Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
1
Oral Ulceration
(RAS) or Ulceration (RAU)
Recurrent Aphthous Stomatitis
RAS constitutes the most common oral mucosal disease and
affects around 25% of the population at some time in their life.
Many cases are mild, and no treatment is required. Generally,
RAS characterized by recurring ulcers confined to the oral
mucosa in patients with no other signs of any disease.
However, ulcers similar and sometimes identical to RAS can be
a feature of other diseases or syndromes. Whether these are
truly aphthous stomatitis is unclear. Diseases & syndromes
such as Behçet
’s disease, MAGIC syndrome (mouth and genital
ulcers with inflamed cartilage syndrome), PFAPA syndrome
(Periodic Fever, Aphthous Stomatitis, Pharyngitis,
Adenitis “a
childhood syndrome”)), and HIV infection have been associated
with RAS like ulcers. Furthermore, immunologic disorders,
hematologic deficiencies, allergic or psychological abnormalities
have also been implicated in cases of RAS.
linical features:
General c
• Ulcers frequently start in childhood. Recurrences increase in
frequency until early adult life or a bit later, then gradually fade.
• If Ulcers start in adults, this may indicate a hematological
deficiency.
• RAU are rare in the elderly, particularly the edentulous unless
affected by a hematological deficiency.
• Patients of different socioeconomic status are affected, but the
majority of them are non-smokers.
• Many patients have prodromal symptoms of pricking or
sensitivity and erythema at the site for a few- 24 hours before
the ulcer appears.
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
2
• The ulcers have a smooth sharply defined margin with an
erythematous halo in the enlarging phase. Typically, the center
is yellowish-greyish. The surrounding area is usually slightly
inflamed/erythematous.
• The erythematous halo or rim reduces once the ulcer reaches
its full size, and while it heals, the margin becomes irregular or
less well defined.
, each of which is defined by its
of RAS
types
There are three
clinical presentation.
1- Minor aphthous ulcers
2- Major
aphthous ulcers (other clinical variants
Sutton’s
disease, periadenitis mucosa necrotica recurrens)
3- Herpetiform ulcers
Minor aphthous ulcer: Is the most common type of RAS which
usually occurs as one painful ulcer of less than 1 cm in
diameter, less common in a group of 2-3 ulcers.
Minor aphthous ulcer recurs at intervals of a few weeks (during
its peak). Typically affecting only the non-keratinized mucosa,
usually the labial and buccal mucosa, sulcuses, lateral borders
of the tongue, or floor of the mouth.
The individual minor aphthae persist for 7
–10 days, then heal
without scarring. Often all ulcers in a group develop and heal
more or less synchronously. Unpredictable, remissions of
several months may be noted. In rare and severe cases, ulcers
are more numerous, and new groups may develop and heal
continuously at different sites, without remission.
Major aphthous ulcer: Other names
(Sutton’s disease,
periadenitis mucosa necrotica recurrens). Mostly a single
painful ulcer which is larger than 1 cm in diameter, occasionally
2-3 major ulcers may develop at same time. The ulcer usually
develops on the keratinized mucosa (less commonly on the
non-keratinized) affecting the palate, fauces (back of the mouth

Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
3
or oropharynx), buccal mucosa, dorsum and lateral borders of
the tongue.
Major aphthous is very painful and interfere with eating. It
persists for many weeks and heals with scarring. Ulcer can be
designated as major on the basis of either size or duration.
Herpetiform aphthous ulcers also rare and distinct clinical
form of RAU which causes crops of many tiny ulcers (1-2 mm
across), dozens or hundreds may present at a time.
Ulcers may
coalesce to form large irregular ulcers. HAUs occur usually on
non-keratinized mucosa such as the floor of mouth and ventral
surface of the tongue, other parts of the oral mucosa may be
affected. The background mucosa is red, giving a resemblance
to herpetic ulceration, but viral infection is not the cause.
of RAU/RAS:
Etiology
There is no clear explanation for the etiology of RAS; however,
different predisposing factors may apply to different individuals or
subgroups of patients.
