1
Paragonimus westermani
Paragonimus westermani (Kebert, 1878) Braun, 1899, the Oriental lung fluke. The
most heavily endemic regions of Oriental paragonimiasis are in central China,
Korea, Japan, Nepal, Thailand, and Philippines.
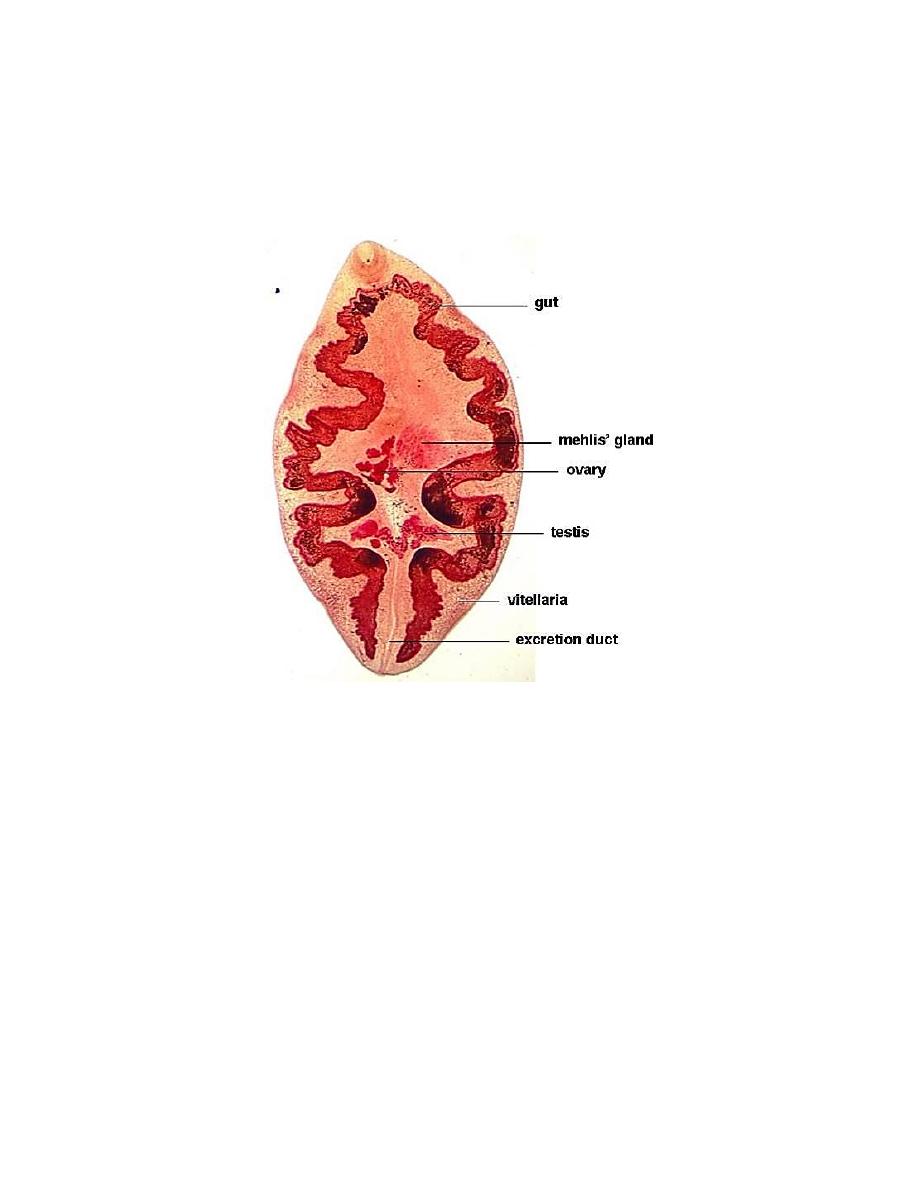
Morphology, Biology and Life Cycle
The adult Oriental lung fluke resides normally in fibrous capsules in the lungs, but
it may also develop in other soft tissues of the body. The worm is a plump, ovoidal
object, reddish-brown in the living state, gray or grayish-brown after preservation.
It measures 7.5 to 12 mm in length, 4 to 6 mm in breadth and 3.5 to 5 mm in
thickness.

