


Lect. Wasan Mowafaq Al-Omary
Ulcerated vesicular & bullous diseases
Vesicular & bullous lesions which affect the mouth tend to break down rapidly & present
clinically as areas of ulcerations or erosions owing to the effect of saliva & oral
musculature .
Classifications:
Infective
-
1
Herpes simplex virus
Primary herpes or acute herpetic gingivotomatitis
Recurrent herpes or secondary herpetic gingivostomatitis or cold sore
or recurrent herpes labialis
Varicella-Zoster Virus Infection
chickenpox (varicella)
shingles (herpes zoster [HZ]).
Coxsackie virus Infections
Herpangina
hand ,foot- and-mouth disease
Acute lymhpo nodular pharyngitis
immune
-
Auto
-
2
Pemphigus
Pemphigoid
Miscellaneous
-
3
Bullous lichen planus
Epidermolysis bullosa
Herpes virus Infections
:
The Herpes viridae family of viruses contains nine different viruses that are
pathogenic in humans . Nonetheless, each of the herpes viruses is Distinct.HSV-1, an
a-herpes virus, is a ubiquitous virus, .
I n general, infections above the waist are
caused by HSV-1 and those below the waist by HSV-2, although with changing
sexual practices, it is not uncommon to culture HSV-2 from oral lesions and vice
versa.
The primary infection, which occurs on initial contact with the virus, is
acquired by inoculation of the mucosa, skin, and eye with infected secretions.
The virus then travels along the sensory nerve axons and establishes chronic, latent
infection in the sensory ganglion
(such as the trigeminal ganglion).
Extra neuronal
latency ( HSV remaining latent in cells other than neurons such as the epithelium)
may play a role in recurrent lesions of the lips.
Recurrent HSV results when HSV-1
reactivates at latent sites and travels centripetally to the mucosa or the skin, where
it is directly cytopathic to epithelial cells, causing recurrent HSV infection in the form
of localized vesicles or ulcers. The most common sites of infection are the oral and
genital mucosa and the eye. HSV infection of the cornea (keratitis) is a major cause of
blindness in the world. HSV-1 or -2 may cause herpes whitlow, an infection of the
fingers when virus is inoculated into the fingers through a break in the skin. This was
a common occupational hazard (including within the dental profession)
Other HSV-1 infections include herpes gladiatorum (infections of the skin spread
through the sport of wrestling) herpes encephalitis, HSV esophagitis, and HSV
pneumonia. HSV is an important etiologic agent in erythema multiform , HS V has
been recovered in the endoneurial fluid of 77% of patients with Bell's palsy.
Treatment with antiviral therapy resulted in better outcomes, further supporting the
concept of HSV involvement in the pathogenesis of Bell's palsy.
Immunocompromised Hosts
Recurrent
Infection
Primary Infection
Type of Virus
Unusual ulcers at any
mucocutaneous site usually
large and persistent
Herpes labialis
ntraoral ulcers,
Keratoconjunct
ivitis Genital
and skin lesion
,
Gingivo stomatitis,
Kerat conjunctivitis,
Genital and skin
lesion
Herpes
simplex virus
1
Unusual ulcers at any
mucocutaneous site usually
large and persistent;
disseminated infection
,
Genital and
skin lesions
Gingivostomati
tis, Aseptic
meningitis
Genital and skin
lesions,
Gingivostomatitis
Keratoconjunctivitis,
Neonatal infections
Aseptic meningitis
Herpes
simplex virus
2
Disseminated infection
Zoster (shingles
Varicella
(chickenpox
Varicella-
zoster virus
Retinitis, gastroenteritis
hepatitis, severe oral ulcers
Infectious
mononucleosis,
Hepatitis,
Congenital disease
Cytomegalovi
rus
Hairy leukoplakia; lympho
proliferative disorders
Infectious
mononucleosis,
Hepatitis
Encephalitis
Epstein-Barr
virus
Fever; bone marrow
suppression
Roseola infantum,
Otitis media,
Encephalitis
Human
herpesvirus 6
Roseola infantum
Human
herpesvirus 7
Kaposi’s sarcoma; lympho