Possible etiologic factors:
• Genetic predisposition: Family history is often positive
• Exaggerated response to trauma
• Immunological abnormalities
• Gastrointestinal disorders: Such as Crohn's disease, ulcerative
colitis, and coeliac disease, as well as malabsorption.
• Hematological deficiencies: Deficiencies of vitamin B12, folate or
iron have been reported in approximately 20% of patients with
RAS (especially if it starts in middle age adults and elderly)
• Hormonal disturbances: RAU might occur in females during the
luteal phase of the menstrual cycle. Pregnancy is often associated
with remission
• Stress
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
4
• HIV infection: RAS is a recognized feature of HIV infection. It's
both frequency and severity are related to the degree of immune
deficiency
• Non-smoking: Smokers don not have RAS, this might be due to
the effects of nicotine on the oral mucosa by increasing its
epithelium thickness or keratinization
• Allergy: Though it's less common, allergy to foods such as milk,
cheese, wheat, and flour. As well as, allergy to a detergent present
in toothpaste, sodium lauryl sulfate (SLS), was suspected as a
predisposing etiologic factor in RAS development
:
of RAU/RAS
Diagnosis
.
examination
and
history
detailed
mostly achieved via
s
Diagnosis i
.
of other diseases
exclusion
RAS is essentially diagnosed by
regular
ling intraoral ulcers at
hea
-
of self
rimarily recurrences
P
intervals. Almost the only other condition with this history is
Behçet
’s disease.
Usually, increasing frequency of ulcers brings the patient to seek
treatment. A detailed history of the ulcer number, shape, size, site,
duration, frequency of attacks is required.
should be
s
laboratory investigation
patients appear well,
Though
considered especially when ulcers worsen or begin above the age
particularly important
are
s
ematological investigation
H
of 25 years.
in older patients and those with recent exacerbations in frequency
of crops, ulcer size or pain.
Hence, patients with abnormal hematological values should be
referred to a hematologist/ or physician to rule out GIT Diseases
or malabsorption syndromes and to initiate proper replacement
therapy which control or abolish aphthae.
It is also useful to investigate any food allergy or gluten
sensitivity especially in severe cases resistant to other forms of
treatment.
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
5
Biopsies are only indicated when it is necessary to exclude
other diseases, particularly granulomatous diseases such as
Crohn’s disease or Sarcoidosis. Biopsy might be considered
with Major aphthous to exclude malignancy.
HIV infected patients, particularly those with CD4 counts below
oral
occasionally, such
,
, may develop major aphthous
3
100/mm
ulcers are the presenting sign of AIDS.
:
of RAU/RAS
Treatment
Apart from the minority with underlying systemic disease,
treatment is empirical and palliative only. Despite numerous
clinical trials, no medication gives complete cure or relief. Low-
potency and topical agents should be tried first. Some patients
report that changing toothpastes is helpful.
1. Reassurance and education: Patients need to understand that
the ulcers may not be curable but can be made bearable with
symptomatic treatment. Reducing the number of attacks is more
difficult to address, but some treatments are successful,
particularly if attacks are frequent. The condition usually wanes
eventually by its own, although after many years.
2. Medications prescribed should relate to the severity of the
disease.
* Corticosteroids: Some patients get relief from hydrocortisone
pellets or muco-adhesive buccal tablets (2.5 mg hydrocortisone
sodium succinate) allowed to dissolve next to the ulcer three
times per day. These low-potency corticosteroids adhere to the
mucosa to provide a high local concentration of drug and are
suitable for use in dental practice. They probably reduce the
painful inflammation but do not speed healing much or reduce
frequency of attacks. They are best applied in the very early,
asymptomatic stages.
%
0.1
Kenalog in Orabase
such as
dental paste
Triamcinolone
2-3 times daily.
