L6 12 JAN 2021
الدكتورضياء كاظم الوائلي
شهادة الاختصاص الدقيق في السكري والغدد الصماء
شهادة البورد (الدكتوراه) للامراض الباطنيه والقلبيه والصدريه
عضو الجمعيه الامريكيه للسكري والغدد الصماء
عضو الهيئة التدريسية في كلية الطب - جامعة ذ ي قار
Hydroxycobalamin (vitamin B12)
Vitamin B12 is a co-factor in folate co-enzyme recycling and nerve myelination. Vitamin B12 and folate are particularly important in DNA synthesis in red blood cells.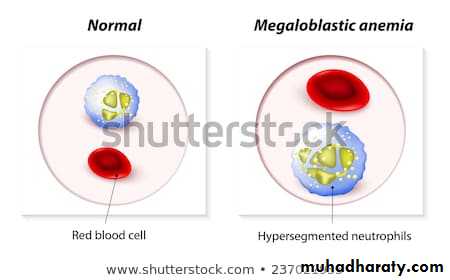
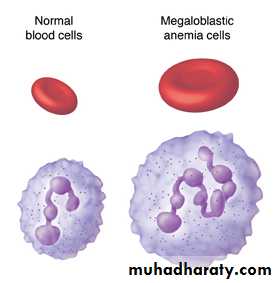
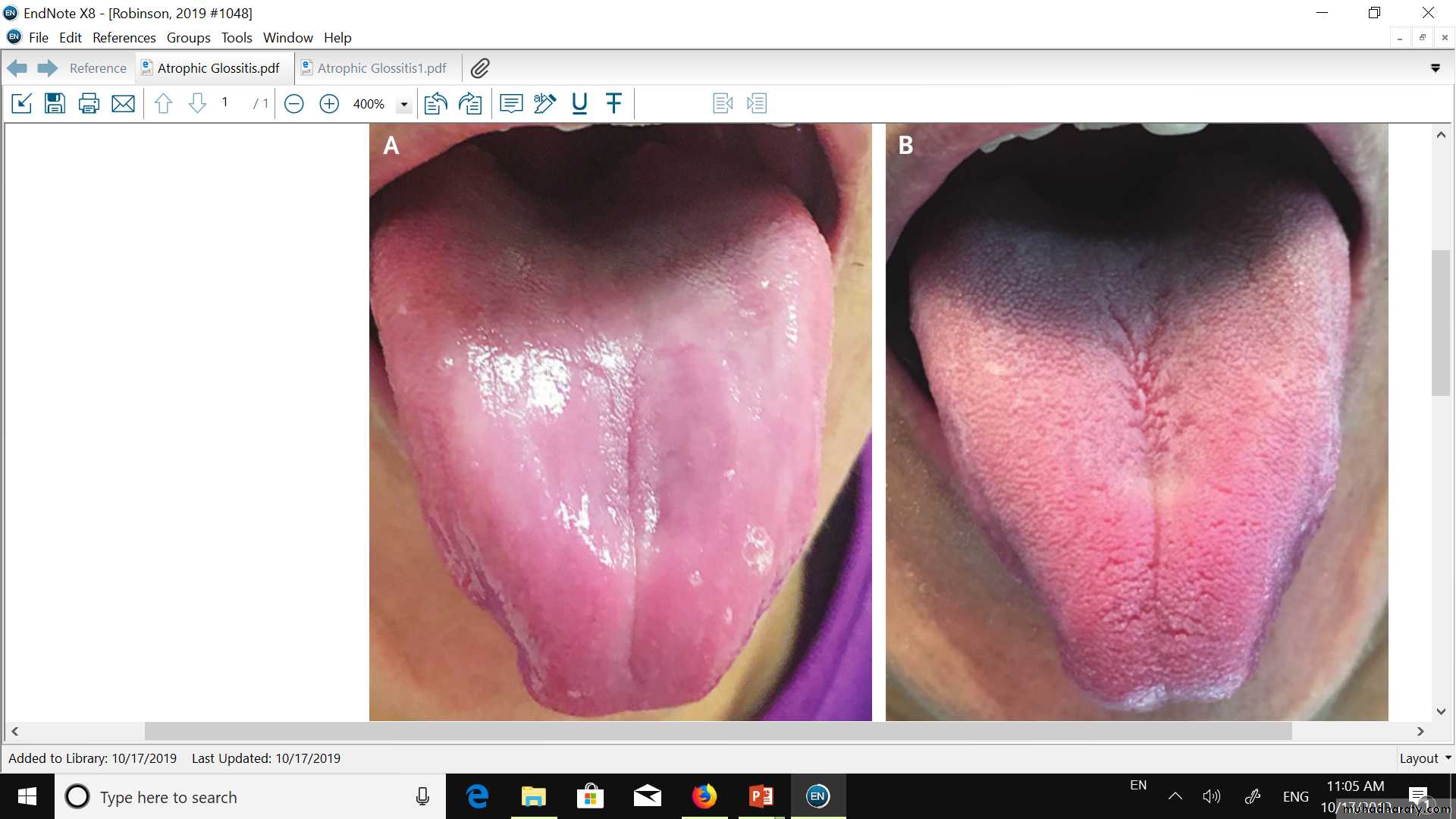
MEGALOBLASTIC ANEMIA
Vitamin B12 , but not folate, is needed for the integrity of myelin, so that vitamin B12
deficiency is also associated with neurological diseaseNeurological disease
• Neurological findings in B12
• Peripheral nerves• • Glove and stocking paraesthesiae
• • Loss of ankle reflexes
• Spinal cord
• Subacute combined degeneration of the cord
• Posterior columns – diminished vibration sensation and proprioception
• Corticospinal tracts – upper motor neuron signs
• Cerebrum
• • Dementia
• • Optic atrophy
• Autonomic neuropathy deficiency
• Neurological consequences of vitamin B12
• In older people and chronic alcoholics, vitamin B12 deficiency arises from insufficient intake and/or from malabsorption.
• Several drugs, including neomycin, can render vitamin B12 inactive.
• Adequate intake of folate maintains erythropoiesis and there is a concern that fortification of foods with folate may mask underlying vitamin B12
• deficiency.
• In severe deficiency there is insidious, diffuse and uneven demyelination. It may be clinically manifest as peripheral neuropathy or spinal cord degeneration affecting both posterior and lateral columns (‘subacute combined degeneration of the spinal cord), or there may be cerebral manifestations (resembling dementia) or optic atrophy.
• Vitamin B12 therapy improves symptoms in most cases.

Vitamin C (ascorbic acid)
• Vitamin C (ascorbic acid)• Ascorbic acid is the most active reducing agent in the aqueous phase of living tissues and is involved in intracellular electron transfer.
• It takes part in the hydroxylation of proline and lysine in protocollagen to hydroxyproline and hydroxylysine in mature collagen.
• It is very easily destroyed by heat, increased pH and light, and is very soluble in water; hence many traditional cooking methods reduce or eliminate it.
• Claims that high-dose vitamin C improves immune function (including resistance to the common cold) and cholesterol turnover remain unsubstantiated.