proliferative disorders; bone
marrow suppression
Infectious
mononucleosis,
Febrile exanthema
Human
herpesvirus 8
Mucocutaneous
lesions, Encephalitis
Simian
herpesvirus B
zoster
-
HSV1, HSV2, and varicella
Are viruses that are known to cause oral mucosal disease .Classically, HSV1 causes a
majority of cases of oral ,pharyngeal infection , meningo encephalitis, &dermatitis
above the waist; HSV2 is implicated in most genital infections. Both types can cause
of either the oral or the genital area, and both may
Primary Or Recurrent Infection
cause recurrent disease at either site. Primary infection may also occur concurrently
in both oral and genital sites from either HSV1 or HSV2, although HSV1 recurs
more frequently in the oral region and HSV2 more frequently in the genital region.
Humans are the only natural reservoir of HSV infection, and spread occurs by direct
intimate contact with lesions or secretions from an asymptomatic carrier. This latter
method of spread of HSV is common; between [2 - 9%] of asymptomatic individuals
shed HSV in saliva or genital secretions.
Latency,
A characteristic of all herpes viruses, occurs when the virus is transported from
mucosal or cutaneous nerve endings by neurons to ganglia where the HSV viral
genome remains present in a non-replicating state. Reactivation of the latent virus
occurs when HSV switches to a replicative state; this can occur as a result of a
number of factors including peripheral tissue injury from trauma or sunburn, fever,
or immunosuppression & menstruation .
Carcinogenesis
There is evidence linking HSV to carcinogenesis. Epidemiologic studies have
demonstrated an increased incidence of HSV2 serum antibodies or positive HSV2
cultures in patients with cervical carcinoma .
Primary herpetic stomatitis
This is a common viral infection caused by HSV1. It affects the mouth, pharynx &
skin . It is most often seen in children, although young adults are sometimes affected
but rarely occur before 6 month due to maternal antibodies .
Clinical manifestations:
Primary herpes manifests as an acute illness with fever, irritability, headache &
lymphadenopathy . Typically, there are initial symptoms of malaise associated with
aches & a sore throat followed after (2-3) days by multiple small oral vesicles which
rapidly breakdown to form well defined yellow base ulcer with a red margin . They
may affect hard palate, tongue, lips & circumoral skin. In addition to the ulcerations,
the whole mucosa is bright-red & painful with a marked edematous gingivitis . The
lesions are self-limiting & usually disappear in ( 7-10) days .
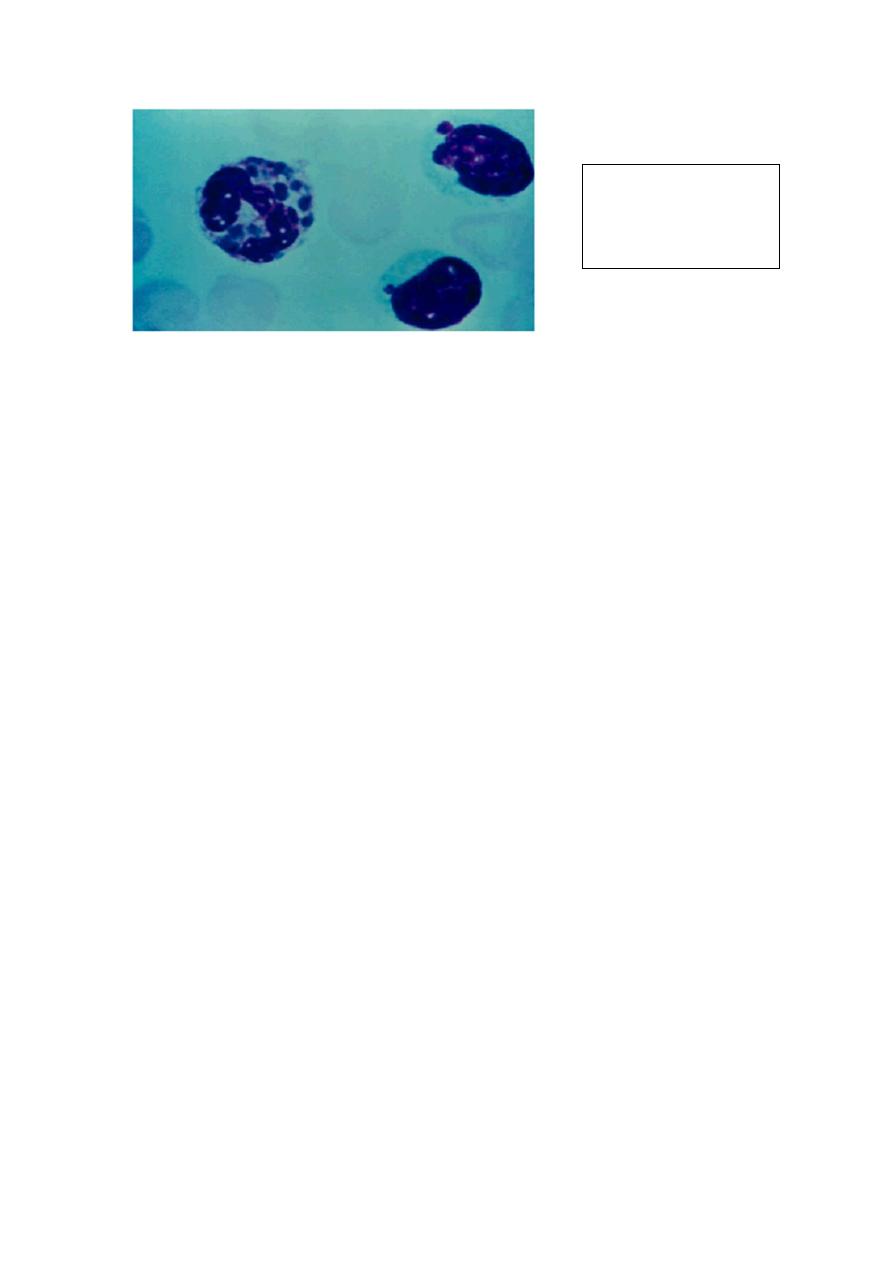
Diagnosis of herpes :
Cytology
:
For cytology, a fresh vesicle can be opened and a scraping made from the base of
the lesion and placed on a microscope slide. The slide may be stained with [Giemsa ,
Wright’s or Papanicolaou’s stain ]and searched for multinu-cleated giant
cells&ballooning degeneration of the nucleus
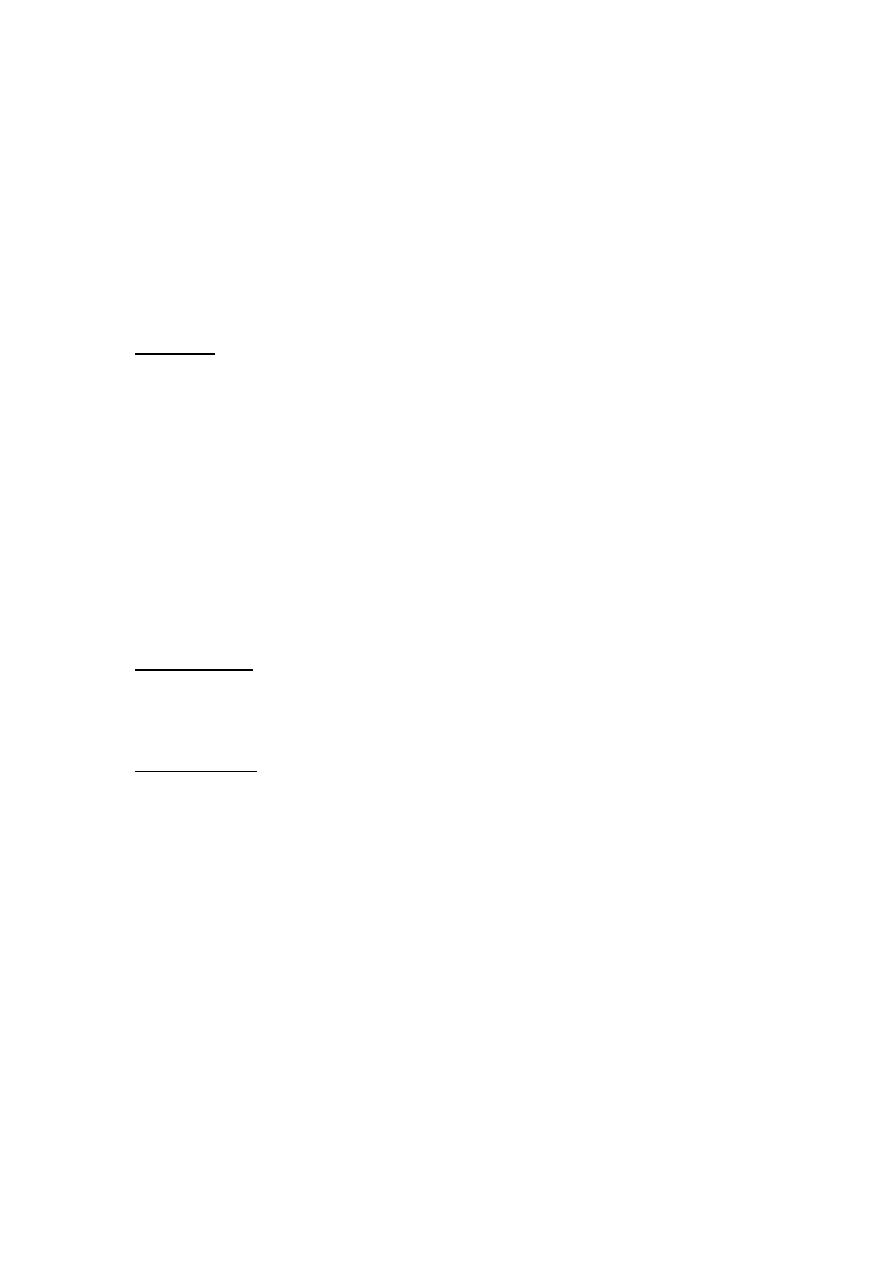
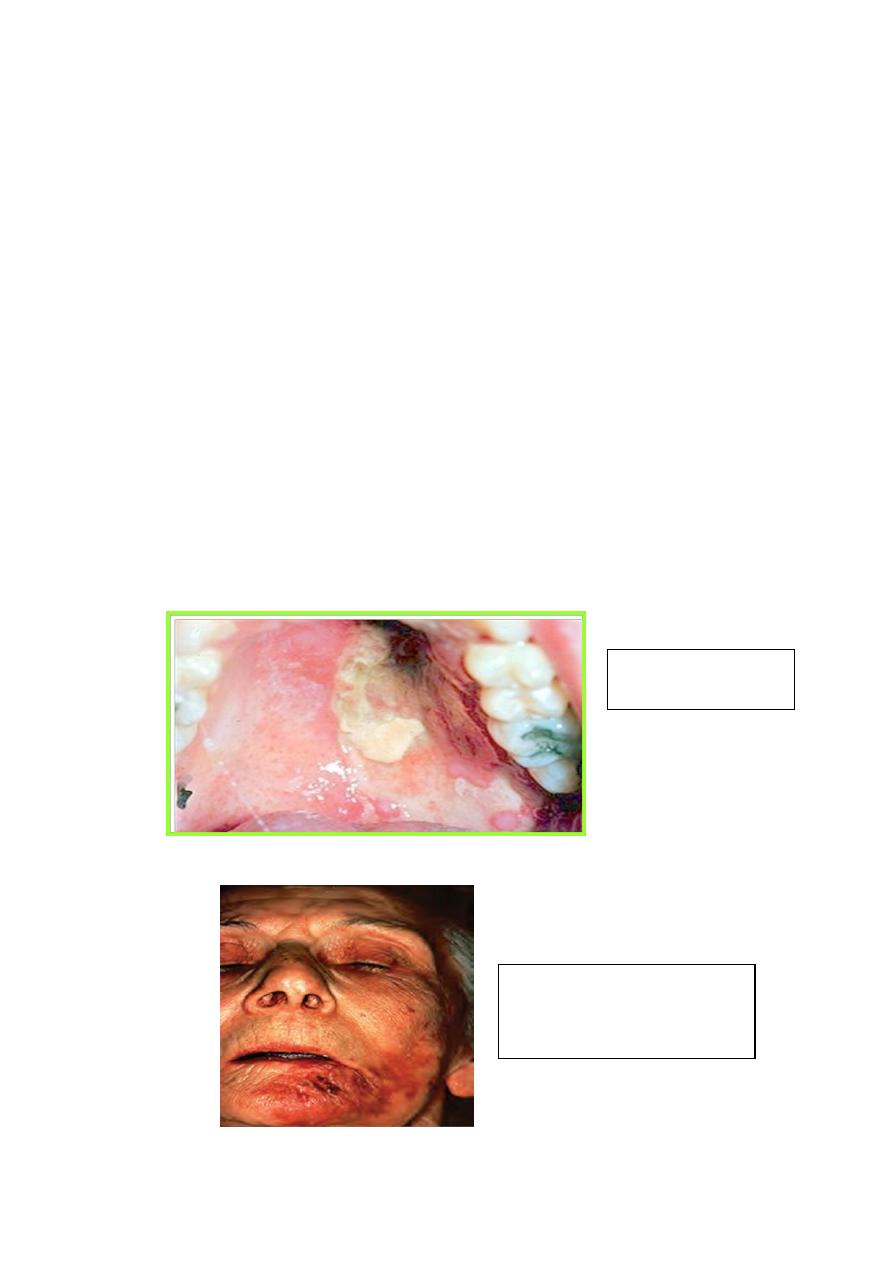
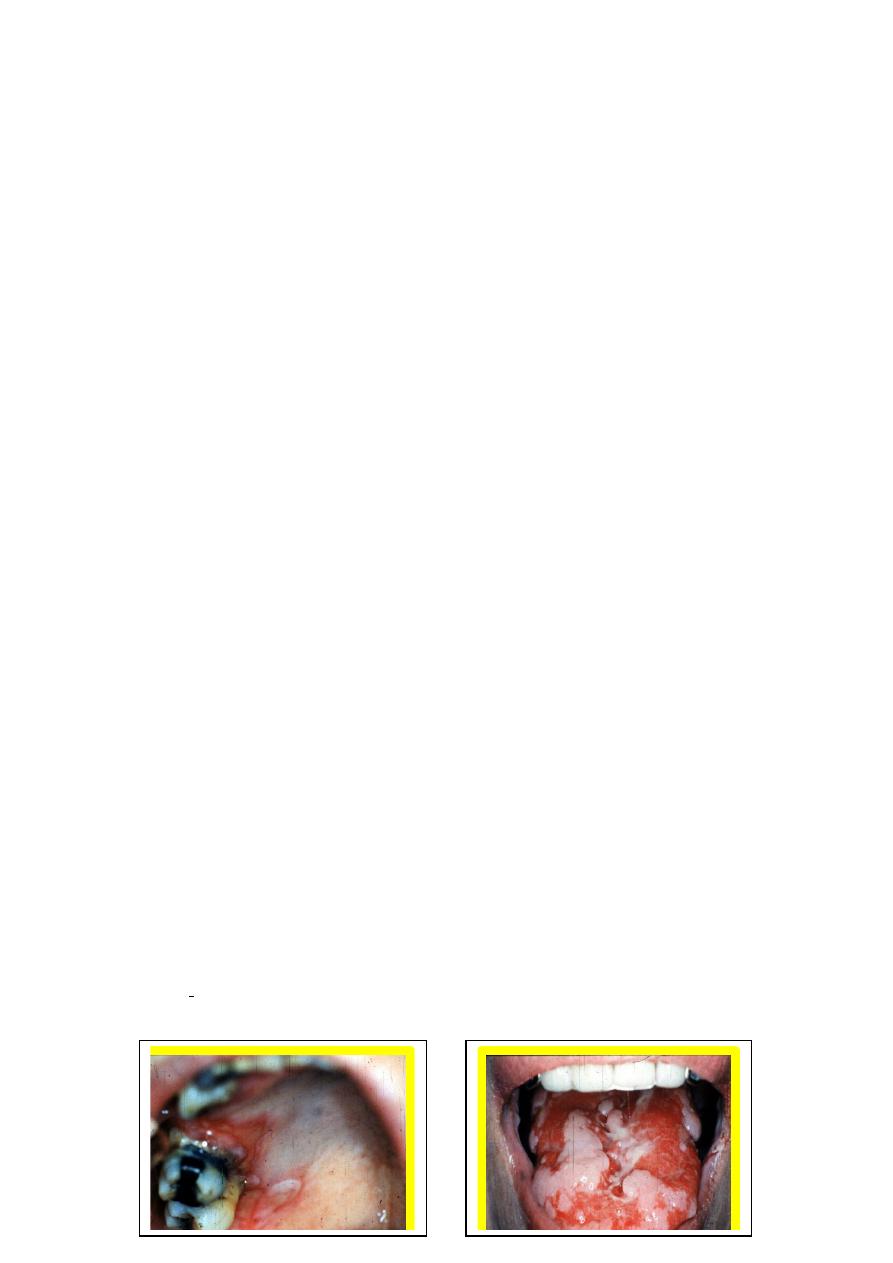
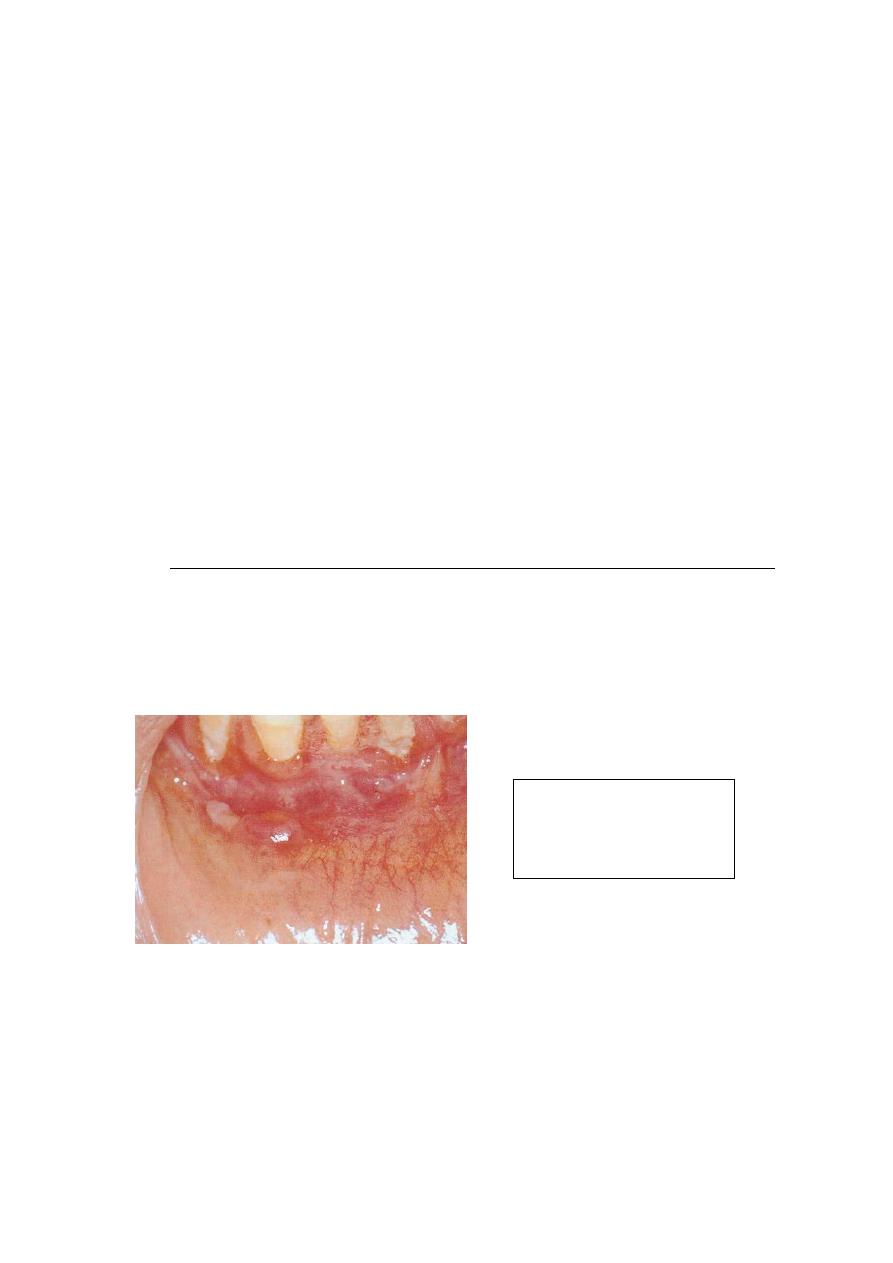
Primary herpetic gingivostomatitis:
erythema and multiple ulcers on the
Multifactorial ulceration
present on movable & bound
mucosa . Note the intensely
erythematous gingiva without
significant plaque
Palatal mucosa
demonstrating numerous
small ulceration that tend to
cluster . Not the significant
erythema & ulceration of the
palatal gingiva
HSV Isolation
:
Isolation and neutralization of a virus in tissue culture is the most positive method of
identification and has a specificity and sensitivity of 100%. A clinician must
remember that isolation of HSV from oral lesions does not necessarily mean that
HSV caused the lesions. Patients who have lesions from other causes may also be
asymptomatic shedders of HSV.