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
6
Composition: 1mg of triamcinolone (medium potency steroid) in
orabase (Orabase contains gelatin, pectin, &
carboxymethylcellulose sodium in plasticized hydrocarbon gel,
a polyethylene and mineral oil gel base).
ualinium chloride
Composed of Deq
:
(aerosol)
Angiovag spray
(0.1% w/v), Hydrocortisone acetate (0.06 % w/v), Lidocaine
hydrochloride (0.1% w/v), Tyrothricin (0.4% w/v). Initial dose
(first 3 days) 1-2 nebulization (spray) every 3 hours, then
maintenance dose 1-2 nebulization (if required) every 6 hours.
* Local analgesics: These provide only symptomatic relief.
spray helps
romucosal
o
or
outhwash
m
enzydamine 0.15% w/v
B
is a
)
hydrochloride
benzydamine
(
Benzydamine
some patients.
locally acting nonsteroidal anti-inflammatory drug with local
anesthetic and analgesic properties for pain relief and anti-
inflammatory treatment of inflammatory conditions of the mouth
and throat. Topical lidocaine or benzocaine sprays and gels are
more effective but can only be used in limited doses and for a
short time (mostly before meals).
* Chlorhexidine: A 0.2% solution has also been used as a
mouth rinse for aphthae. Used three times daily after meals and
held in the mouth for at least 1 minute, it has been claimed to
reduce the duration and discomfort of aphthous stomatitis.
* Topical salicylate preparations: Salicylates have an anti-
inflammatory action and also have local effects. Preparations of
choline salicylate in a gel can be applied to aphthae. These
preparations, which are available over the counter, appear to
help some patients.
* Tetracycline mouth rinses: Trials in both the UK and USA
showed that tetracycline rinses significantly reduced both the
frequency and severity of aphthae. Best reserved for
herpetiform aphthae. The contents of a tetracycline capsule
(250 mg) can be stirred in a cup of water and held in the mouth
for 2
–3 minutes, three times daily. However, there are few
easily soluble tetracycline preparations, and their use carries a
risk of super-infection by Candida albicans.
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
7
* Hyaluronic acid: Recent studies and clinical trials showed that
0.2% hyaluronic acid gel was effective for the treatment of
recurrent minor aphthous ulcers.
Note: Low level Diode LASER may also be used for the
treatment of some cases of RAUs
Treatment of major aphthae
which
are so painful, persistent and
resistant to conventional treatment. MAUs can be treated by
placing a gauze sponge containing the topical steroid on the
ulcer and leaving it in place for 15 to 30 minutes to allow for
longer contact of the medication. Intralesional injection of
steroids can be used to treat large major RAS lesions.
pentoxifylline,
treatments include
Reportedly effective
, but
and dapsone
azathioprine, cyclosporin, colchicine
effective. However, such
is probably most reliably
thalidomide
drugs can only be given under specialist supervision.
Thalidomide has been shown to reduce both the incidence and
severity of major RAS in both HIV-positive and HIV-negative
patients, but this drug must be used with extreme caution in
women during childbearing years (not used in pregnancy) owing
to the potential for severe life-threatening and deforming birth
defects or congenital defects.
Behçet’s disease/syndrome
Behçet’s disease (BD) was initially described by the Turkish
dermatologist Hulusi Behçet as a triad of symptoms including
recurring oral ulcers, recurring genital ulcers, and eye
involvement.
BD is now known to be a multisystem disorder with many
possible manifestations. There is a systemic vasculitis of small
blood vessels and affects many more organ systems than
suggested by the triad limited definition.
-
The importance Behçet’s diagnosis is indicated by the life
threatening risk of thrombosis, blindness or brain damage.

Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
8
The highest incidence of BD has been reported in Eastern Asia,
the Middle East, and the Eastern Mediterranean, particularly
Turkey and Japan, where BD is a leading cause of blindness in
young males; however, cases have been reported worldwide,
including Europe and North America (especially immigrants).
BD is more severe in younger patients and those with eye and
GIT involvement.
Clinical manifestation:
Patients are usually young adult males between 20 and 40
years old. Patients suffer one of four patterns of disease:
* Mucocutaneous: Oral aphthae are the most consistent feature,
not distinguishable from common aphthous stomatitis and may
be of any of the three RAU types. There is often genital
ulceration, skin rash/inflammation (erythema nodosum) and
vasculitis.