• Deficiency – scurvy
• Vitamin C deficiency causes defective formation of collagen with:-• Impaired healing of wounds
• Capillary haemorrhage
• Reduced platelet adhesiveness (normal platelets are rich in ascorbate)
• Scurvy – vitamin C deficiency precipitating factors:-
• Increased requirement• • Trauma, surgery, burns, infections
• • Smoking
• • Drugs (glucocorticoids, aspirin, indometacin, tetracycline)
• Dietary deficiency
• • Lack of dietary fruit and vegetables for > 2 months
• • Infants fed exclusively on boiled milk
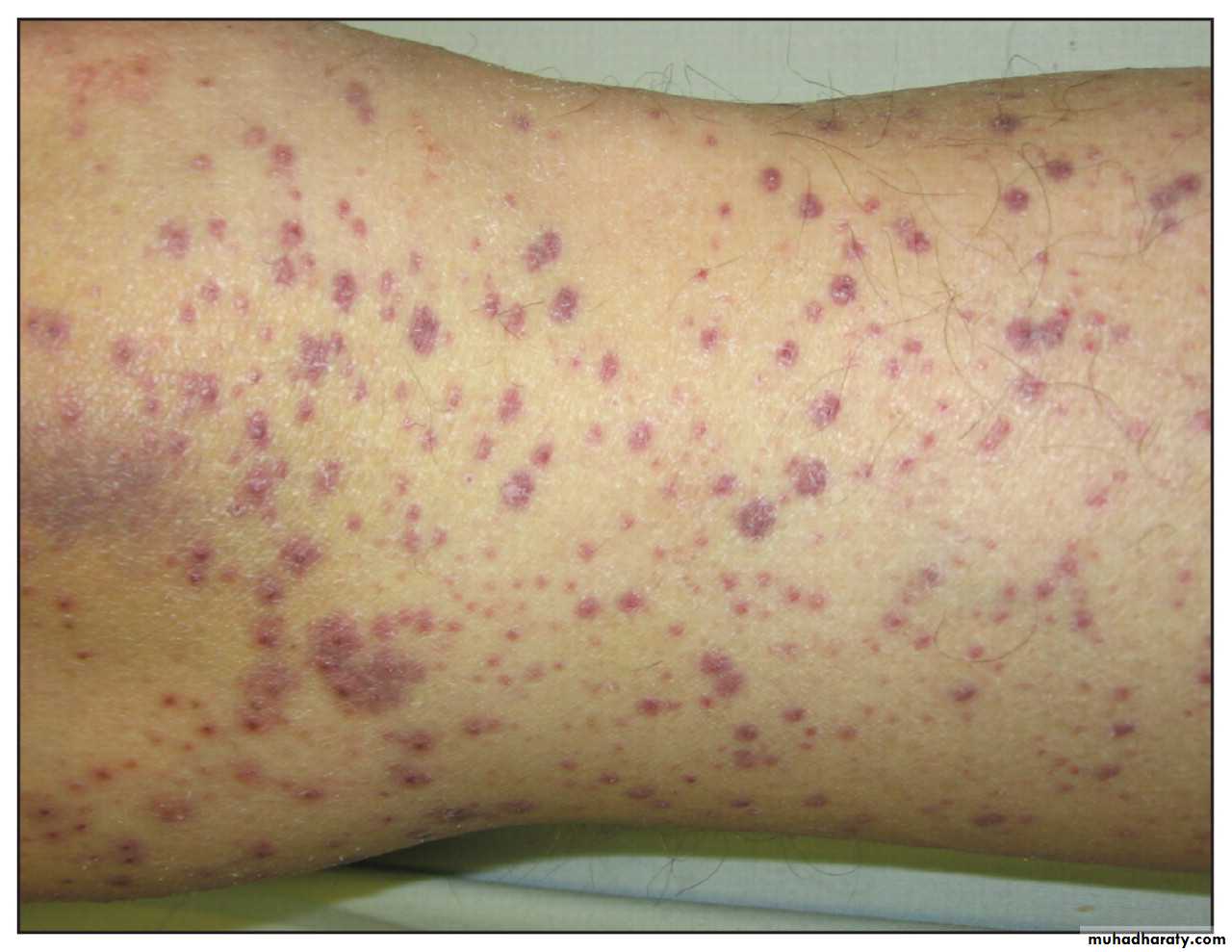
• Clinical features of scurvey
• • Swollen gums that bleed easily• • Perifollicular and petechial haemorrhages
• • Ecchymoses
• • Haemarthrosis
• • Gastrointestinal bleeding (GIT bleeding)
• • Anaemia
• • Poor wound healing

• Perifollicular hyperkeratosis
• A dose of 250 mg vitamin C 3 times daily by mouth should saturate the tissues quickly.
• The deficiencies of the patient’s diet also need to be corrected and other vitamin supplements given if necessary.• Daily intakes of more than 1 g/day have been reported to cause diarrhoea and the formation of renal oxalate stones.
• Other dietary organic compounds
• There are a number of non-essential organic compounds with purported health benefits, such as reducing risk of heart disease or cancer.• Groups of compounds such as the flavonoids and phytoestrogens show bioactivity through their respective antioxidant and oestrogenic or anti-oestrogenic activities.