Antibody Titers
Serum specimen should be obtained within 3or 4 days of the onset of symptoms. The
absence of detectable antibodies plus the isolation of HSV from lesions is compatible
with the presence of a primary HSV infection. Antibody to HSV will begin to appear
in a week and reach a peak in 3weeks. A convalescent serum can confirm the
diagnosis of primary HSV infection by demonstrating at least a fourfold risein anti-
HSV antibody. If anti-HSV antibody titers are similar in both the acute and
convalescent sera, then the lesions from which HSV was isolated were recurrent
lesions.
Recurrent herpes
It manifests as attenuated version of primary infection with no systemic symptoms. It
is thought that there is a latent virus situated in the trigeminal ganglion which is
reactivated by inciting factors such as :
-
Sun exposure
Menstruation
Febrile conditions
Cytology smear stained
with Giemsa,
demonstrating
multinucleated giant cells
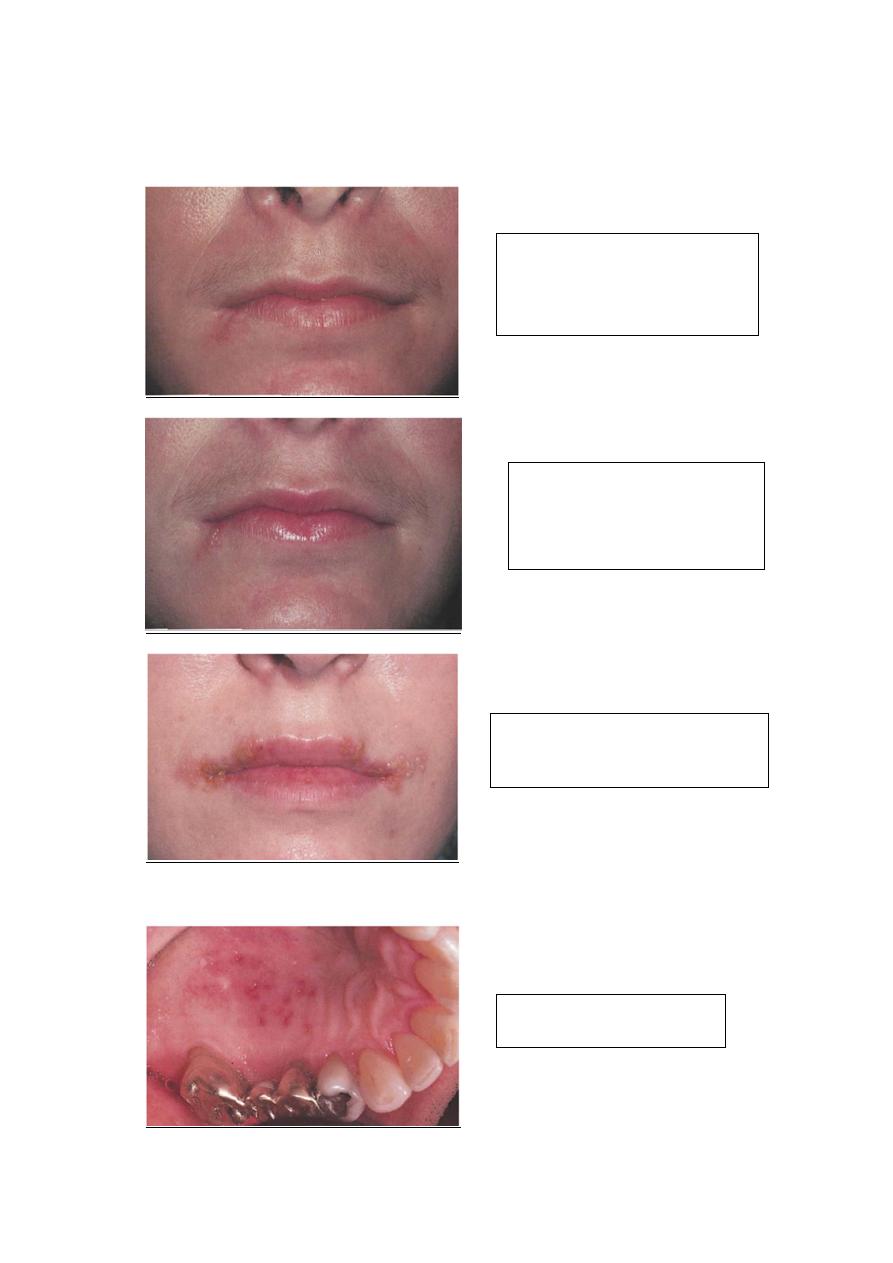
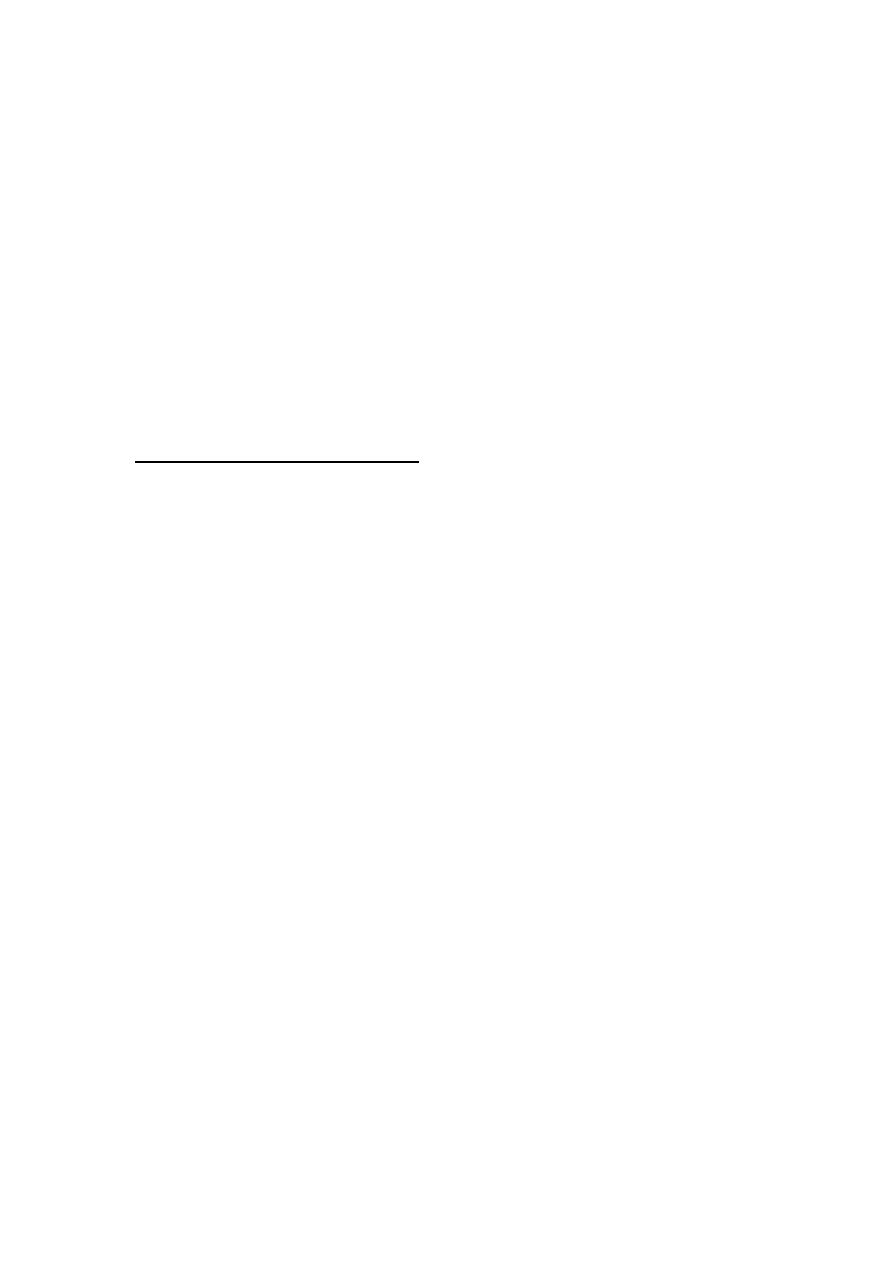
Clinical feature :
Early lesion characterized by Area
of erythema of the right side of the
lower lip that has been present for
less than one day . The patient
reports a burning sensation
Followed by Multiple fluid-filled
vesicles and erythema of the right
side of the lower lip . This picture
depicts the same patient 24 hours
after
Wide spread bilateral fluid-filled
vesicles of both upper & lower lips .
Many of the vesicles have ruptured &
formed crusts
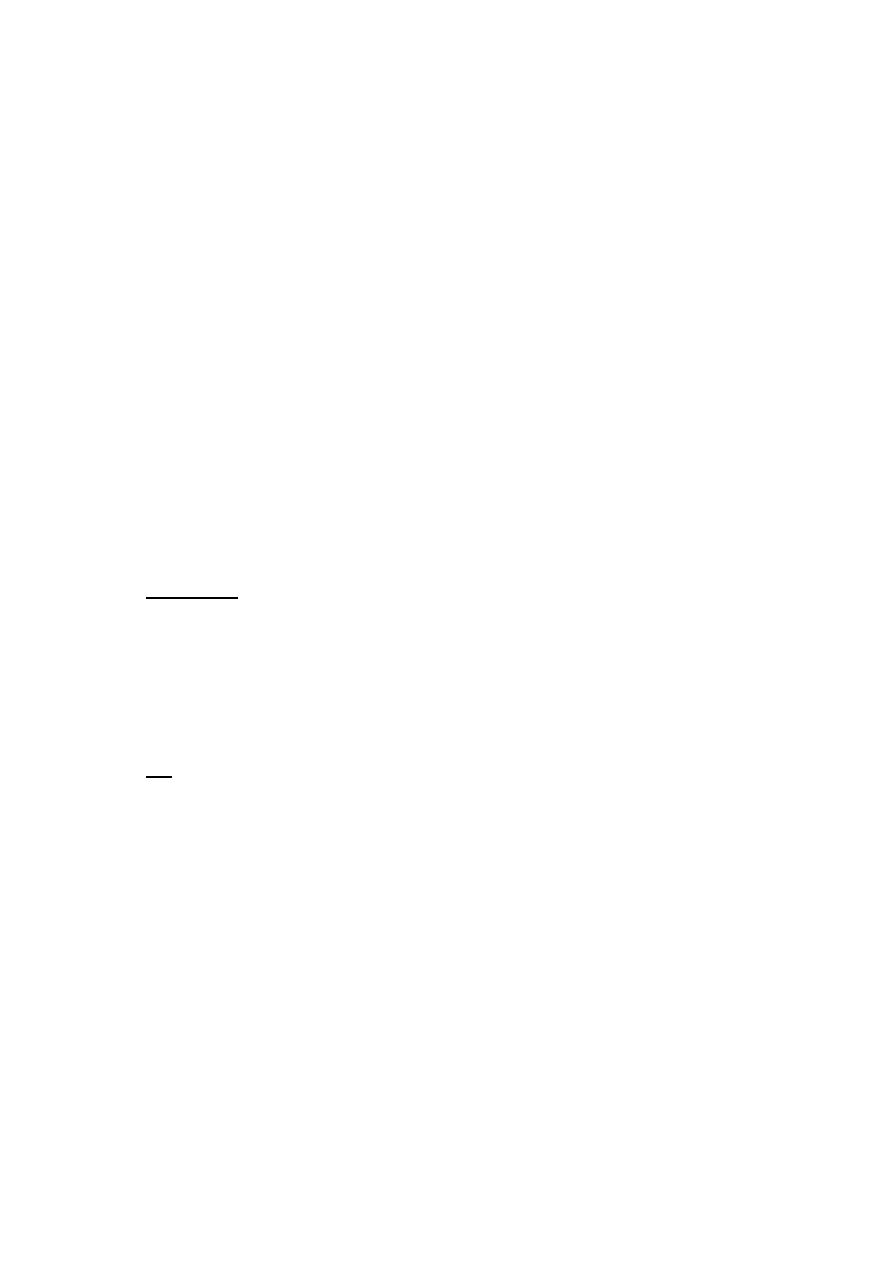
A cluster of multiple small
ulceration of the hard palate
Treatment
:
A significant advance in the management of herpes simplex infections was
the discovery of
acyclovir,
which has no effect on normal cells but inhibits
DNA replication in HSV-infected cells. Acyclovir has been shown to be
effective in the treatment of primary oral HSV in children when therapy was
started in the first 72 hours. Acyclovir significantly decreased days of fever,
pain, lesions, and viral shedding .