* Arthritic: Joint involvement with or without mucocutaneous
involvement. The large weight-bearing joints are most affected.
There is pain, but no destructive arthritis and only a few joints
are involved. The pain may be relapsing or constant.
* Neurological: This type may occur with or without other
features and is usually a late stage. Vasculitis within the brain
causes a variety of neurological symptoms including sensory
and motor disturbances, confusion and seizures. Thrombosis of
vessels causes raised intracranial pressure, blurred vision and
headache.
* Ocular: This type may also be solitary or accompanies other
types. There may be uveal inflammation or vasculitis and
thrombosis of the retinal arteries, either of which can lead
rapidly to blindness if not treated.
Etiology:
The etiology is unknown, but the disease has features including
circulating immune complexes, high levels of cytokine secretion
and activation of lymphocytes and macrophages in the
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
9
circulation. These suggest an immune-mediated reaction
(disease), and it is presumed that this may be a response to an
unknown infectious agent, possibly through immune cross
reaction between pathogen and host heat shock proteins.
The racial distribution suggests a strong genetic component and
HLA tissue types are linked, most strongly to HLA-B51. This is a
common allele and so is not of use in diagnosis but can predict
ocular lesions.
Diagnosis:
. Behçet’s
first manifestation
are frequently the
Oral aphthae
disease should therefore be considered in the differential
diagnosis of aphthous stomatitis, particularly in patients from a
racial group at risk, and the medical history should be checked
the features of The International Criteria for Behçet’s
for
.
Disease System
The frequency of other manifestations is highly variable.
aphthous stomatitis in combination
in a dental clinic,
,
However
with any two of the other major features can be regarded as
likely indicators for referral of the patient to a specialist.
Hence, BD diagnosis is mostly history & clinical based.
Pathergy test: It is common for patients with BD to have a
cutaneous hyper-reactivity to intra-cutaneous injection or a
needlestick
Apart from pathergy test, other tests are not helpful in diagnosis
of BD. However, laboratory tests may be used to rule out other
diseases, such as connective tissue (e.g., lupus erythematosus)
and hematologic diseases causing severe neutropenia.
Pathergy test is positive if there is an exaggerated response to
