri and related organisms also cause humidifier fever , a form of allergic alveolitis resulting from inhaling air from air- coolers. . these amoeba grow in water of the air- coolers .
Diagnosis :
Wet mount preparation of CSF may appear the amoeboid trophozoite . fixed preparation stained with iron heamatoxilin will reveal the trophozoite along with their nuclear details .
Acanthamoeba sp
There are seven species of Acathameoba known to infect human . Acathameoba culberttsoni is most common .
Morphology :
Acathameoba sp in two forms trophozoite and cyst. Both the forms occur in infected tissue . the nuclear characteristic of trophozoite are similar to that of Naegleria fowleri . they produce fine, tapering , hyaline pseudopodia called acanthopodia . motility is sluggish . A flagellate stage is absent and the cyst have double wall , the inner wall is smooth and the outer is wrinkled and and ragged . the cyst survive in dust for many years.
Life cycle , pathology and clinical features :
Acanthameoba occur in soil and water . trophozoite and cysts are infective to human beings. The infection is through contaminated traumatized skin or eyes and by inhalation . in primary infection the skin and lungs are involved . heamatophagous spread from these sites leads to involvement of the CNS producing granulomatous amoebic encephalitis (GAE) .patient with lymphoproliferative disease , lupus erythromatous , AIDS and those on glucococorticoids or chemotherapy are at an increased risk . GAE usually present as space – occupying lesion. Rarely, the cysts of Acanthamoeba rapidly transform into trophozoite in the nasal mucosa to reach brain through the cribriform plate along the olfactory nerve and may lead to meningoencephalitis .
Acanthameoba can produce keratitis . contact – lens users are at increase risk . risk factors include the use of home- made saline for clearing lenses , wearing lenses while swimming and inadequate disinfection . deeper corneal invasion with perforation and lose of vision may follow Acanthameoba keratitis.
Diagnosis :
examination of CSF for trophozoite may be helpful. The cyst of Acanthameoba are present in corneal scraping .
Treatment :
No satisfactory treatment is available for GAE . cases of Acanthameoba keratitis respond to a combination of neomycin drops, dibromopropamide ointment and propamide isethionate drops .
Prevention :
Prevention of CNS infection by Acanthameoba if difficult because the life cycle is poorly understood . removing contact-lenses and proper cleaning and disinfection of lenses prevent eye infection.
Class (2) : The Flagellated Protozoa
The flagellates are members of subphylum mastigophora and have the following characters:
they move with the help of flagellum or flagella .
reproduction is by binary fission .
Flagellates of medical importance :
Flagellata includes three basic group and classified according to their location in the body of the host :
Intestinal species
Giardia lamblia
Trichomonas hominis
Chilomastix mesnili
Enteromonas hominis
Retortamonas intestinalis
Oral and vaginal species .
Trichomonas tenax
Trichomonas vaginalis
Blood species
Leishmania donovani
Leishmania tropica
Leishmania brazielinses
Trypanosoma cruzi
Trypanosoma gambiense
Trypanosoma rhodesience
Giardia lamblia
The infection of Giardia lamblia is world wide and it is more common in children . Giardia lamblia, a protozoan flagellate, inhabits (duodenum and jejunum) of man. This protozoan is the only intestinal flagellate known to endemic and epidemic diarrhea in man.
Morphology :
Giardia lamblia has a trophozoite and cystic stage.
Trophozoite stage : It is pear-shaped with broad rounded anterior end and a tapering posterior end. Dorsal surface is convex while ventral surface is concave .A sucking disc, the organ of attachment because presence of Giardin protein, occupies one-third to one-half of the ventral surface. Trophozoite is bilaterally symmetrical and has two nuclei, axostyle and four pairs of flagella. Two median bodies are present on the axostyle at its origin.
Cyst : the oval cyst measuring 8-12μm in length and 7-10μm in breath . A thick wall surrounds it. The cyst consists of cytoplasm, which is finely granular and is separated from the cyst wall by a clear space. This gives an appearance of the cyst being surrounded by a halo. The mature cyst consists four nuclei, which may remain clustered at one end or are present in pairs at two opposite ends. Also it consists of an axostyle and margins of the sucking disc. The axostyle and the remains of flagellum is placed diagonally in the cyst. The four nuclei cyst is the infective stage of G. lamblia..
