Fifth Stage
Internal Medicine
Dr. Abbas / Lec . 1
1
Nervous system
The anatomy
The nervous system consists of the brain and spinal cord [central nervous
systm[C.N.S] and peripheral nerves and muscles [peripheral nervous system [P.N.S].
▪
The neurone has a cell body and axon terminating at a synapse and is the
functioning unit of the nervous system
▪
Astrocytes provide the structural framework for for the neurones,control their
biochmical environment and form blood-brain barrier.
▪
Micrglail cell are blood-derived mononuclear macrphage and have immune role.
▪
Inthe C.N.S,oligodendrocytes createe and mentain amyelin sheath round the axon
while in the P.N.S the myelin sheath is produced by Schwann cells.
The brain consists of two cerebral hemispheres each with four functionally
specialized lobes [frontal,parietal,temporal and occipital] ,the brainstem and cerebellum
The cerebral cortex over the cerebral hemispheres constitutes the highest
level of function
The cerebral cortex constitutes the highest level of nervous function, the anterior half
dealing with executive ('doing') functions and the posterior half constructing a
perception of the environment ('receiving and perceiving'). and which of the two
hemispheres is 'dominant', i.e. where language function is represented. In right-handed
individuals this is almost always the left hemisphere while in left-handers either
hemisphere may be dominant with about equal frequency .
The brainstem consist of the midbrain,pons and medulla oblongata,contains
all sensory and motor pathways entering and leaving the cerebral
hemispheres ,together with nuclei of the cranial nerves
The cerebellum which lies below cerebral hemispheres and posterior to the
brainstem,is responsible for co-ordination including gait and posture.
Between the soft brain and the skull are three types of membranous covering called
meninges
▪
The dura mater next to the bone
▪
The arachnoid in mmiddle
▪
The pia mater next to the brain
Tentorium cerebelli divide the brain into two levels
Supratentorail level
&
infratentorail level
2
The spinal cord
▪
The spinal cord is 18 in (45 cm) long. It is continuous above with the medulla
oblingata at the level of the foramen magnum and ends below at the lower
level of the 1st, or the upper level of the 2nd lumbar vertebra.
▪
Tapers into the conus medullaris from which a prolongation of pia mater.