Newer antiherpes drugs are now available, including
valacyclovir
and
famciclovir.
The advantage of the newer drugs is increased
bioavailability, allowing for effective treatment with fewer doses.
Milder cases can be managed with supportive care only.
Routine supportive measures include
aspirin or acetaminophen for fever
fluids to maintain proper hydration and electrolyte balance.
If the patient has difficulty eating and drinking, a topical anesthetic may be
administered prior to meals.
Dyclonine hydrochloride 0.5% has been shown to be an excellent topical
anesthetic for the oral mucosa.
If this medication is not available, a solution of diphenhydramine
hydrochloride 5 mg/mL mixed with an equal amount of milk of magnesia
also has satisfactory topical anesthetic properties.
Infants who are not drinking because of severe oral pain should be referred to
a pediatrician for maintenance of proper fluid and electrolyte balance.
Antibiotics are of no help in the treatment of primary herpes infection, and use of
corticosteroids is contraindicated.
Future therapy may include prevention of the infection with use of a genetically
disabled HSV vaccine.
Oral lesion should be treated with topical acyclovir cream 5% five times daily.
Varicella-Zoster Virus Infection
VZV is a herpes virus, and, like other herpes viruses, it causes both primary
and recurrent infection and remains latent in neurons present in sensory ganglia.
VZV is responsible for two major clinical infections of humans
chickenpox (varicella)
shingles (herpes zoster [HZ]).
Chickenpox is a generalized primary infection that occurs the first time an
individual contacts the virus. After the primary disease is healed ,VZV becomes
latent in the dorsal root ganglia of spinal nerves or extra medullary ganglia of
cranial nerves. A child without prior contact with VZV can develop chickenpox
after contact with an individual with HZ.
Clinical Manifestations
:
Chickenpox
Is a childhood disease characterized by mild systemic symptoms and a generalized
intensely pruritic eruption of maculopapular lesions that rapidly develop into vesicles
on an erythematous base. Oral vesicles that rapidly change to ulcers may be seen, but
the oral lesions are
not
an important symptomatic, diagnostic, or
management problem.
HZ
Commonly has a prodromal period of 2 to 4 days ,when shooting pain, paresthesia ,
burning, and tenderness appear along the course of the affected nerve .Unilateral
vesicles on an erythematous base then appear in clusters, chiefly along the course of
the nerve, giving the characteristic clinical picture of single dermatome involvement.
Some lesions spread by viremia occur outside the dermatome. The vesicles turn to
scabs in 1 week, and healing takes place in 2 to 3 weeks. The nerves most commonly
affected with HZ are C3, T5, L1, L2, and the first division of the trigeminal nerve
Diagnosis of HZ:
Clinical feature ; lesion along the distribution of the involved nerve.
Fluorescent antibody test .
PCR
The most common complication of HZ
Postherpetic neuralgia ;which is defined as pain remaining for over a month
after the mucocutaneous lesions have healed, although some clinicians do not
use the term postherpetic neuralgia unless the pain has lasted for at least 3
months after the healing of the lesions. The overall incidence of postherpetic
neuralgia is [12- 14%], but the risk increases significantly after the age of 60
years, most likely due to the decline in cell-mediated immunity.
HZ of the geniculate ganglion called Ramsay Hunt syndrome, It is a rare
form of the disease characterized by
Bell’s palsy .
unilateral vesicles of the external ear.
vesicles of the oral mucosa .
Herps zoster ophthalmicus ; It is serious complication of the HZ because it may
lead to blindness &use of I.V acyclovir to prevent such complication
Treatment of HZ:
Antiviral drugs such as acyclovir 800mg 5 times daily & symptomatic
treatment.
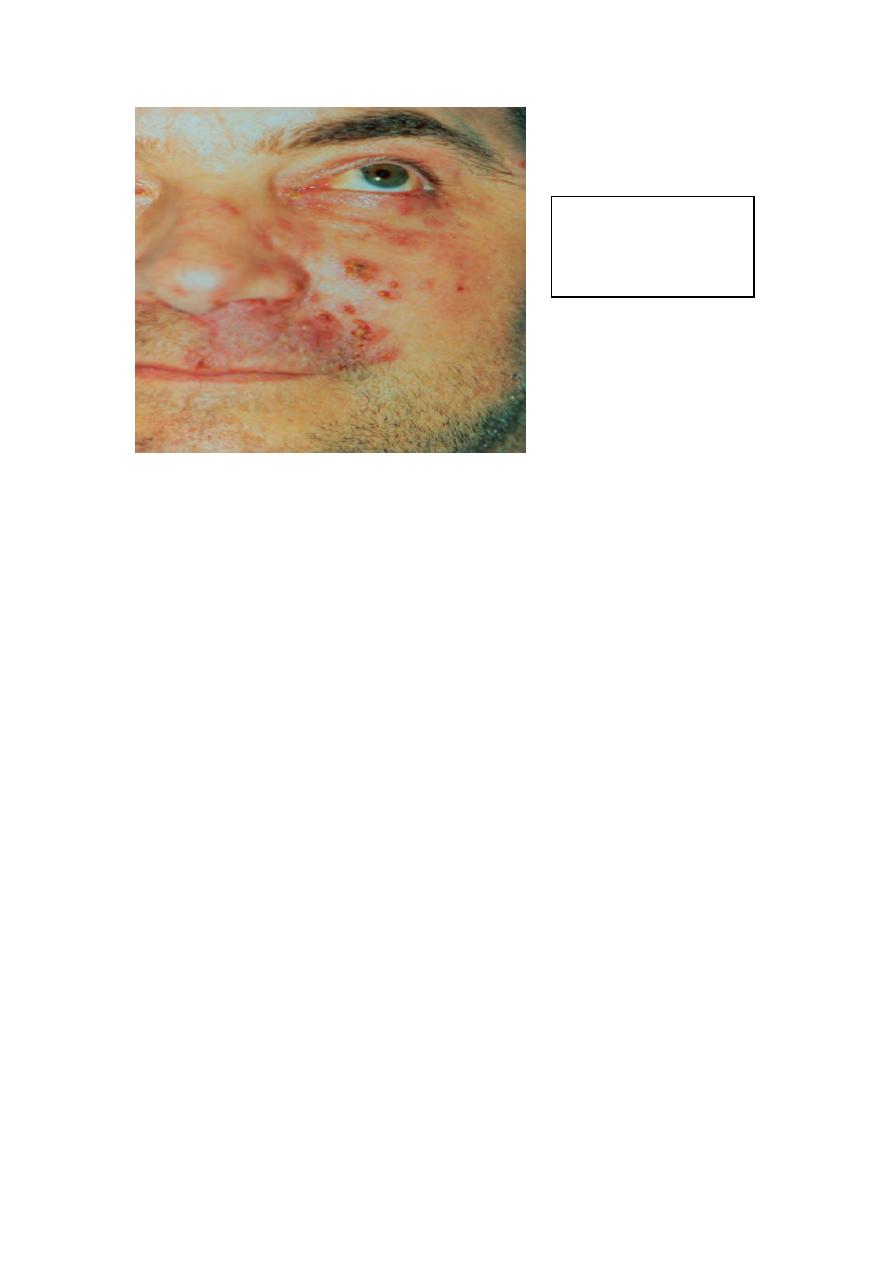
Intra Oral Ulceration
Unilateral
Facial lesions of herpes zoster
involving the third division of the
trigeminal nerve
Coxsackievirus Infections
Coxsackie viruses are (RNA) entero viruses . Coxsackie viruses have been separated
into two groups A and B. There are 24 known types of coxsackie virus group A and
6types of coxsackie virus group B. These viruses cause hepatitis, meningitis,
myocarditis, pericarditis, and acute respiratory disease.
Three clinical types of infection of the oral region that have been described are
usually caused by group A coxsackie viruses:
herpangina
hand ,foot, and-mouth disease
acute lympho nodular pharyngitis.
Herpangina
Coxsackie virus A4 has been shown to cause a majority of cases of herpangina
.Unlike herpes simplex infections, which occur at a constant rate, herpangina
frequently occurs in epidemics that have their highest incidence from June to
October. The majority of cases affect young children ages 3 through, but infection of
adolescents and adults is not uncommon.
Facial lesions of herpes
zoster involving the second
division of the trigeminal
nerve
Clinical Manifestations:
After a 2- to 10-day incubation period, the infection begins with generalized
symptoms of fever, chills, and anorexia. The patient complains of sore throat,
dysphagia, and occasionally sore mouth. Lesions start as macules, which quickly
evolve into papules and vesicles involving the posterior pharynx, tonsils, faucial
pillars, and soft palate. Within 24 to 48 hours, the vesicles rupture, forming small 1 to
2 mm ulcers.
Diagnosis :
Clinical diagnosis , lesion are summed in posterior part of the oral mucosa .
The
disease is usually mild and heals without treatment in 1 week. It is self-limiting & only
supportive care is indicated .
Acute Lymphonodular Pharyngitis
This is a variant of herpangina caused by coxsackie virus A10. The distribution of the
lesions is the same as in herpangina, but yellow-white nodules appear that do not
progress to vesicles or ulcers. The disease is self-limiting, and only supportive care is
indicated. Symptomatic treatment directed toward antipyretic & topical anesthetic ,
also patient should be given proper hydration .