• Flavonoids (of which there are a number of different classes of compound) are found in fruit and vegetables, tea and wine; phytoestrogens are found in soy products (with higher intakes in parts of Asia compared to Europe and the USA) and pulses.
• Caffeine from tea and coffee and carbonated beverages affects the nervous system and can improve mental performance in the short term, with adverse effects seen at higher intakes.
• Intake of non-carbonic organic acids (which are not metabolised to carbon dioxide), e.g. oxalates, may be restricted in individuals prone to kidney stones.
• Inorganic micronutrients
• A number of inorganic elements are essential dietary constituents for humans.
• Deficiency is seen when there is inadequate dietary intake of minerals or excessive loss from the body.
• Toxic effects have also been observed from self
• medication and disordered absorption or excretion.).
• Examples of clinical toxicity include excess of :-
• Iron (haemochromatosis or haemosiderosis),• Fluoride (fluorosis),
• Copper (Wilson’s disease) and
• Selenium (selenosis, seen in parts of China
• For most minerals, the available biochemical markers do not accurately reflect dietary intake and dietary assessment is required.
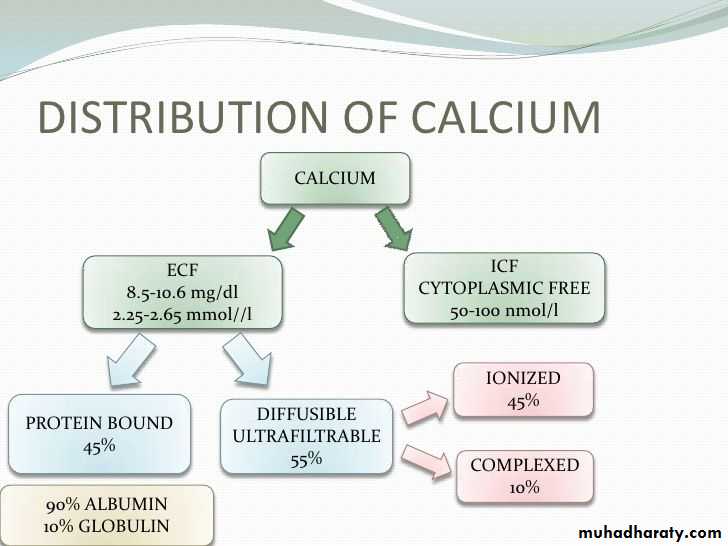
• Calcium is the most abundant cation in the body and powerful homeostatic mechanisms control circulating ionised calcium levels.
• Calcium and phosphorus


• The WHO’s dietary guidelines for calcium differ between countries, with higher intakes usually recommended in places with higher fracture prevalence.
• Between 20% and 30% of calcium in the diet is absorbed, depending on vitamin D status and food source.
• Calcium requirements depend on phosphorus intakes, with an optimum molar ratio (Ca:P) of 1 : 1.
• Excessive phosphorus intakes (e.g. 1–1.5 g/day) with a Ca:P of 1 : 3 have been shown to cause hypocalcaemia and secondary hyperparathyroidism.
• Calcium absorption may be impaired in vitamin D deficiency and in malabsorption secondary to small intestinal disease.
• Calcium deficiency causes impaired bone mineralisation and can lead to osteomalacia in adults. Too much calcium can lead to constipation, and toxicity has been observed in ‘milk-alkali syndrome’.
• Dietary deficiency of phosphorus is rare (except in older people with limited diets) because it is present in nearly all foods and phosphates are added to a number of processed foods.
• Phosphate deficiency in adults occurs:
• • In patients with renal tubular phosphate loss
• • In patients receiving a prolonged high dosage of aluminium hydroxide.
• • In alcoholics sometimes when they are fed with high carbohydrate foods
• • In patients receiving parenteral nutrition if inadequate phosphate is provided.
• Deficiency causes hypophosphataemia and muscle weakness secondary to ATP deficiency.