life cycle :
The life cycle of G. lamblia is simple and is completed in a single host, the man .Cysts are resistant forms and are responsible for transmission of giardiasis. The cysts are hardy, can survive several months in cold water. Infection occurs by the ingestion of cysts in contaminated water, food, or by the fecal-oral route (hands or fomites). Cysts pass through the stomach and excyst to trophozoites in the duodenum within 30 minutes of ingestion, Excystation process is trigged by exposure of the cysts to pancreatic enzymes . In duodenum and jejunum, the trophozoite multiply asexually by binary fission thereby producing a large numbers of daughter trophozoites. Trophozoites browse on the mucosal surface, to which they are attached by an oval sucker. When the intestinal contents leave the jejunum and begin to lose moisture, the trophozoites retract their flagella, cover themselves with a thick wall and encyst. These encysted trophozoites undergo another phase of nuclear division and produce four nucleated mature cysts. The four nucleated mature cysts are the infective forms of the parasites, they are excreted in stool and the cycle is repeated. trophozoites may be present in stool of patient with diarrhea but they are not infective.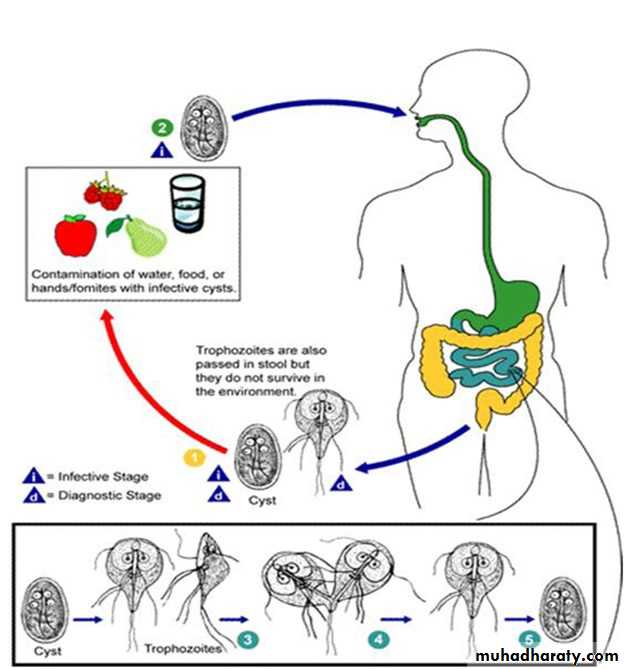
Pathology and symptoms:-
Giardia lamblia causes Giadiasis (steatorroea or fatty diarrhea). A great majority of persons harboring Giardia lamblia are asymptomatic but some have symptoms referable to the duodenum and a few to the gallbladder , in which the only plausible etiology is the infection with Giardia . Although this flagellate does not invade tissues , it causes intestinal malabsorption of fat and carbohydrates, steatorroea and weight loss by forming a tightly attached , pavement –like sheet of trophozoite over the mucosal surface . The most common symptoms in these cases are epigastric or right upper quadrant pain and persistent fatty diarrhea.Diagnosis , treatment and prevention:-
The gold – standard diagnosis for Giardia lamblia is microscopic demonstration of the trophozoite , cyst or both in stool . in acute Giardiasis the trophozoite show the typical falling leaf motility in wet mount examination of stool . Trophozoites may also be obtained by duodenal aspiration.
In at least 90 % of cases the infection is eradicated following quinacrine (Atabrine) therapy . Metronidazole is nearly as effective and is somewhat better tolerated . The adult dose is 250 mg .t.i.d. for 5 to 10 days.
Infection with Giardia lamblia is prevented by not eating or drinking contaminated food and water , respectively . Adequate cooking of contaminated food and boiling or filtering contaminated water , prevent infection.
Species of Trichomonas
These flagellates have the following common characteristic in their trophozoite stage :
a rounded anterior and a somewhat pointed posterior end .
a semi- rigid translucent rod-like axostyle which arises near the median anterior pole and extends through the entire body .
a small cytostome on one side of the anterior end .
3 to 5 free flagella arise from the anterior end and an additional marginal flagellum on an undulating membrane , which spirals down the sides of the body .
Multiplication is by longitudinal binary fission.
Trophozoites are described only for those species that parasitize man.
Three distinct species of Trichomonas are adapted to the human host . The species which occur in man are: T. hominis, T. tenax and T. vaginalis. Although they closely resemble one another they are morphologically different, develop in different locations and are reciprocally not transplantable.
Trichomonas hominis:-
Trichomonas hominis has a cosmopolitan distribution. It inhabit the lumen of the caecum .
Trichomonas tenax:-
Trichomonas tenax is probably a cosmopolitan parasite of man . On the average Trichomonas tenax is smaller than T. hominis. The normal habitat is the mouth, particularly in diseased gums, in tartar around the teeth and in carious teeth. It is not pathogenic but its presence indicates poor oral hygiene.
Trichomonas vaginalis :
Trichomonas vaginalis, a flagellate, is the most common pathogenic protozoan of humans in industrialized and developing countries. It causes trichomoniasis. The infection is transmitted sexually (STD) .