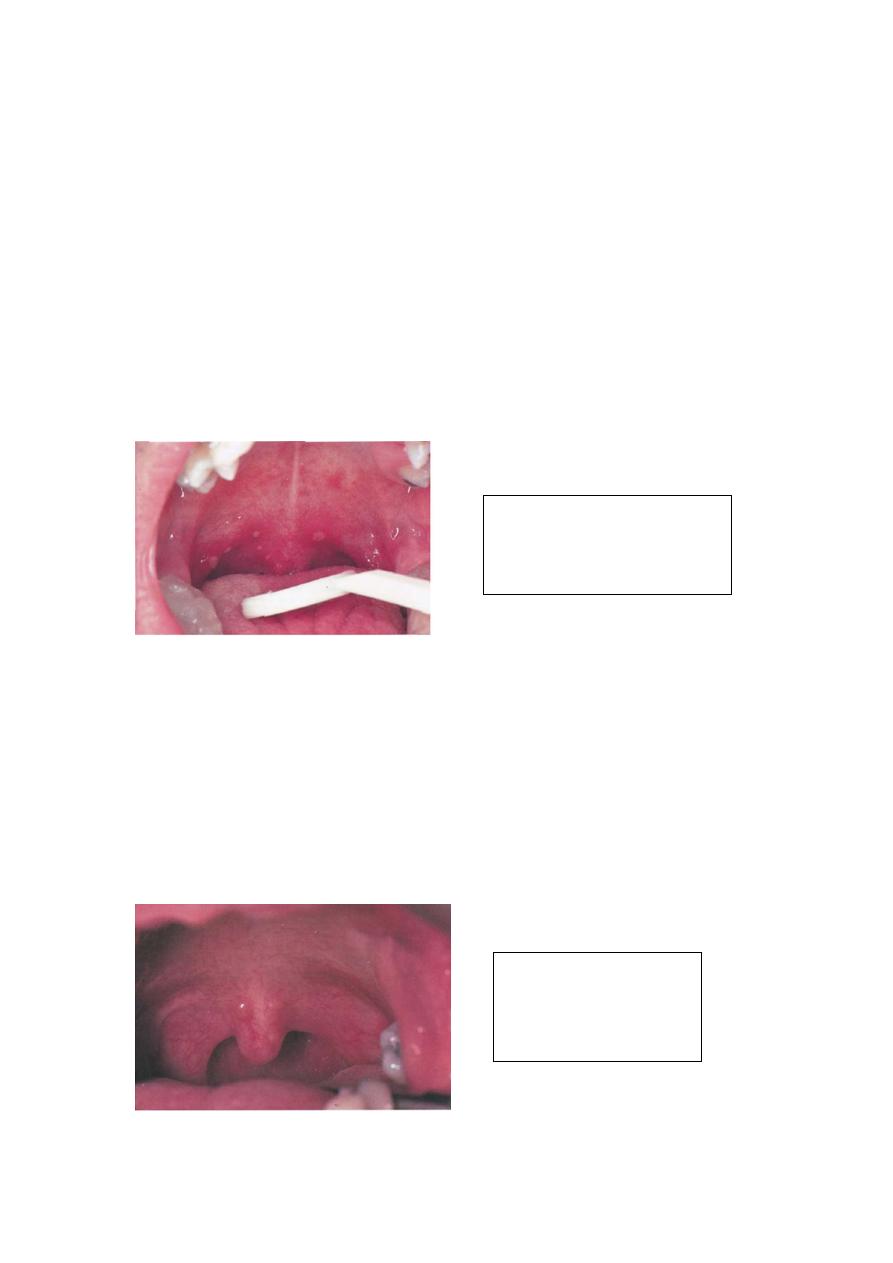
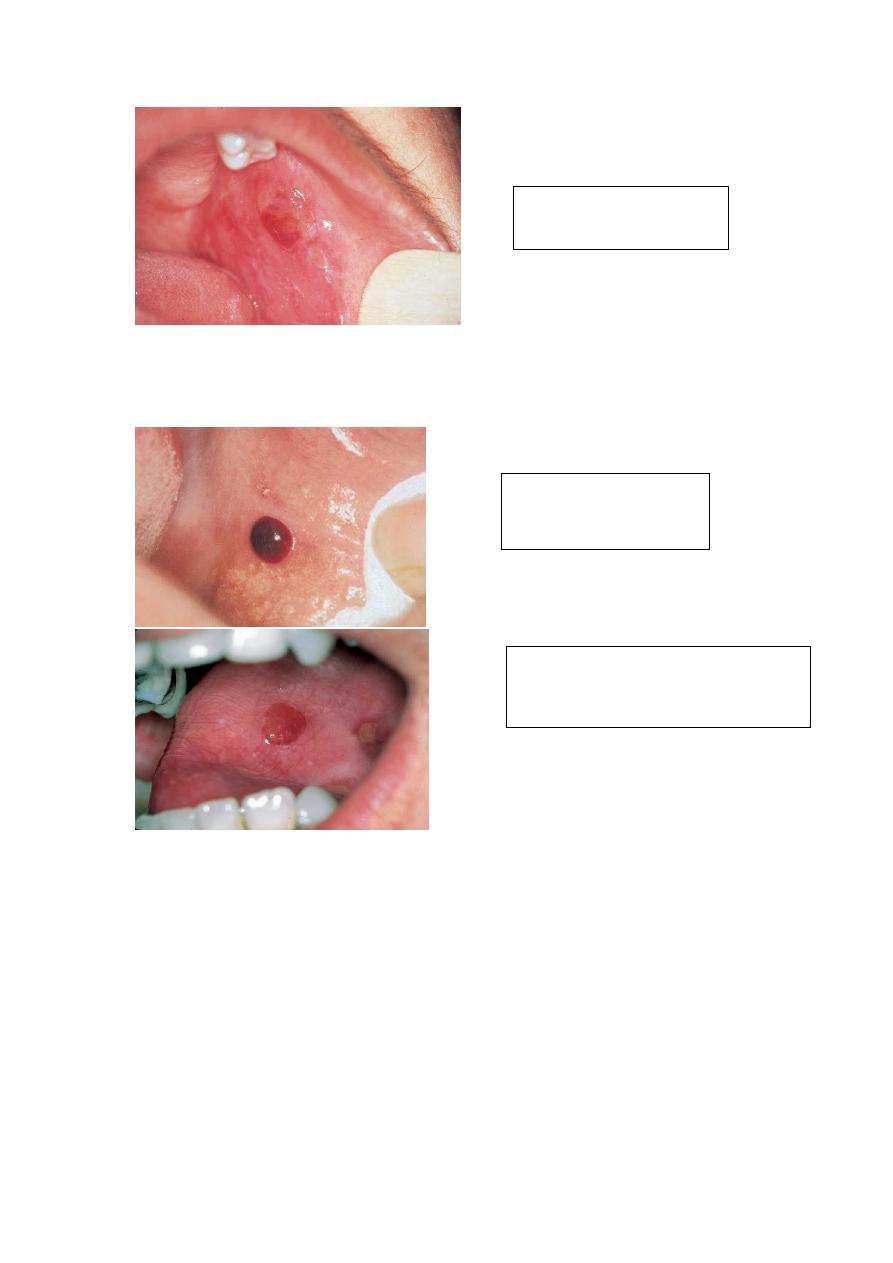
Multifocal area of ulceration &
erythema of the soft palate . The
patient report sore throat , fever ,
headache and vomiting
Tow pink nodules
immediately superior to the
uvula with lateral adjacent
erythema of the soft palat
Hand-Foot-And-Mouth Disease
Is caused by infection with coxsackie virus A16 . In a majority of cases,
the disease is characterized by
Low-Grade Fever
Oral Vesicles And Ulcers
Non pruritic Macules & Papules
Vesicles, Particularly On The Extensor Surfaces Of The Hands and Feet. mainly
the palm of the hand & sole of the feet
The oral lesions are more extensive than are those described for herpangina, and
lesions of the hard palate, tongue, and buccal mucosa are common .
Treatment: self-limiting disease & supportive care only is indicated
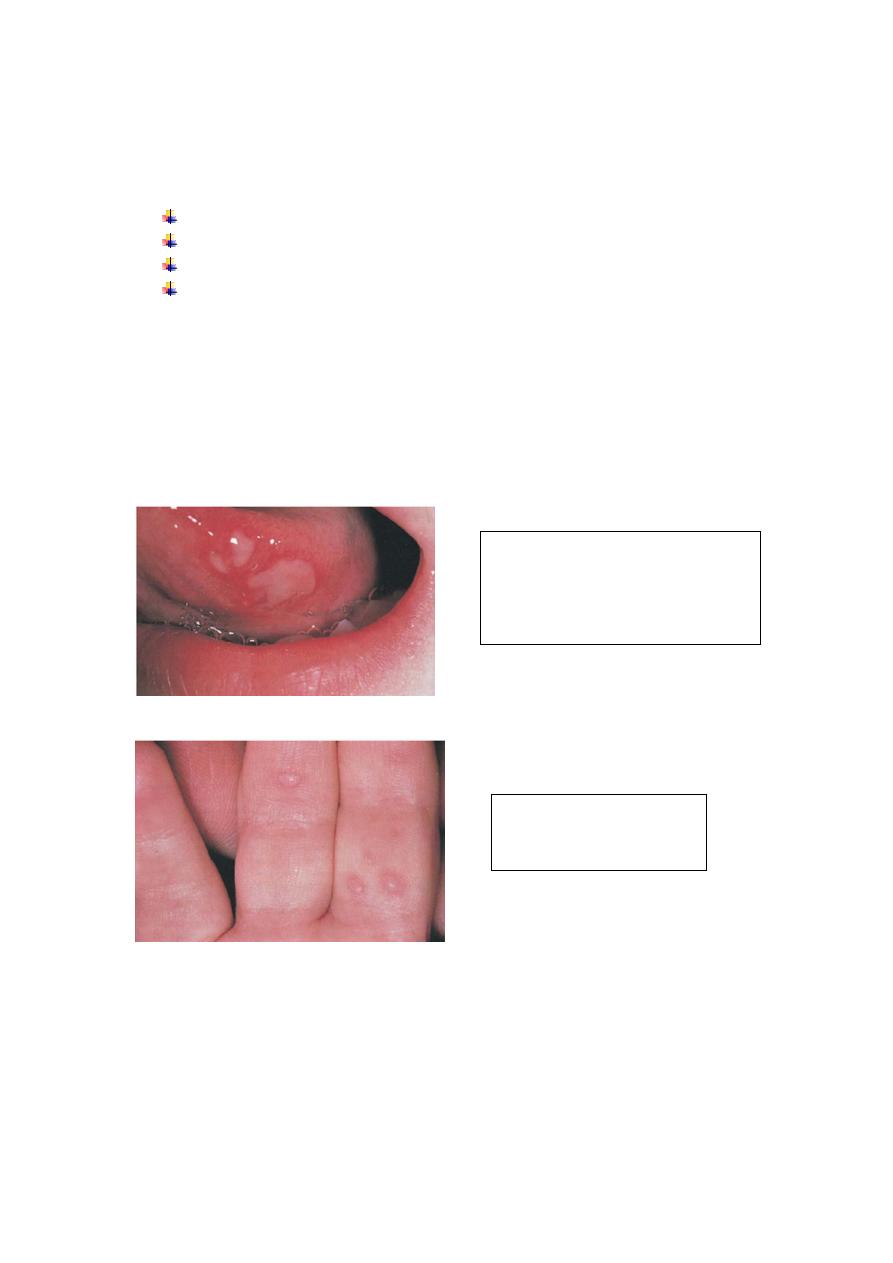
Multiple ulcer of the lateral tongue
In a 3year-old child who also had
Vesicular lesion of the fingers and toes
Multiple vesicles and
erythema of the fingers in
same patient

Pemphigus
Pemphigus is a potentially life-threatening disease that causes blisters and erosions of
the skin and mucous membranes. These epithelial lesions are a result of autoantibodies
that react with desmosomal glycoproteins that are present on the cell surface of the
keratinocyte .The immune reaction against these glycoproteins causes a loss of cell-to-
cell adhesion, resulting in the formation of intraepithelial bullae. The highest
incidence occurring in the fifth and sixth decades of life, although rare cases have been
reported in children and the elderly. Pemphigus occurs more frequently in the Jewish
population in whom studies have shown a strong association with major
histocompatibility complex (MHC) class II alleles HLA-DR4 and DQW3. Familial
pemphigus has also been reported.
The major variants of pemphigus:
pemphigus vulgaris (PV)
pemphigus vegetans
pemphigus foliaceus
pemphigus erythematosus,
Para neoplastic pemphigus (PNPP)
drug –related pemphigus.
Pemphigus vegetans is a variant of pemphigus vulgaris, and pemphigus
erythematosus is a variant of pemphigus foliaceus. Each form of this disease has
antibodies directed against different target cell surface antigens, resulting in a lesion
forming in different layer of the epithelium.In pemphigus foliaceus, the blister occurs
in the superficial granular cell layer, whereas, in pemphigus vulgaris, the lesion is
deeper, just above the basal cell layer. Mucosal involvement is not a feature of the
foliaceus and erythematous forms of the disease.