a sterile needle puncture of the skin. However, the test must be
interpreted by an experienced clinician and tends to be positive
only in Mediterranean patients. Moreover, a positive pathergy
test does not correlate with the presence of oral lesions or with
the overall severity of the disease and is rarely positive in
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
10
patients who are not originally from the Mediterranean basin. It
is also not entirely specific for BD.
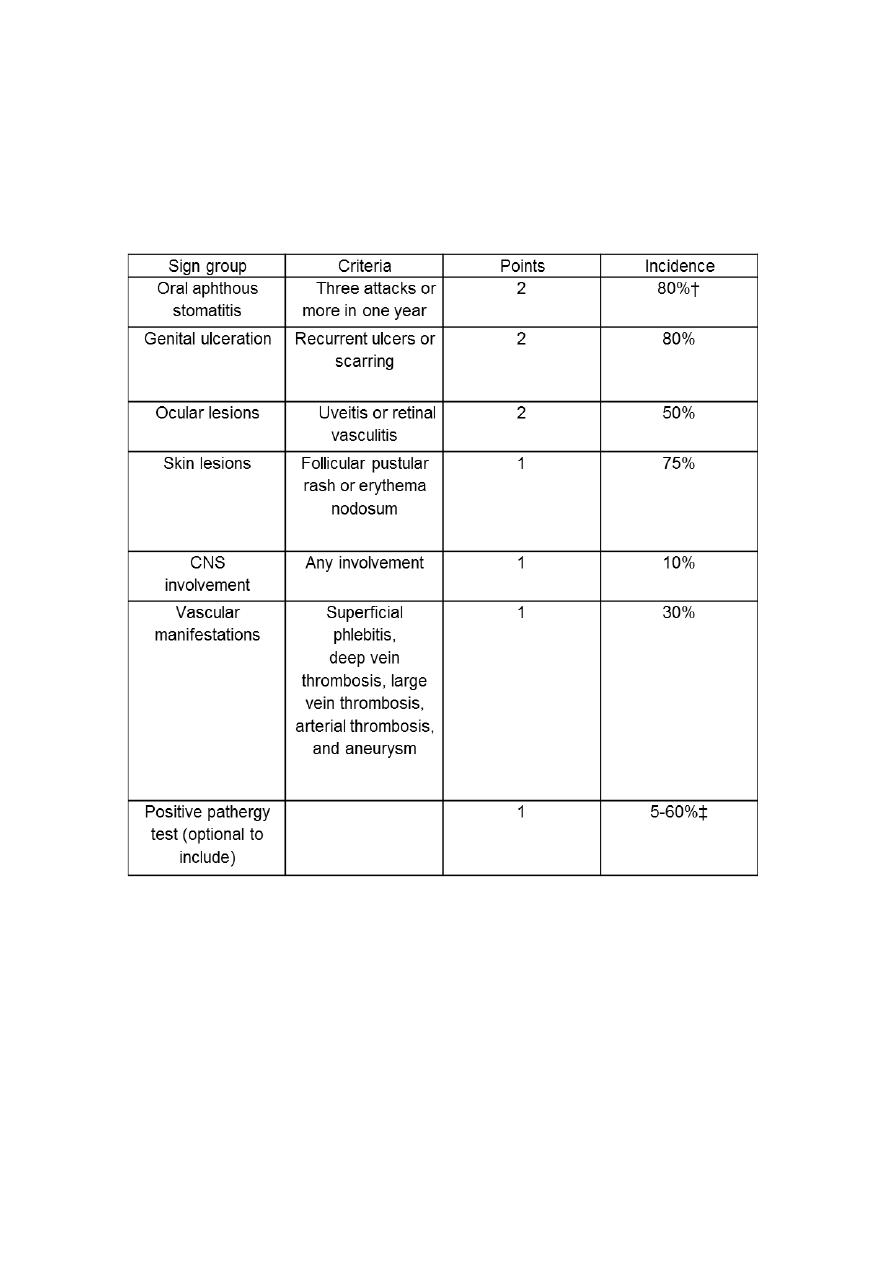
The International Criteria for Behçet’s Disease 2010
together with their overall incidence in all patients*
*A score of 4 or more points predicts Behçet
’s disease with 95%
certainty, 98% if the pathergy test is performed. Incidence of
features varies between populations.
†100% using older criteria, previously a requirement for diagnosis.
‡The higher figure is for patients from the middle East and central
Asia.
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
11
Complications include:
* Blindness
* Rupture of a large-vessel, aneurysms, thrombosis and embolism.
In the absence of these significant complications, relapses become
less frequent, and the disease may eventually fade.
Treatment:
Treatment of BD depends on the severity and the sites of
involvement.
Patients with sight-threatening (eye involvement) or CNS lesions
require more aggressive therapy with drugs that have higher
potential for serious side effects.
immunosuppressive drugs combined with
other
and
Azathioprine
have been shown to reduce ocular disease as well as
prednisone
oral and genital involvement.
-
ich has fewer side effects than immune
, wh
Pentoxifylline
suppressive drugs or systemic steroids, has also been reported to
be effective in decreasing disease activity, particularly of oral and
genital lesions.
have also been used
thalidomide
, and
colchicine
,
Dapsone
effectively to treat mucosal lesions of BD.
Inflammatory bowel disease (IBD)
IBD is a general classification of inflammatory processes that
affect the large and small intestines such as:
Ulcerative colitis
Crohn’s disease
Both diseases are of unknown etiology (Idiopathic). They are of
interest to the dentists because of their associated oral findings
and the impact of their medical management (particularly the use
of corticosteroids) on dental management.

Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
12
Ulcerative colitis:
Diagnosis of ulcerative colitis is made on the basis of:
*History *Clinical examination *Gastrointestinal imaging
*Endoscopy, which involves direct visualization of the intestinal
mucosa.