Morphology :
Trichomonas vaginalis only exists in trophozoite stage and multiplies by longitudinal binary fission. Cystic stage is absent. Trophozoite inhabit the vagina in female, the prostate and seminal vesicles in male and urethra in both sexes. The trophozoites of Trichomonas, measuring 14-17μm×5-15μm have a single nucleus and a large sausage – shaped parabasal body, four anterior flagella and a single lateral flagellum attached to pellicle to form an undulating membrane . They are actively motile, pear-shaped. The inner margin of this membrane is supported by a filament. There is also a central skeletal rod or axostyle. The cytoplasm contains a large numbers of hydrogenosomes and sometimes viral particles. Trophozoite of Trichomonas vaginalis is facultative anaerobic. It is identified by its characteristic twitching motility. Trophozoite is the infective form of the parasite.
Life cycle :
Life cycle of Trichomonas vaginalis is simple. It is completed in a single host either male or female Trichomonas vaginalis resides in the female lower genital tract and the male urethra and prostate, where it replicates by binary fission. The parasite does not appear to have a cyst form, and does not survive well in the external environment. Trichomonas vaginalis is transmitted among humans, its only known host, primarily by sexual intercourse.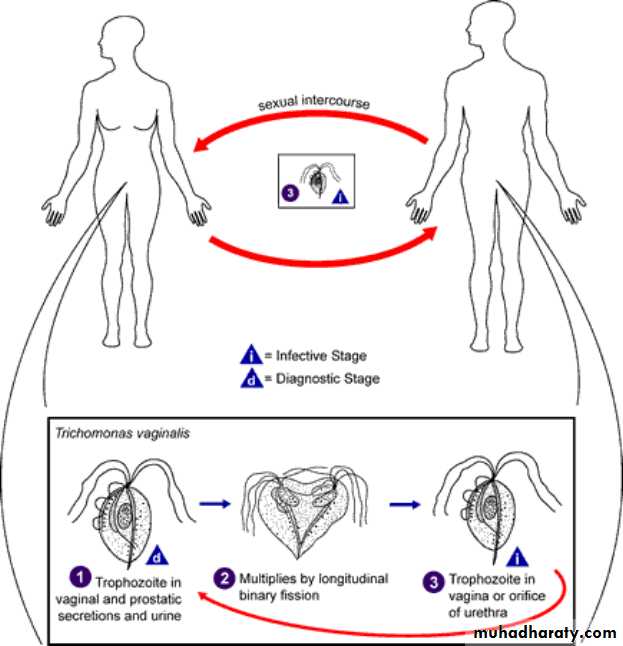
Transmission of T. vaginalis :
Trichomoniasis probably is the most common sexually transmit disease (STD) worldwide. Infected women harbouring T. vaginalis in the genital tract and infected men are the chief reservoir of infection. Trophozoite is the infective stage The infection may be transmitted venereally by sexual contact with infected person, also to babies during passage through an infected birth canal, and occasionally non-venereally through fomites such as towels, toilet seats, etc., and also through mud and water bath as well.Pathology & clinical features :
Trichomonas vaginalis infection in the male is often asymptomatic although at times it is associated with urethritis . In the female the propagation of this organism in the vagina may be symptomless , it may produce a characteristic type of vaginitis or it may be complicated by bacterial, fungous or spirochetal infection. There is definite evidence that time at Trichomonas vaginalis is at least an important contributor to a distance type of vaginitis characterized by leucorrhea , pruritus vaginae and vulvae , burning of the vagina and vulva or dysuria, and chafing of the vulva . The ph of the vaginal discharge in these symptomatic infections is typically alkaline as distinguished from the slightly acid condition of the normal vagina. The symptoms vary from mild to almost intolerable pruritus but the disease is more annoying than disabling .
DIAGNOSIS
The specific diagnosis of trichomoniasis is made by demonstration of organisms (a jerky motile trophozoites) in the genital specimens and also in the urine by microscopy. Microscopic examination of wet mounts may establish the diagnosis by detecting actively motile organisms. This is the most practical and rapid method of diagnosis (allowing immediate treatment). women, examination should be performed on highly vaginal swab (HVS) and urethral secretions. In men, anterior urethral or prostatic secretions should be examined. PCR also useful .
Treatment
Treatment should be implemented under medical supervision, and should include all sexual partners of the infected persons. The drug of choice for treatment is metronidazole therapy is usually highly successful. Tinidazole, which is a better-tolerated alternative drug.
Preventive measures
1) Detection and treatment of cases either male or female.
2) Avoidance of sexual contact with infected partners, and
3) Use of condoms.