Pemphigus Vulgaris (PV)
Is the most common form of pemphigus, accounting for over 80% of cases. The
underlying mechanism responsible for causing the intraepithelial lesion of PV is the
binding of IgG autoantibodies to desmoglein 3, a trans membrane glycoprotein
adhesion molecule present on desmosomes. The presence of desmoglein 1
autoantibodies is a characteristic of pemphigus foliaceus, but these antibodies are also
detected in patients with long-standing PV. The mechanism by which anti desmoglein
antibodies cause the loss of cell-to-cell adhesion is controversial. Some investigators
believe that binding of the PV antibody activates proteases, whereas more recent
evidence supports the theory that the PV antibodies directly block the adhesion
function of the desmogleins. The separation of cells, called acantholysis, takes place
in the lower layers of the stratum spinosum [ prickle cell layer] .

Clinical Manifestations :
The classical lesion of pemphigus is a thin-walled bulla arising on otherwise normal
skin or mucosa. The bulla rapidly breaks but continues to extend peripherally,
eventually leaving large areas of denuded skin .A characteristic sign of the disease
may be obtained by application of pressure to an intact bulla. In patients with PV, the
bulla enlarges by extension to an apparently normal surface .Another characteristic
sign of the disease is that pressure to an apparently normal area results in the
formation of a new lesion. This phenomenon, called the Nikolsky sign, results from
the upper layer of the skin pulling away from the basal layer. The Nikolsky sign is
most frequently associated with pemphigus but may also occur in epidermolysis
bullosa.
Oral Manifestations :
Eighty to ninety percent of patients with pemphigus vulgaris develop oral lesions
sometime during the course of the disease, and, in 60% of cases, the oral lesions are
the first sign. The oral lesions may begin as the classic bulla on a non-inflamed base;
more frequently, the clinician sees shallow irregular ulcers because the bullae rapidly
break. Most commonly the lesions start on the buccal mucosa, often in areas of trauma
along the occlusal plane. The palate and gingiva are other common sites of
involvement. In some cases, the lesions may start on the gingiva and called
desquamative gingivitis. It should be remembered that desquamative gingivitis is not a
diagnosis in itself; these lesions must be biopsied to rule out the possibility of
*Pemphigus vulgaris
*Bullous pemphigoid
*Mucous membrane pemphigoid
*Erosive lichen planus
Laboratory Tests :
PV is diagnosed by [ Biopsy]
done on intact vesicles and bullae less than 24 hours old; however, because these
lesions are rare on the oral mucosa, the biopsy specimen should be taken from the
advancing edge of the lesion, where areas of characteristic supra basilar acantholysis
may be observed by the pathologist. Specimens taken from the center of a denuded
area are nonspecific histologically as well as clinically. Sometimes several biopsies are
necessary before the correct diagnosis can be made. If the patient shows a positive
Nikolsky sign, pressure can be placed on the mucosa to produce a new lesion; biopsy
may be done on this fresh lesion . A second biopsy, to be studied by DIF, should be
performed whenever pemphigus is included in the differential diagnosis .This study is
best performed on a biopsy specimen that is obtained from clinically normal-appearing
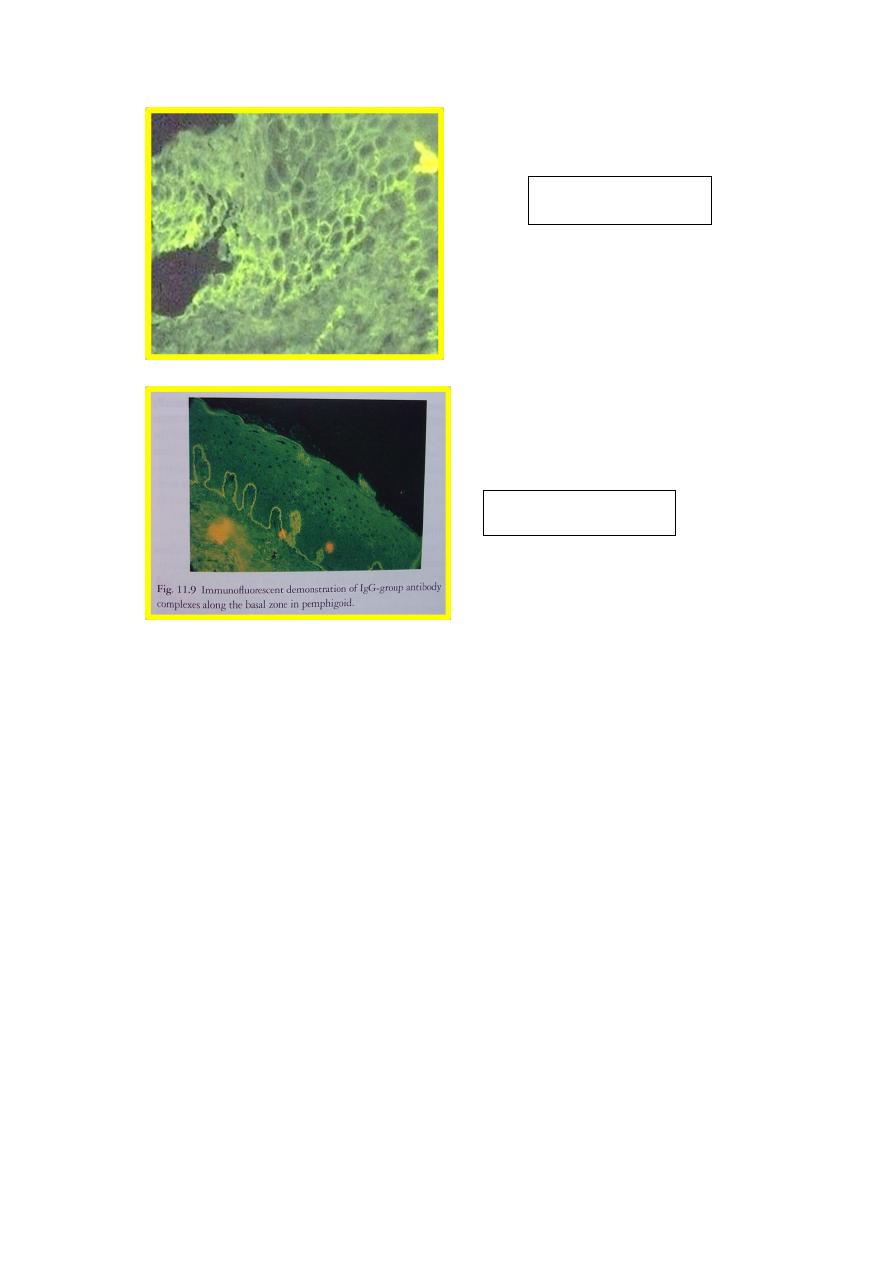
perilesional mucosa or skin. In this technique for DIF ,fluorescein-labeled antihuman
immunoglobulins are placed over the patient’s tissue specimen .In cases of PV, the
technique will detect antibodies, usually IgG and complement, bound to the surface of
the keratinocytes.
Indirect immune fluorescent antibody tests :
Have been described that are helpful in distinguishing pemphigus from pemphigoid
and other chronic oral lesions and in following the progress of patients treated for
pemphigus. In this technique, serum from a patient with bullous disease is placed over
a prepared slide of an epidermal structure (usually monkey esophagus). The slide is
then overlaid with fluorescein-tagged antihuman gamma globulin . Patients with
pemphigus vulgaris have anti keratinocyte antibodies against intercellular substances
that show up under a fluorescent microscope. The titer of the antibody has been
directly related to the level of clinical disease.
ELISA (enzyme-linked immune sorbent assay) :
Has been developed that can detect desmoglein 1 and 3 in serum samples of patients
with PV. These laboratory tests should provide a new tool for the accurate diagnosis of
PV and may also prove useful in monitoring the progress of the disease.
Treatment:
Corticosteroids
The mainstay of treatment remains high doses of systemic corticosteroids,
usually given in dosages of 1 to 2 mg/kg/d.
Adjuvant Therapy
When substantial doses of steroids must be used for long periods of time, adjuvant
therapy is recommended to reduce the steroid dose and their potential serious
complications. The most commonly used adjuvants are immunosuppressive drugs
such as mycophenolate mofetil, azathioprine [Imuran 50 mg] , or cyclophosphamide.
Prednisone is used initially to bring the disease under control, and once this is
achieved, the dose of prednisone is decreased to the lowest possible maintenance
levels.
The need for systemic steroids may be lowered further in cases of oral
pemphigus by combining topical with systemic steroid therapy, either by allowing
the prednisone tablets to dissolve slowly in the mouth before swallowing or by using
potent topical steroid creams.
Other therapies that have been reported as beneficial are
Parenteral gold therapy
Dapsone
Tetracycline
Plasma pheresis. is particularly useful in patients refractory to corticosteroids.
8-methoxypsoralen followed by exposure of peripheral blood to ultraviolet
radiation (therapy described by Rook and colleagues).
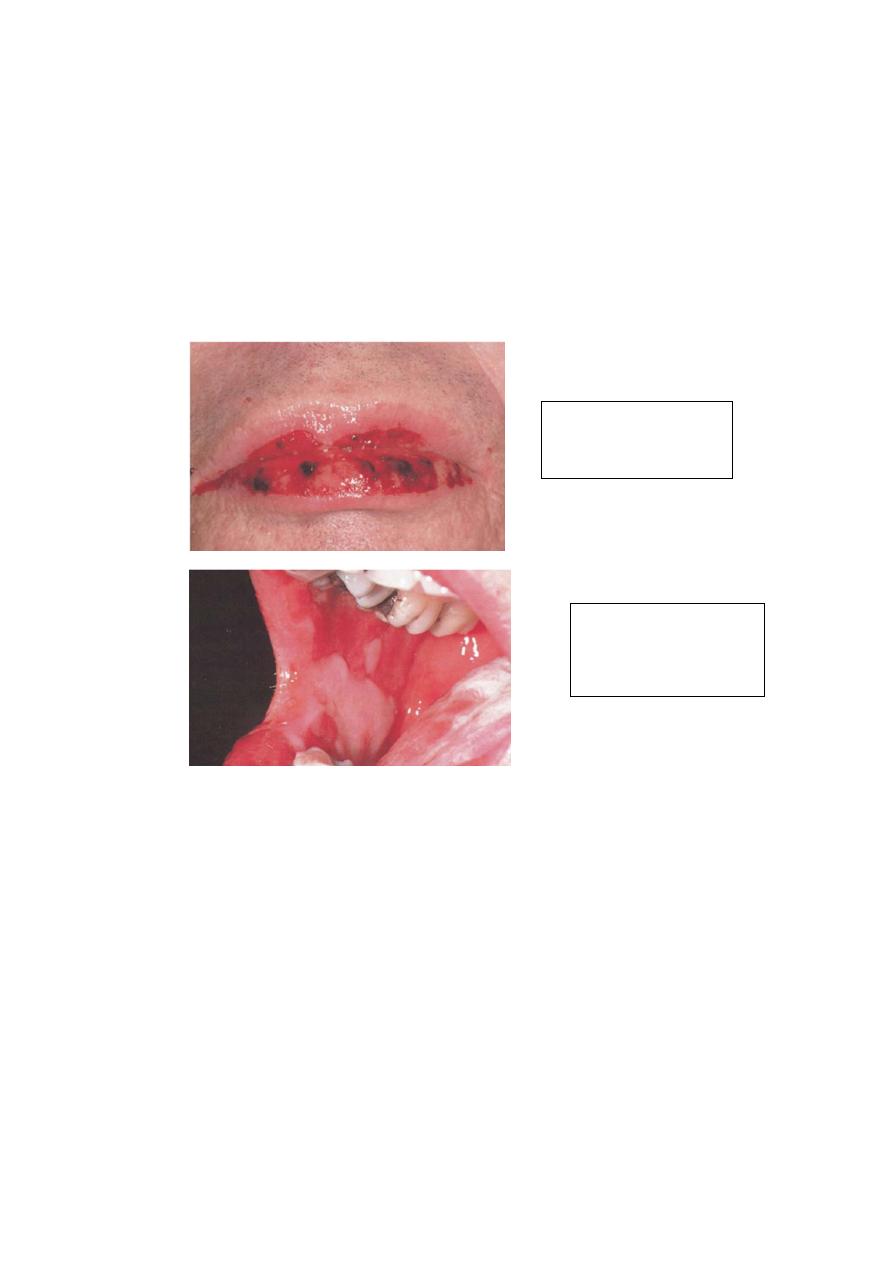
PARANEOPLASTIC PEMPHIGUS
PNPP is a severe variant of pemphigus that is associated with an underlying
neoplasm most frequently non-Hodgkin’s lymphoma, chronic lymphocytic leukemia,
are also associated with cases of PNPP. Patients with this form of pemphigus develop
severe blistering and erosions of the mucous membranes and skin . Treatment of this
disease is difficult, and most patients die from the effects of the underlying tumor,
respiratory failure due to acantholysis of respiratory epithelium, or the severe lesions
that do not respond to the therapy successful in managing other forms of pemphigus.