Most important is the sigmoidoscopic examination, which usually
reveals the characteristic picture of multiple tiny mucosal ulcers
covered by blood and pus.
Crohn’s disease:
Crohn’s disease is an inflammatory disease of the small or large
intestine and the inflammation involves all layers of the gut. Gross
examination may reveal mucosal ulcers or open sores of the
intestines.
Oral lesions:
* Multiple recurrent aphthous ulcers.
* Diffuse swelling of the lips and face.
* Inflammatory hyperplasia of the oral mucosa with a cobblestone
pattern.
* Indurated polypoid tag like lesions in the vestibule and retromolar
pad area.
* Angular cheilitis and glossitis (oral manifestations of anemia)
* Persistent deep linear ulcerations with hyperplastic margins.
* Localized mucocele formation.
* Oral lesions may precede the radiologic changes of the disease
by up to 1 year.
In conclusion: Patients with IBD complain of pain associated with
ulcerative lesions in the oral cavity.
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
13
The
Palliative rinses, ointment, and topical steroids may be helpful.
t of the IBD is carried out by a specialist physician or GIT
treatmen
surgeon.
Note: There appears to be an increased risk of dental caries that is
probably related to dietary changes in patients with IBD. The
causes of the dental caries and increased incidence of bacterial
and fungal infections are multifactorial but appear to be related to
either the patient’s altered immune status (due to therapy) or diet.
:
Cyclic neutropenia
Cyclic neutropenia is a rare hematologic disorder that occurs
secondary to a periodic failure of the stem cells in the bone
marrow to form neutrophils.
It is characterized by transient severe neutropenia that occurs
approximately every 21 days (3-4 weeks). The neutrophil count
lasts 3 to 7 days and is occasionally associated with elevations in
monocytes.
One/third of cases are inherited as an autosomal dominant trait,
and two/thirds arise spontaneously during the first few years of
life.
The disease is frequently present during infancy or childhood,
although there is an adult-onset form of the disease, and both
sexes appear to be equally affected.
The patient looks healthy between neutropenic episodes, but at
regular intervals the absolute neutrophil count falls quickly below
500/µl, and in some patients the neutrophil count falls to 0.
Normal count 1500-8000/µL
Mild neutropenia 1000-1500/µL
Moderate neutropenia 500- 1000/µL
Severe neutropenia < 500/µL
Note: Increased number of neutrophils or Neutrophilia >8000/µL
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
14
Clinical manifestations:
The major signs and symptoms of cyclic neutropenia attributed to
infections occurring during neutropenic episodes.
The most common signs are:
1. Fever
2. Stomatitis (oral ulceration) and periodontal diseases
3. Pharyngitis
4. Skin abscesses
The severity of the infections is related to the severity of the
neutropenia.
However, some patients with severe periodic neutropenia
experience few infections owing to a compensatory increase in
monocytes, which act as phagocytes to prevent the spread of
bacterial infection. Less frequently, patients experience lung and
urinary tract infections and rectal and vaginal ulcers.
Life expectancy is good for patients who receive careful
monitoring.
Oral manifestations:
Oral lesions are common in cyclic neutropenia and might be the
major clinical manifestation of the disease.
The two most common oral manifestations are oral ulcers and
periodontal diseases.
* The oral ulcers recur with each new bout (cycle) of neutropenia
and resemble the large deep scarring ulcers seen in major
aphthous stomatitis.
* The periodontal manifestations range from marginal gingivitis
to rapidly advancing destructive periodontitis.
Diagnosis:
Thorough history and clinical examination of patients with major
RAUs or generalized rapidly advancing progressive periodontitis
cyclic neutropenia
that cannot be explained by local factors alone,
should be ruled out as a possible cause.
Suspicion of cyclic neutropenia should be particularly high when
either of these oral diseases is seen in children. Diagnostic

Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
15
evaluation entails serial measurement of circulating neutrophils.
The diagnosis may be established by demonstrating at least two
cycles of neutropenia.