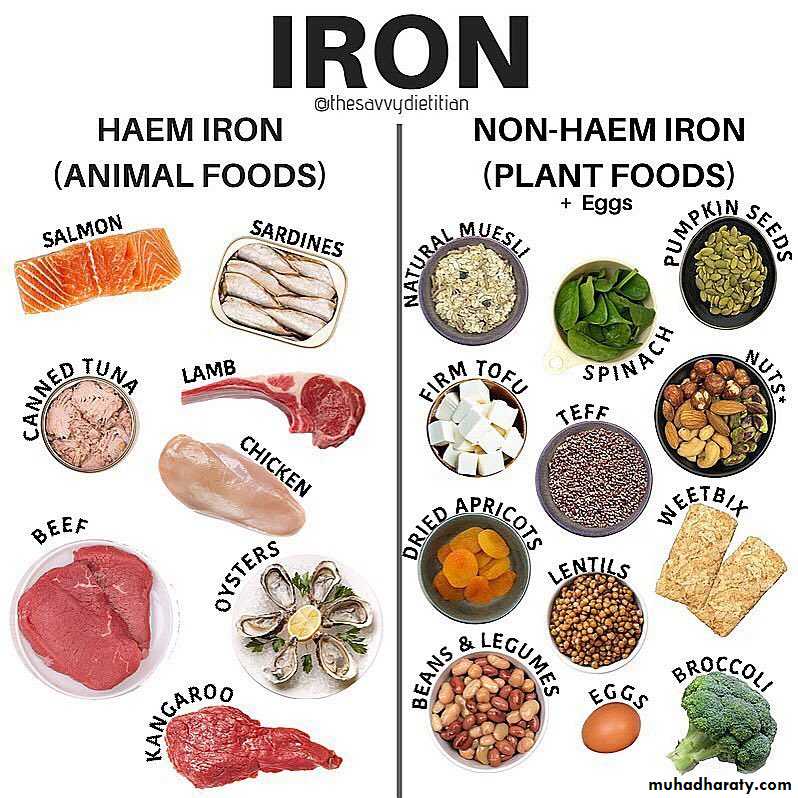
Iron



• Non-haem iron in cereals and vegetables is poorly absorbed but makes the greater contribution to overall intake, compared to the well-absorbed haem iron from animal products.
• Iron
• Iron is involved in the synthesis of haemoglobin and is required for the transport of electrons within cells and for a number of enzyme reactions
• Fruits and vegetables containing vitamin C enhance iron absorption, while the tannins in tea reduce it.
• Dietary calcium reduces iron uptake from the same meal, which may precipitate iron deficiency in those with borderline iron stores.
• There is no physiological mechanism for excretion of iron, so homeostasis depends on the regulation of iron absorption.
• This is regulated at the level of duodenal enterocytes by hepcidin (a peptide secreted by hepatocytes in the duodenum).
• The expression of hepcidin is suppressed when body iron is low, leading to enhanced efflux of iron into the circulation.
• The normal daily loss of iron is 1 mg, arising from desquamated surface cells and intestinal losses.
• A regular loss of only 2 mL of blood per day doubles the iron requirement.
• On average, an additional 20 mg of iron is lost during menstruation, so pre-menopausal women require about twice as much iron as men (and more if menstrual losses are heavy).• The major consequence of iron deficiency is anaemia.
• This is one of the most important nutritional causes of ill health in all parts of the world.• In the UK, it is estimated that 10% women are iron-deficient.
• Dietary iron overload is occasionally observed and results in iron accumulation in the liver and, rarely,
• cirrhosis.
• Haemochromatosis results from an inherited increase
• in iron absorption.
Iodine
• Iodine
• Iodine is required for synthesis of thyroid hormones.• It is present in sea fish, seaweed and most plant foods grown near the sea.
• The amount of iodine in soil and water influences
• the iodine content of most foods.
• Iodine is lacking in the highest mountainous areas of the world (e.g. the Alps and the Himalayas) and in the soil of frequently flooded plains (e.g. Bangladesh).
• About a billion people in the world are estimated to have an inadequate iodine intake and hence are at risk of iodine deficienc disorder.
• Goitre is the most common manifestation, affecting about 200 million people (p. 648).