2
Eggs of Paragonimus taken from a lung biopsy
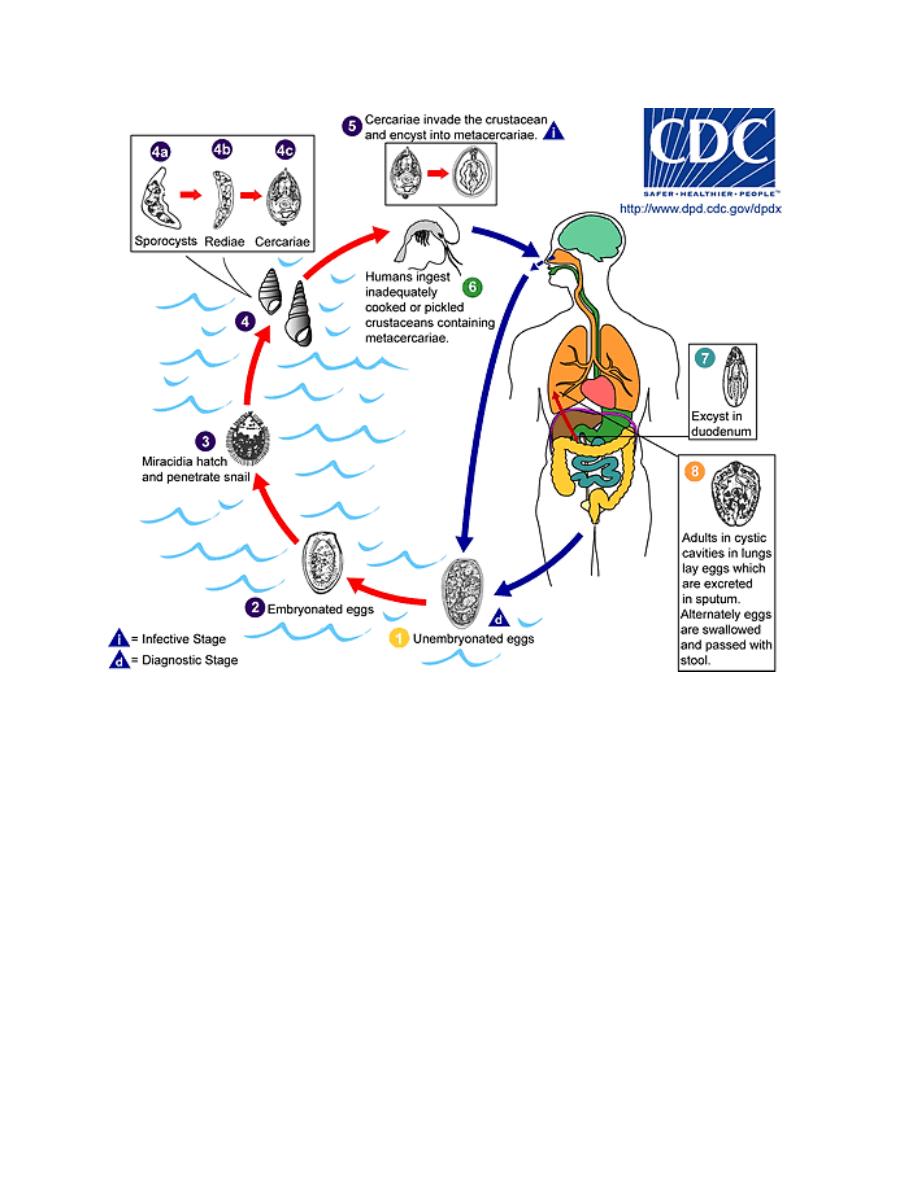
Egg of P.westermani are broadly ovoidal, golden-brown in color, measure 80 to
118 microns by 48 to 60 microns. They are unembryonated when laid by the parent
worm. When deposited in the pulmonary capsules the egg usually accumulates
around the worm, but some eggs reach the respiratory passages and are coughed
up, imparting a rusty tinge to the sputum. Many are swallowed, pass down the
digestive tract and evacuated in the feces. If the eggs reach running water, they
embryonate in 16 or more days, then hatch. The free-swimming miracidia enter
suitable operculate snails, including several species of Semisulcospira. Within
these snails, the miracidium transforms into a first generation sporocyst, in which
rediae are developed. Each redia, in turn, produces a brood of cercariae, which
escape from the snail and are temporarily free in the water. These cercariae invade
the viscera and muscles of freshwater crabs, in the soft tissues of which they
become encysted.
When the viable cysts are ingested by human, excystation occurs in the duodenum
and the young worms migrate through the intestinal wall to the peritoneal cavity,
burrow through the diaphragm, enter the lungs, and finally settle down, usually in
pairs, near a bronchiole where they develop into adult worms within a fibrous
capsule laid down by the host.
3
Pathogenicity and Symptomatology
If the lung fluke reaches the pulmonary parenchyma, the host-tissue reaction
consists of an eosinophilic and neutrophilic infiltration around the growing worm,
followed by the development of a thick fibrous envelope 6 to 10 mm in diameter in
the deeper lung tissue. Almost invariably small blood vessels in the capsule
provide leakage from the cystic cavity into the bronchiole, so that with the
irritation caused by discharge of eggs and the fluke's metabolites into a bronchiole,
paroxysmal coughing occur, frequently resulting in hemorrhage, with blood in
sputum.
Worms have also been discovered in many ectopic locations, including the liver,
intestinal wall, mesenteric lymph nodes, peritoneum, and brain. In these abnormal

4
sites there is a tendency for development of abscesses, or the lesion may be
suppurative or frankly ulcerative.
There may be no symptoms other than the occasional coughing up of rusty sputum,
Shortness of breath but there may be a history of periodic hemoptysis or at least of
occasional discharge of blood-tinged sputum. However, dyspnea, fever, and
anorexia have been observed in cases of extensive pulmonary involvement.
Secondary anemia rarely occurs as a result of the hemoptysis.
Diagnosis
A specific diagnosis can readily be made by the recovery of the eggs of
P.westermani in rusty or blood-tinged sputum, or from the feces, pleural aspirate or
peritoneal abscesses.
Treatment
Triclabendazole,
WHO-recommended
medicines
for
treatment
of
paragonimiasis. 20 mg/kg, in two divided doses of 10 mg/kg, to be administered
on the same day.
Epidemiology
The definitive host commonly acquires the infection from eating the tissues or
freshwater crabs. These crustaceans live typically in clear, fresh water, usually
mountain streams, which are contaminated with the egg-laden excreta of human
and reservoir hosts, which provide the inoculum for the molluskan hosts and
subsequently the crustaceans.
Control
For the individual in endemic areas, the disease may be prevented by care not to
eat crabs or cryfishes unless they have been thoroughly heated, and care not to
contaminate fingers during preparation of the raw crustaceans for the table. No
public health program has been developed to control the infection.