▪
At each intervertebral foramen the anterior and posterior nerve roots unite to
form a spinal nerve which immediately divides into its anterior and
▪
posterior primary rami, each transmitting both motor and sensory fibres.
NEUROLOGICAL INVESTIGATIONS NEURORADIOLOGY
Skull X-rays
▪
fractures of the skull vault or base
▪
skull lesions (e.g. metastases, osteomyelitis, Paget's disease, abnormal skull
foramina, fibrous dysplasia)
▪
enlargement or destruction of the pituitary fossa - intrasellar tumour, raised
intracranial pressure
▪
Spinal X-rays show fractures, congenital bone lesions (e.g. cysts), destructive
lesions (infection, metastasis) or spondylosis (degenerative change .)
Imaging of the brain and spinal cord :Brain CT is now widely available world-wide
and MRI is rapidly becoming a standard test
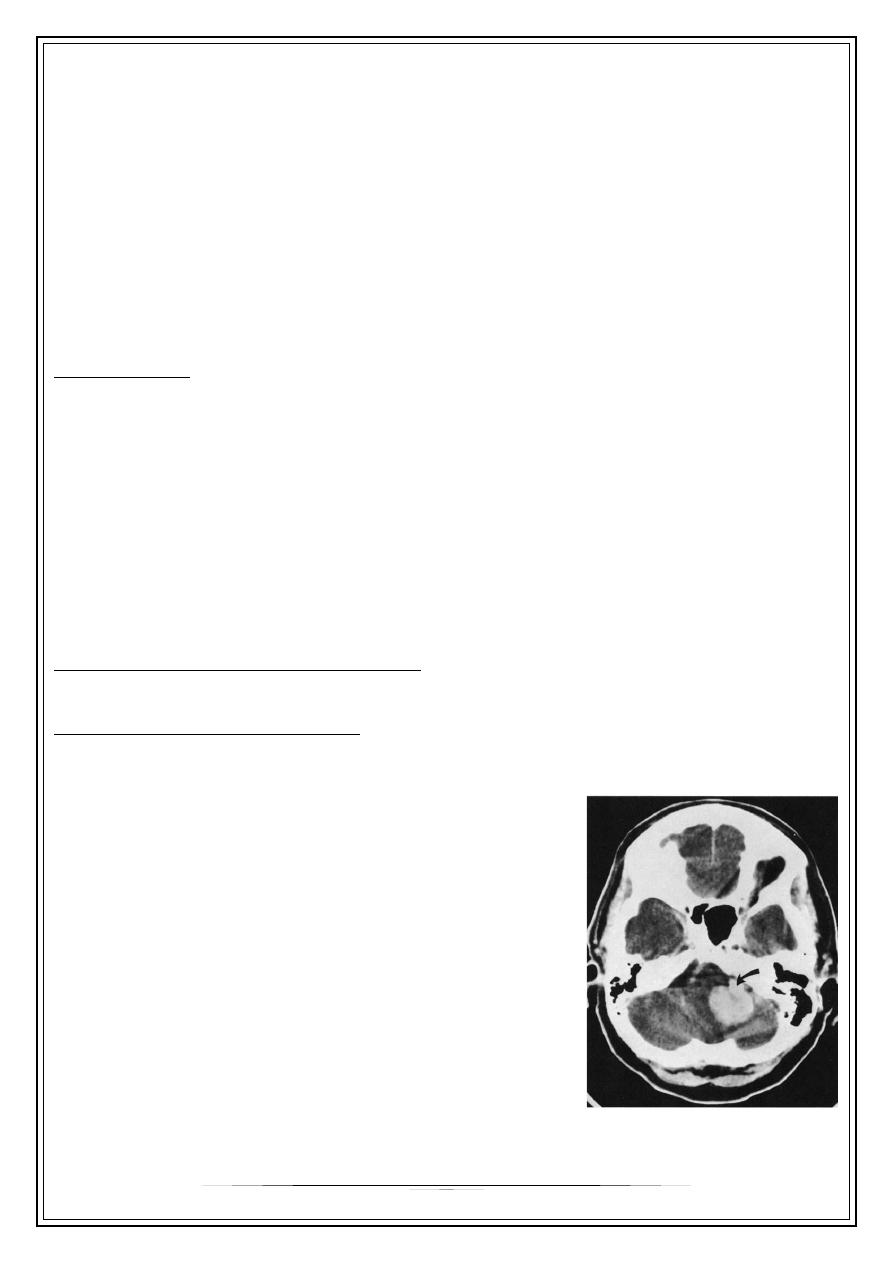
Computed tomography: CT
▪
A collimated X-ray beam moves synchronously across a slice of brain between 2
mm and 13 mm thick.
▪
attenuation (density) between bone, brain and CSF
enable recognition of normal and infarcted tissue,
tumour, extravasated blood, and oedema
.
Enhancement with i.v. contrast media
delineates areas of increased blood supply. CT
imaging of the spinal cord (myelography) and
cerebral ventricles (ventriculography) is occasionally
performed
▪
CT is safe apart from occasional systemic
reactions to contrast; the irradiation involved
is small.
3
CT scanning demonstrates :
▪
cerebral tumours
▪
intracerebral haemorrhage and infarction
▪
subdural and extradural haematoma
▪
free blood in the subarachnoid space (subarachnoid haemorrhage)
▪
lateral shift of midline structures and displacement/enlargement of the ventricular
system
▪
cerebral atrophy
▪
spinal trauma (with CT myelography(
▪
skull and scalp lesions .
▪
CT imaging, within its limitations, shows that the brain is anatomically normal, and
gives reassurance .
Limitations of CT
▪
Lesions under 1 cm diameter may be missed .
▪
Lesions with attenuation close to that of bone may be missed if near the skull .
▪
Lesions with attenuation similar to that of brain are poorly imaged (e.g. MS
plaques, isodense subdural haematoma(
▪
CT sometimes misses lesions within the posterior fossa .
▪
The spinal cord is not imaged directly by CT (contrast is necessary).
▪
Cooperation is required - a general anaesthetic is occasionally needed .