Treatment:
* Refer to Hematologist for treatment and monitoring of the
disease.
* Dental management: Patients with known cyclic neutropenia
require frequent dental treatment visits to minimize advancing
periodontal disease.
Routine treatment should be confined to the periods when the
absolute neutrophil count is above 2,000/µL.
WBC count should be taken on the day of any dental procedure is
a wise precaution because the neutrophil count can change
rapidly.
Oral hygiene must be carefully maintained, and patients should be
recalled for oral hygiene maintenance every 2 to 3 months.
Treating the disease itself, has reduced oral ulcers and periodontal
disease in these patients.
:
Erythema multiforme
Erythema multiforme (EM) is an acute, inflammatory muco-
cutaneous disease which affects the skin and oral mucosa, other
mucosal surfaces, such as the genitalia, may also be involved.
In patients presenting to dentists, oral lesions may be the only
sign.
EM is one of the few causes of recurrent oral ulceration and also
produces blisters.
It represents a hypersensitivity reaction to infectious agents
(majority of cases) or medications.
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
16
In general, EM is classified into:
if there is less than 10% of skin involvement and there is
EM minor
minimal to no mucous membrane involvement
has more extensive but still characteristic skin
EM major
involvement, with the oral mucosa and other mucous membranes
affected
However, there is a subset of EM that affects the oral mucosa only
without skin involvement
Johnson syndrome (SJS)
–
Stevens
Other forms of EM known as
Lyell
,
Toxic epidermal necrolysis (TEN) (Lyell disease
and
However, recent studies consider
).
syndrome, Lyell's syndrome
them both as different entities.
Etiology:
appears
erythema multiforme
Though the mechanism is unclear,
mediated hypersensitivity reaction.
-
to be a cell
EM is a hypersensitivity reaction, and the most common inciting
however,
(
HSV
Herpes Virus
factors are infections particularly with
infections with mycoplasma and Chlamydia pneumonia have been
to Penicillin, NSAIDS, anticonvulsants, or
Drug reactions
reported).
other drugs play a smaller role. Cases of oral EM precipitated by
benzoic acid, a food preservative, have been reported.
EM is associated with HSV infection in
Studies show that recurrent
, both by history of HSV infection one to three
70% of cases
–
65%
weeks before onset of EM, and sero-positivity for HSV antibodies
or identification of HSV antigens.
Clinical manifestations:
Most patients are aged between 20 and 40 years, with a slight
male predominance.
only skin is involved and this is a relatively mild
,
minor form
In the
self-limiting condition.
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
17
there are florid lesions on skin and oral, nasal
major form
In the
and genital mucosae.
There is acute onset, sometimes preceded by vague arthralgia or
slight fever for a day in the major form.
Then the characteristic ‘target’ “Iris” “Bulls’ Eye” lesions appear,
initially on arms and legs and spreading centrally.
Each lesion is a well-defined red macule about a cm or more in
diameter.
During a period of a few hours to days, the center becomes raised,
with a bluish cyanotic center.
In severe cases, skin lesions blister and ulcerate centrally.
New crops of lesions develop during a period of approximately 10
days.
Oral and lip lesions appear a few days into the attack, most
commonly anteriorly in the mouth on the buccal and labial mucosa
and tongue. Target lesions are not seen intra-orally
The oral lesions are inflamed patches with irregular blistering and
broad, shallow irregular ulcers.
On the lips, fibrin oozes continually and forms hemorrhagic crusts.
There is severe pain.
Diagnosis:
Diagnosis relies on the typical presentation, history of previous
recurrent episodes and a trigger, if present. When only the mouth
is involved, a biopsy may be required; however, as the
appearances are very variable excluding alternative causes might
aid in the diagnosis.

Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
18
Treatment:
The attack usually lasts for 3 or 4 weeks and is self-limiting without
treatment in the minor form. However, oral lesions are painful,
interfere with eating and fluid intake must be maintained. Mild oral
EM can be managed with systemic or topical analgesics for pain
and supportive care since the disease is self-limiting and resolves
within a few weeks.