Drug-related Pemphigus like reactions
Drugs implicated in the induction of Pemphigus like reactions are
Ampicillin, procaine Penicillin , Benzyl Penicillin, Penicillamine , Piroxicam ,
Captopril , Diclofenac , Rifampicin , Gold salt & Garlic .
Subepithelial Bullous Dermatoses
Subepithelial bullous dermatoses are a group of mucocutaneous autoimmune
blistering diseases that are characterized by a lesion in the basement membrane zone.
The diseases in this group include
Para neoplastic
pemphigus , crusting
hemorrhagic lip lesion
Para neoplastic
pemphigus , extensive
erosive lesions of the
buccal mucosa

bullous pemphigoid (BP)
mucous membrane (cicatricial) pemphigoid (MMP)
linear IgA disease (LAD)
chronic bullous dermatosis of childhood (CBDC)
erosive and bullous lichen planus.
There is significant overlap among these diseases, and the diagnosis often depends
on whether the disease is categorized by clinical manifestations combined with
routine histopathology or the newer techniques of molecular biology. Recent
research into pathologic mechanisms is defining the specific antigens in the
basement membrane complex involved in triggering the autoantibody response.
Bullous Pemphigoid:
BP, which is the most common of the subepithelial blistering diseases, occurs
chiefly in adults over the age of 60 years; it is self-limited and may last from a few
months to 5 years. BP may be a cause of death in older debilitated individuals. BP
has occasionally been reported in conjunction with other diseases , particularly
multiple sclerosis and malignancy, or drug therapy, particularly diuretics.
In pemphigoid, the initial defect is not intraepithelial as in PV, but it is sub
epithelial in the lamina lucida region of the basement membrane . There is no
acantholysis, but the split in the basement membrane is accompanied by an
inflammatory infiltrate that is characteristically rich in eosinophils .
Mucous membrane pemphigoid (cicatricial pemphigoid)
MMP is a chronic autoimmune subepithelial disease that primarily affects the
mucous membranes of patients over the age of 50 years, resulting in mucosal
ulceration and subsequent scarring . The primary lesion of MMP occurs when
autoantibodies directed against proteins in the basement membrane zone, acting with
complement (C3) and neutrophils, cause a subepithelial split and subsequent vesicle
formation .
The antigens associated with MMP are most frequently present in the
lamina lucida portion of the basement membrane, but recent research has
demonstrated that the identical antigen is not involved in all cases, and the lamina
densa may be the primary site of involvement in some cases. The circulating
autoantibodies are not the same in all cases, and subsets of MMP have been
identified by the technique of immunofluorescent staining of skin that has been split
at the basement membrane zone with the use of sodium chloride. The latter antigen
has been identified in MMP in epiligrin (laminin 5), an adhesion molecule that is a
component of the anchoring filaments of the basement membrane.

Clinical Manifestations:
The subepithelial lesions of MMP may involve any mucosal surface, but they most
frequently involve the oral mucosa .The conjunctiva is the second most common site
of involvement and can lead to scarring and adhesions developing between the
bulbar and palpebral conjunctiva called symblepharon . Corneal damage is common,
and progressive scarring leads to blindness in close to 15% of patients. Lesions may
also affect the genital mucosa, causing pain and sexual dysfunction . Laryngeal
involvement causes pain, hoarseness, and difficulty breathing ,whereas esophageal
involvement may cause dysphagia, which can lead to debilitation and death in severe
cases. Skin lesions, usually of the head and neck region, are present in 20 to 30% of
patients .
Oral Manifestations:
Oral lesions occur in over 90% of patients with MMP. Desquamative gingivitis is
the most common manifestation and may be the only manifestation of the disease.
Since these desquamative lesions resemble the lesions of erosive lichen planus and
pemphigus, all cases of desquamative gingivitis should be biopsied and studied with
both routine histology and direct immunofluorescence to determine the correct
diagnosis . Lesions may present as intact vesicles of the gingival or other mucosal
surfaces, but more frequently they appear as nonspecific-appearing erosions. The
erosions typically spread more slowly than pemphigus lesions and are more self-
limiting.
Diagnosis:
Patients with MMP must have a biopsy done for both routine and direct immune
fluorescent study. Routine histopathology shows sub-basilar cleavage.
Using the direct immune fluorescent technique, biopsy specimens taken from MMP
patients demonstrate positive fluorescence for immunoglobulin and complement in
the basement membrane zone in 50 to 80% of patients. The direct immune
fluorescent technique is excellent for distinguishing MMP from pemphigus .Only