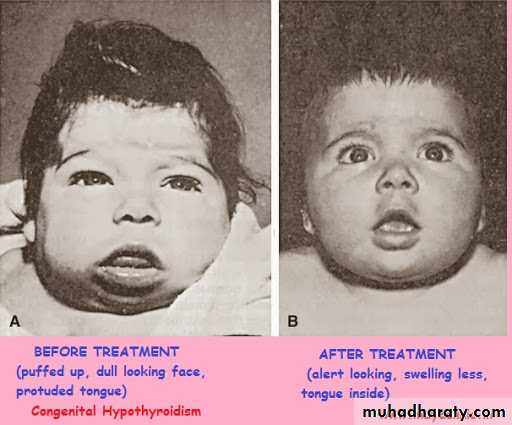
• In those areas where most women have endemic goitre, 1% or more of babies are born with cretinism (characterised by mental and physical retardation).
• There is a higher than usual prevalence of deafness, slowed reflexes and poor learning in the remaining population. The best way of preventing neonatal cretinism is to ensure adequate levels of iodine during pregnancy. This can be achieved by intramuscular injections with 1–2 mL of iodised poppy seed oil (475–950 mg iodine) to women of child-bearing age every 3–5 years, by administration of iodised oil orally at 6-monthly or yearly intervals to adults and children,
• or by provision of iodised salt for cooking.
• Zinc
• Zinc is present in most foods of vegetable and animal origin. It is an essential component of many enzymes, including carbonic anhydrase, alcohol dehydrogenase and alkaline phosphatase.• Acute zinc deficiency has been reported in patients receiving prolonged zinc-free parenteral nutrition and causes diarrhoea, mental apathy, a moist, eczematoid dermatitis, especially around the mouth, and loss of hair.

• Chronic zinc deficiency occurs in dietary deficiency, malabsorption syndromes, alcoholism and its associated hepatic cirrhosis.
• It causes the clinical features seen in the very rare congenital disorder known as acrodermatitis enteropathica (growth retardation, hair loss and chronic diarrhoea).
• Zinc deficiency is thought to be responsible for one-third of the world’s population not reaching their optimal height..



• In the Middle East, chronic deficiency has been associated with dwarfism and hypogonadism.
• In starvation, zinc deficiency causes thymic atrophy; zinc supplements may accelerate the healing of skin lesions, promote general well-being, improve appetite and reduce the morbidity associated with the under-nourished state, and lower the mortality associated with diarrhoea and
• pneumonia in children

Selenium
• Selenium• The family of seleno-enzymes includes glutathione peroxidase, which helps prevent free radical damage to cells, and mono-deiodinase, which converts thyroxine to triiodothyronine.