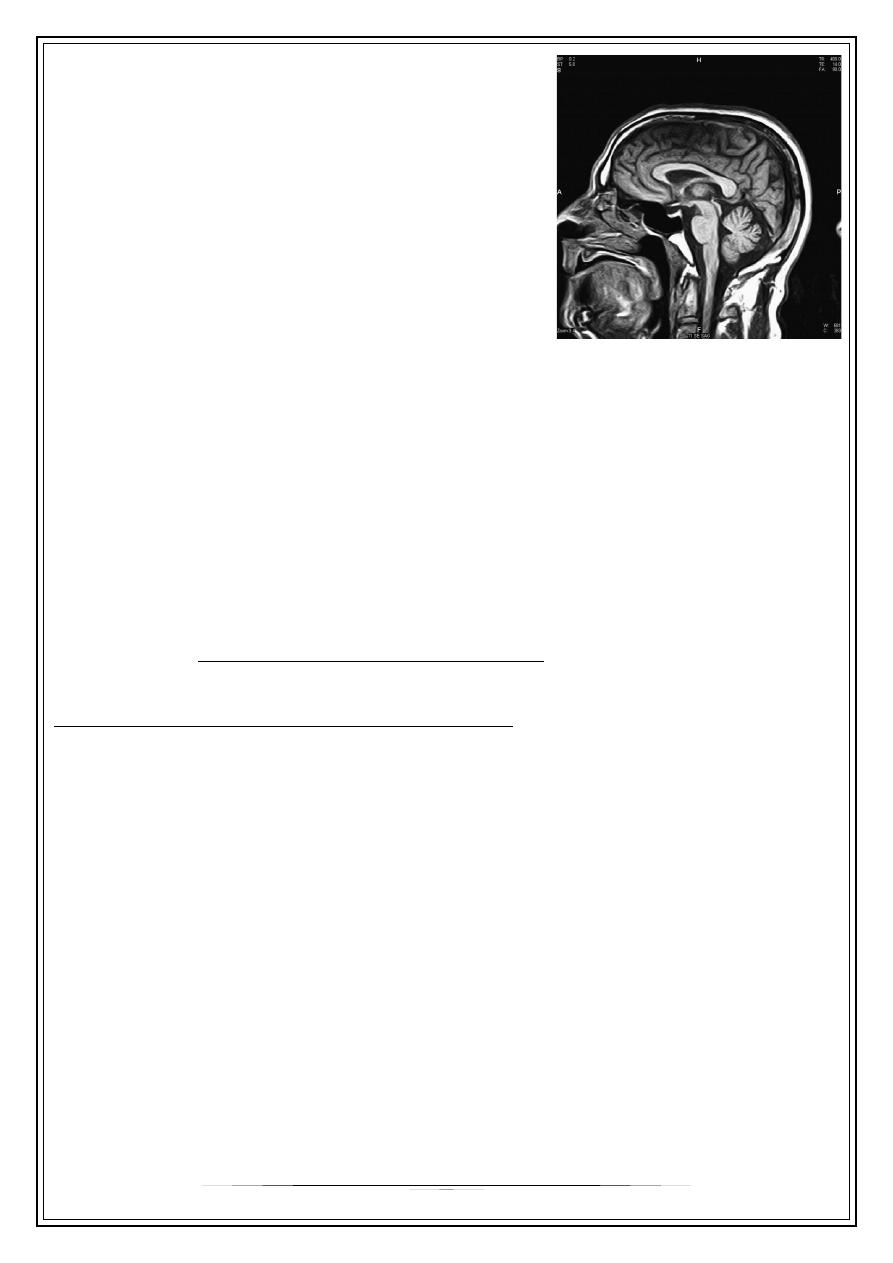
Magnetic resonance imaging: MRI
▪
The hydrogen nucleus is a proton whose electrical charge creates a local electrical
field. These protons are aligned by sudden strong magnetic impulses. Protons are
then imaged with radiofrequency waves at right angles to their alignment. The
protons resonate and spin, then revert to their normal alignment. As they do so,
images are made at different phases of relaxation, known as T1, T2, T2 'STIR',
diffusion-weighted imaging (DWI) and other sequences. Gadolinium is used as an
intravenous contrast medium .
Advantages of MRI
▪
MR distinguishes between brain white and grey matter .
4
▪
Spinal cord and nerve roots are imaged directly .
▪
Pituitary imaging .
▪
MRI has greater resolution than CT (around 0.5
cm(
▪
No radiation is involved .
▪
Magnetic resonance angiography (MRA) images
blood vessels without contrast .
▪
It is useful in muscle disease, e.g. myositis .
Limitations of MRI are principally
▪
time and cost. Imaging one region takes about 20 minutes.
▪
Patients do need to cooperate.
▪
Claustrophobia is an issue but 'open' machines are available.
▪
Patients with pacemakers or with metallic bodies in the brain cannot be imaged.
▪
MR imaging for some days after lumbar puncture frequently shows diffuse
meningeal enhancement with gadolinium .
Doppler studies
B-mode and colour ultrasound
are valuable in the detection of
stenosis of the carotid arteries
Digital cerebral and spinal angiography,
These techniques are little used. Contrast is injected intra-arterially or intravenously.
These studies carry a mortality and risk of stroke (<1%). Sequences of the aorta, carotid
and vertebral arteries demonstrate occlusion, stenoses, atheroma and aneurysms.
Spinal angiography images cord arteriovenous malformations .
Isotope bone scanning
▪
[99mTc]-pertechnetate is injected intravenously, is of value in detection of vertebral
and skull lesions (e.g. metastases(
▪
Positron emission tomography (PET) and single proton emission
computed tomography (SPECT) These techniques image function more than
anatomy by tracking the uptake and metabolism of radioisotopes
To be continued,,,