10% of MMP patients demonstrate positive indirect immunofluorescence for
circulating anti basement membrane zone antibodies .
Treatment:
Management of MMP depends on the severity of symptoms. When the lesions are
confined to the oral mucosa, systemic corticosteroids will suppress their formation.
Unlike pemphigus, MMP is not a fatal disease, and long-term use of steroids for this
purpose must be carefully evaluated, particularly because most cases are chronic, most
patients are elderly, and treatment is required for a long period of time .Patients with
mild oral disease should be treated with topical and intra lesional steroids
Desquamative gingivitis can often be managed with topical steroids in a soft dental
splint that covers the gingiva, although the clinician using topical steroids over large
areas of mucosa must closely monitor the patient for side effects such as candidiasis
and effects of systemic absorption. When topical or intra lesional therapy is not
successful, dapsone therapy may be attempted [ Since dapsone causes hemolysis and
methe-moglobinemia, glucose-6-phosphate dehydrogenase deficiency must be ruled
out and the patient’s hemoglobin must be closely monitored ]. Methemoglobinemia
can be reduced with the use of cimetidine and vitamin E. Another rare side effect of
dapsone is dapsone hypersensitivity syndrome. Patients resistant to dapsone should be
treated with a combination of systemic corticosteroids and immunosuppressive drugs ,
particularly when there is risk of blindness from conjunctival involvement, or
significant laryngeal or esophageal damage. Reports suggest that tetracycline and
nicotinamide may also be helpful in controlling the lesions of MMP .
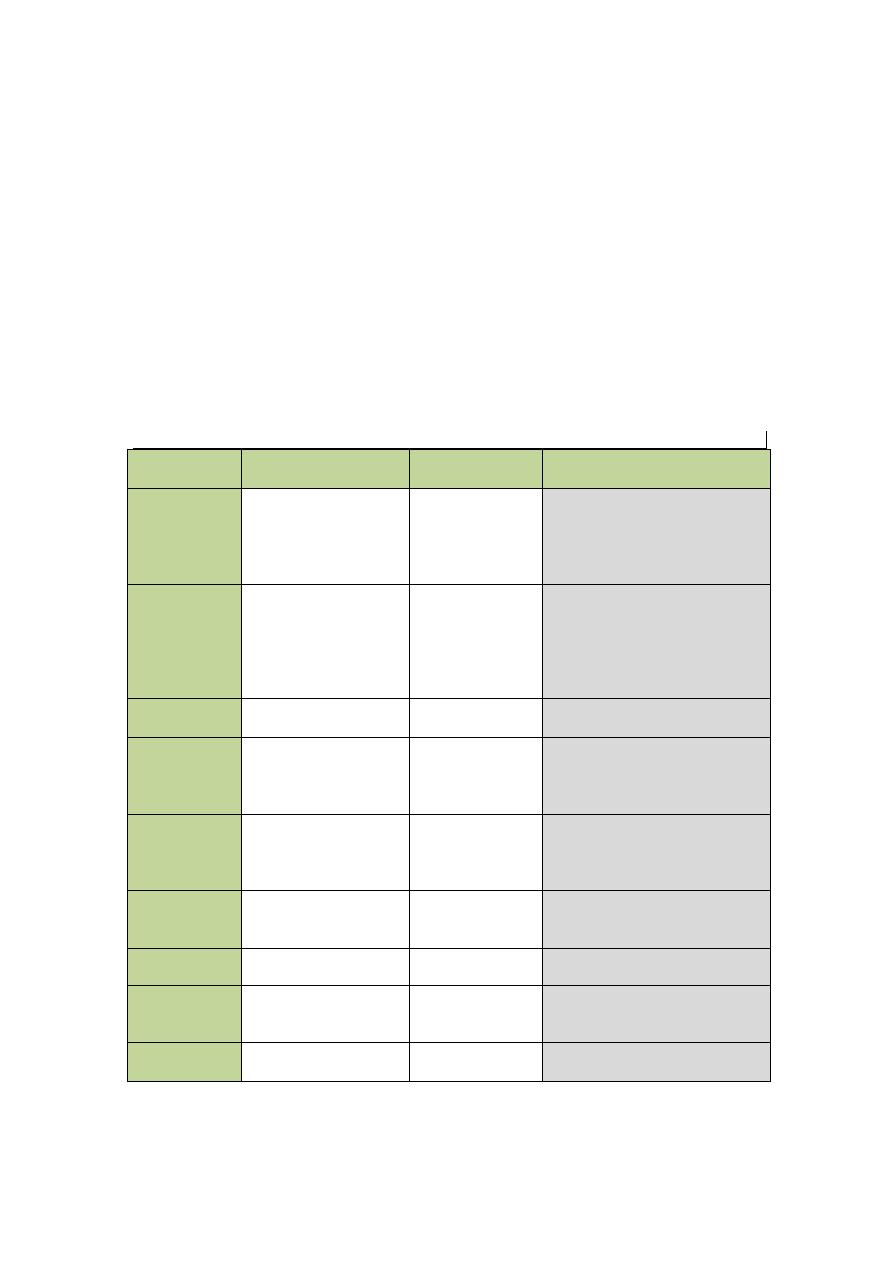
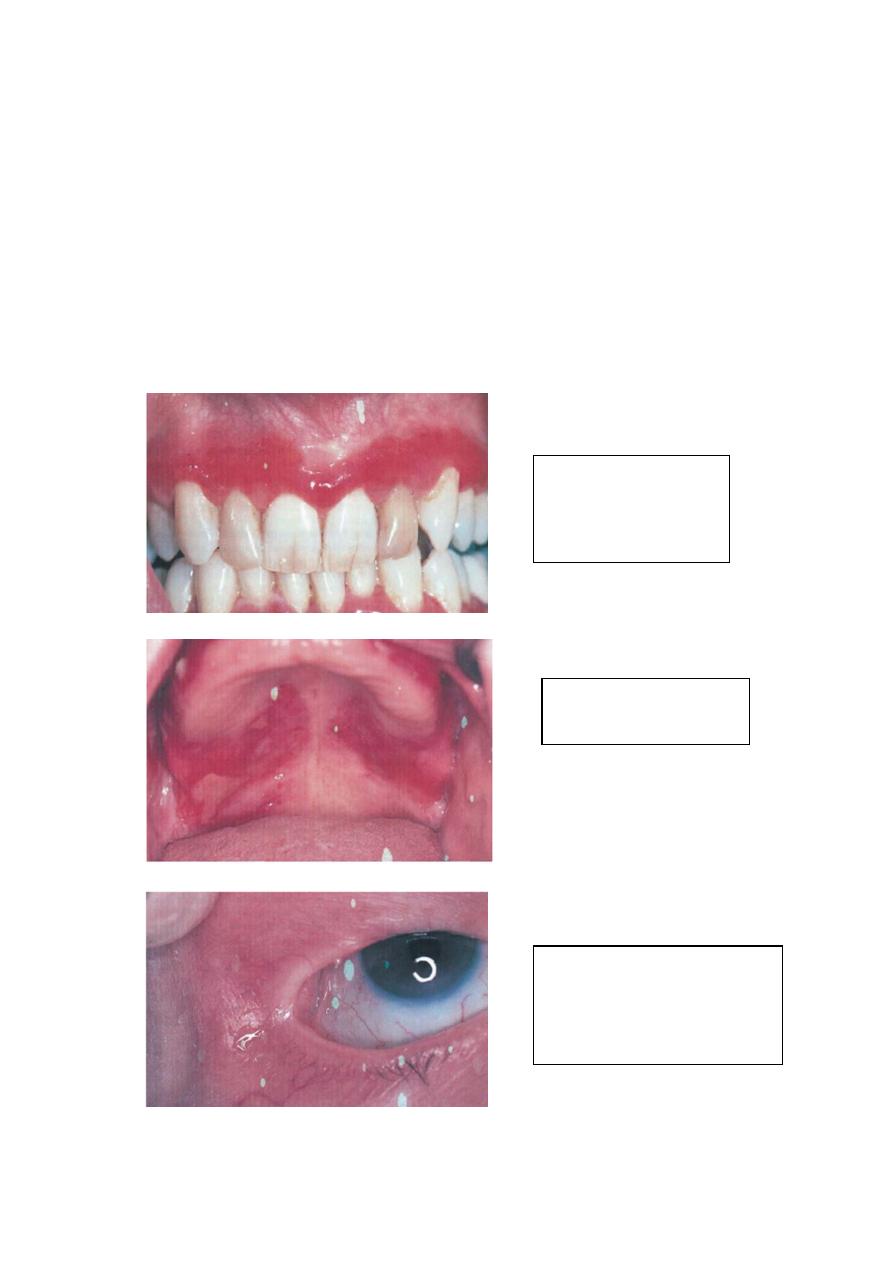
M.M.P
Erythematous &erosive
gingival lesion
[desquamative gingivitis]
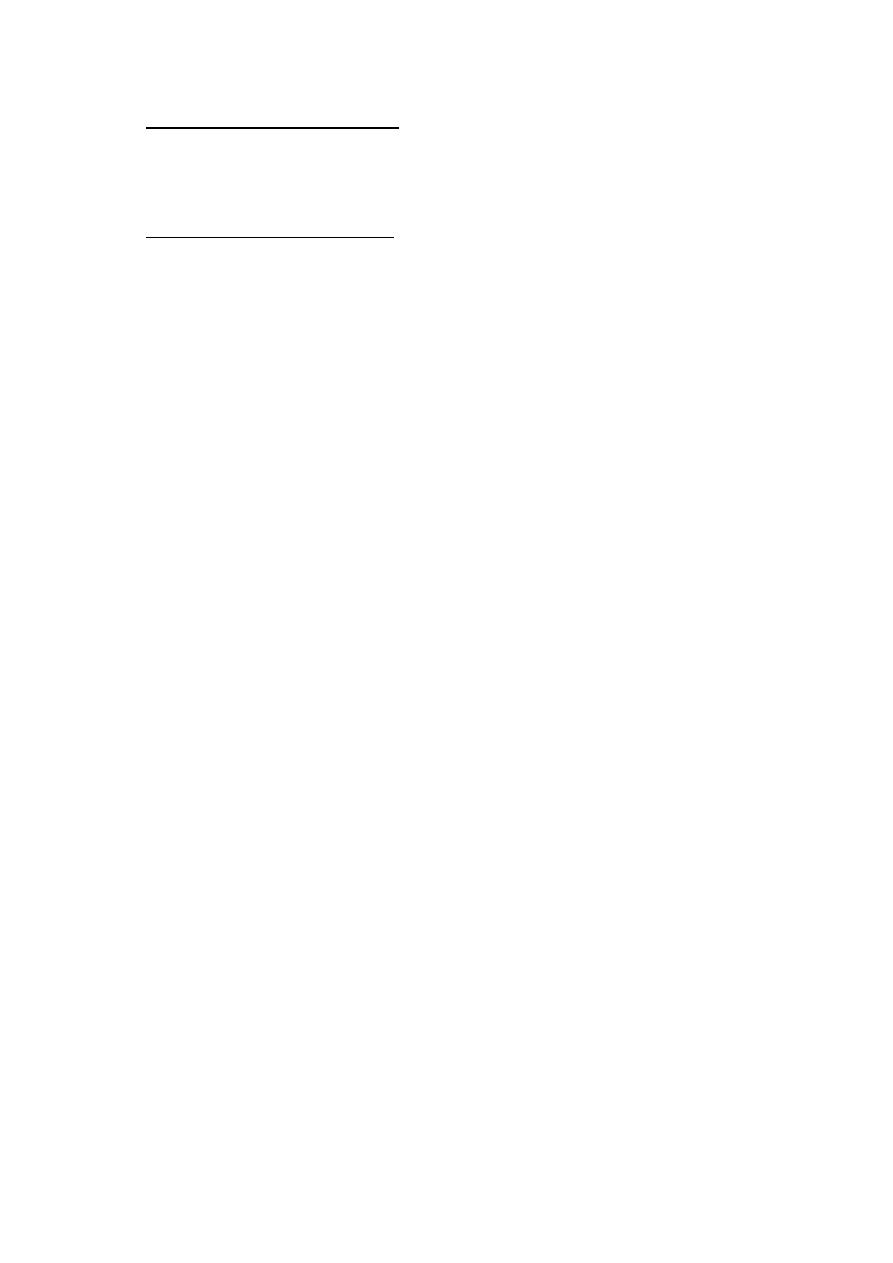
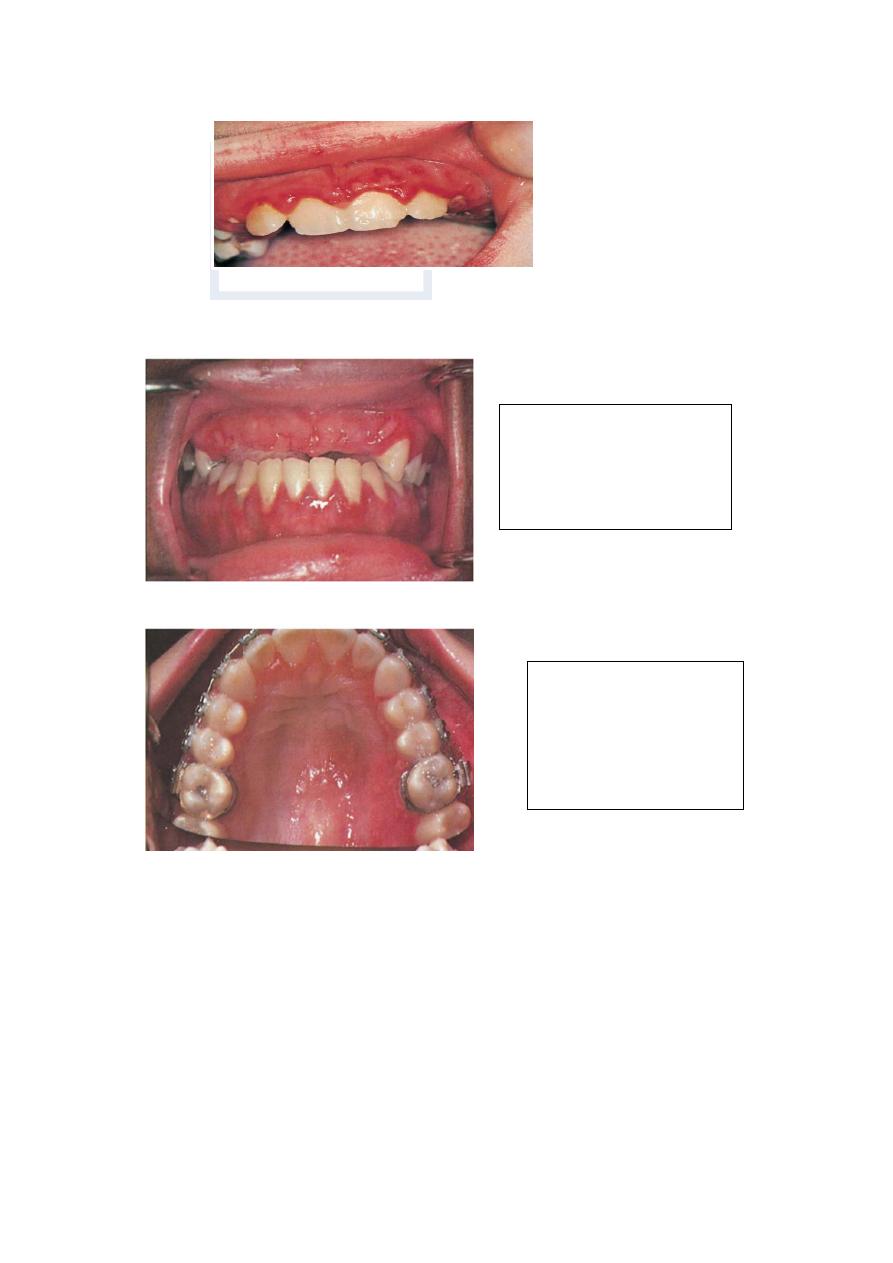
M.M.P
Lesion of the palate
M.M.P
Symblepharon formation of the
eye
Epidermolysis bullosa:
It is a dermmatological disorder in which bullae or vesicles occur on skin or
M.M surface spontaneously, shortly after minor trauma. There is defect in
attachment mechanism of epithelial cell .The term epidermolysis bullosa [EB] is
used for group of mechanobullos diseases characterized by the development of
blisters in area of minor trauma . At least 23 distinct forms of the disease have
been recognized . Most of these have a hereditary basis , with onset of blistering
lesions at birth or within the first few years of life . Epidermolysis bullosa
acquista is not hereditary , however , and appear to be an autoimmune disorder ,
with lesions typically arising during adolescence or adulthood . The various
types are characterized by spontaneous or trauma-induced blister formation
caused by
degeneration of basal or Para basal epithelial cells [EB simplex]
lack of hemi desmosome [junctional EB]
defects in anchoring fibrils in the connective tissue [dystrophic EB] .
Oral lesion are common in several types of EB present as bullae, usually in areas of
friction, which rupture, leaving shallow ulcers, and may result in painful erosion and
severe scarring . Enamel hypoplasia is a common finding in junctional forms of EB .
Rampant dental caries frequently is seen in patients with junctional EB and severe
Pemphigus Vulgaris
B.M.M. Pemphigoid
recessive dystrophic EB . Leukoplakia and squamous-cell carcinoma of the tongue has
been reported in several cases of recessive dystrophic EB. Skin lesions are characterized
by the formation of bullae, followed by ulcerations and scarring, particularly in areas
exposed to low-grade chronic trauma. Nail involvement, deformities of hands and feet,
milia formation, and involvement of the larynx, pharynx, and esophagus are common in
the recessive dystrophic type.
The prognosis for EB depends on the specific subtype of EB . EB letalis is usually fatal
during the first few months of life because of fluid loss and sepsis , dystrophic recessive
EB is often fatal before patients reach adulthood . Milder forms of EB are usually
compatible with a normal life span.
Treatment: Supportive. Systemic steroids in severe cases.
Classification:
Epidermolysis Bullosa Simplex
Epidermolysis bullosa Dystrophic, dominant.
Epidermolysis bullosa Dystrophic ,recessive.
Junctional Epidermolysis bullosa.
Epidermolysis bullosa acquisita (acquired)
Bullous Lichen Planus
Bullous lichen planus is a rare form of lichen planus . It is clinically characterized by
the formation of bullae that soon rupture, leaving painful shallow ulcerations .The
bullae usually arise on a background of papules or striae with the typical pattern of
lichen planus.
Dermatitis herpetiformis:
intact bulla on the lower lip
mucosa and small erosions
on the gingiva.
Lichen planus of the buccal
mucosa: bullous form.
Epidermolysis bullosa
simplex: hemorrhagic bulla
on the
buccal mucosa.
Epidermolysis bullosa, recessive
dystrophic form: bulla and scarring on
the tongue
.