• North American soil has a higher selenium content than European and Asian soil, and the decreasing reliance of Europe on imported American food in recent decades has resulted in a decline in dietary selenium intake.
• Selenium deficiency can cause hypothyroidism, cardiomyopathy in children (Keshan’s disease) and myopathy in adults.
• Excess selenium can cause heart disease.

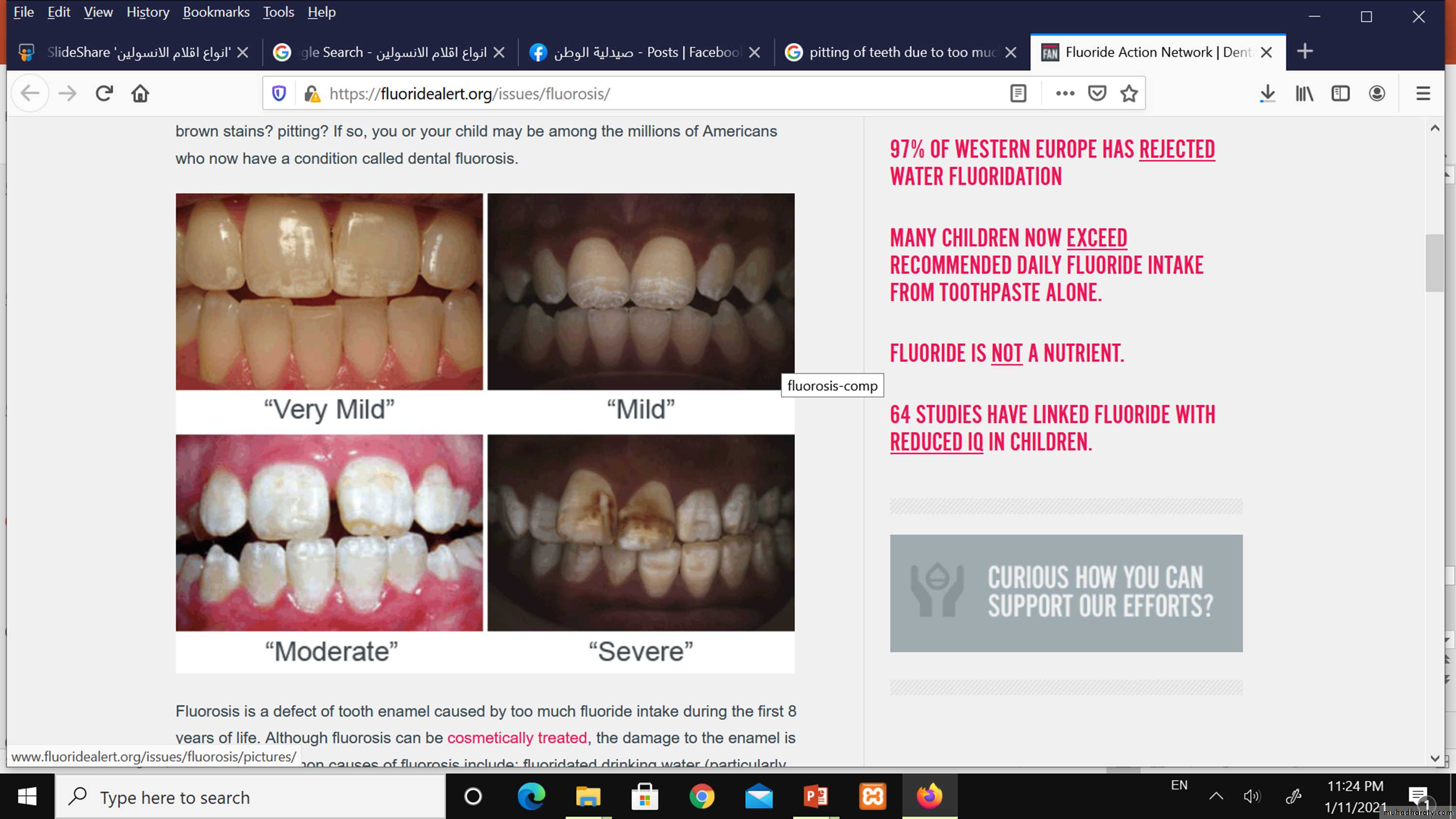
• Fluoride helps prevent dental caries because it increases the resistance of the enamel to acid attack.
• It is a component of bone mineral and some studies have shown anti-fracture effects at low doses, but excessive intakes may compromise bone structure.
• If the local water supply contains more than 1 part per million (ppm) of fluoride, the incidence of dental caries is low.
Fluoride
• Soft waters usually contain no fluoride, while very hard waters may contain over 10 ppm.
• The benefit of fluoride is greatest when it is taken before the permanent teeth erupt, while their enamels being laid down.
• The addition of traces of fluoride (at 1 ppm) to public water supplies is now a widespread practice. Chronic fluoride poisoning is occasionally seen where the water supply contains > 10 ppm fluoride..
• It can also occur in workers handling cryolite (aluminium sodium fluoride), used in smelting aluminium.
• Pitting of teeth is a result of too much fluoride as a child

• Sodium, potassium and magnesium
• Western diets are high in sodium due to the sodium chloride (salt) that is added to processed food.• In the UK, it is suggested that daily salt intakes are kept well below 6 g.
• Other essential inorganic nutrients
• These include chloride (a counter-ion to sodium and potassium), cobalt (required for vitamin B12),• sulphur (a constituent of methionine and cysteine), manganese (needed for or activates many enzymes) and chromium (necessary for insulin action). Deficiency of chromium presents as hyperglycaemia and has been reported in adults as a rare complication of prolonged parenteral nutrition.
• Copper metabolism is abnormal in Wilson’s disease.
• Deficiency occasionally occurs but only in young children, causing microcytic hypochromic anaemia, neutropenia, retarded growth, skeletal rarefaction and dermatosis.