Unless already resolving, lesions might benefit from treatment with
corticosteroids. A short reducing dose of prednisolone starting at
around 60 mg/day for 3 days, then tapering off over a week, is
frequently given.
Chlorhexidine will prevent secondary oral mucosal infection and
maintain gingival health while tooth brushing is impossible.
If present, Eye lesions require specialist treatment.
More severe cases are usually managed with systemic
corticosteroids. Topical steroids also help to resolve oral and
cutaneous lesions.
Recurrences, usually at intervals of several months, for a year or
two are characteristic and are sometimes increasingly severe.
Hence, attempts should be made to identify the trigger.
Recurrent HSV infections trigger most of cases, therefore,
suspected HSV-associated EM should be treated with antiviral
medications. Treatment with acyclovir at the first sign of the
disease in recurrent EM, suppresses the trigger and controls EM in
approximately half of patients.
Other treatment modalities include dapsone, hydroxychloroquin,
mycophenolate mofetil, azathioprine, colchicine, methotrexate, and
intravenous immunoglobulin.
In patients who have persistent oral lesions, mycoplasmal infection
should be suspected and suppressed.

Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
19
Johnson Syndrome & Toxic Epidermal Necrolysis
-
Stevens
Severe hypersensitivity reaction which has many features in
common with EM but is now considered a separate entity on the
basis of its severity, extent and causes.
Toxic epidermal necrolysis is its most severe presentation.
The mouth is always involved in SJS & TEN.
SJS & TEN are more severe than EM and tend to arise on the
chest rather than the extremities as erythematous and purpuric
macules, lesions known as “atypical targets”.
and sometimes
*
mainly a drug
trigger is
, SJS/TEN
Unlike EM
. Many drugs are implicated, but the most
mycoplasmal infection
other
,
penicillin
&
*
sulfonamides
frequent causes are antibacterial
. Same
NSAIDs in children
drugs such as anticonvulsants, and
drugs in addition to allopurinol, and oxicams (NSAIDs cox-2
inhibitors) in adults.
Some genetic predispositions are known for individual drugs (as in
Han Chinese).
Histopathology indicates that primary cytokine involved in these
hypersensitivity reactions is tumor necrosis factor (TNF)-
α.
The mucosal surfaces of the eye, genitalia, and mouth are almost
always severely affected by SJS/TEN, always with skin
involvement.
The typical oral manifestation is extensive oral ulceration with
hemorrhagic crusts on the lips vermilion, oral and other mucosal
surfaces.
Treatment:
* First of all, cessation of causative drugs.
* Because of the severity of this condition, treatment is generally
with intensive supportive care because of loss of skin barrier (and
antibiotics to control skin infection), intravenous
alternative
immunoglobulin, immunosuppressants (systemic steroids,
Dr. Ahmed Salih Khudhur
BDS, M.Sc., PhD.
Newcastle University/ UK
20
cyclosporine, cyclophosphamide, and TNF-
α inhibitor) and
plasmapheresis.
There is a high risk of death when the area of skin involved in toxic
epidermal necrolysis is extensive.
Other miscellaneous oral ulcers
Other types of ulcers might present in the oral cavity associated
with/or as the main manifestation of local (oral) or systemic
diseases
Such as:
Pemphigus & Mucous Membrane Pemphigoid
Oral cancer
Ulcers associated with: Oral mucositis, Xerostomia &
Sjögren’s
syndrome, Diabetes Mellitus, Renal failure and Others
The basic principles for the management of oral ulcers in
general:
1.
Early diagnosis (might be life-saving)
2.
Relief pain
3.
Remove the cause if possible
/ Treat the
underlaying cause: Direct cause (sharp edge of
broken tooth or restoration, trauma from dental
appliance), infection (viral, bacterial, fungal), and
underlying cause (anemia, malnutrition, immune
disturbance, systemic disease)
4.
Isolate the ulcer from any unwanted effect (such as
further trauma), and prevent super-infection.
5.
Reduce inflammation and promote healing.
6.
Cure if possible.