INTER SEX
Fifth year
KEY POINT
Intersex people are individuals born with any or several variations in sex characteristic include:chromosomal like Turner syndrome
gonadal dysgenesis like Swyer syndrome
hormonal synthesis like congenital adrenal hyperplasia and 5alpha reductase deficiency
androgen receptor insensitivity either partial or complete
KEY POINT
Partial abnormalities usually lead to ambiguous gentile Any patient should be assessed:chromosomal genotype Phenotype
Internal and external gentile
Secondary sexual characteristics
Fitness for marriage
Fitness for pregnancy and childbirth
Role of surgery: diagnostic laparoscopy
Remove of gonad
Dilation of vagina
Plastic surgery
Chromosomal abnormalities
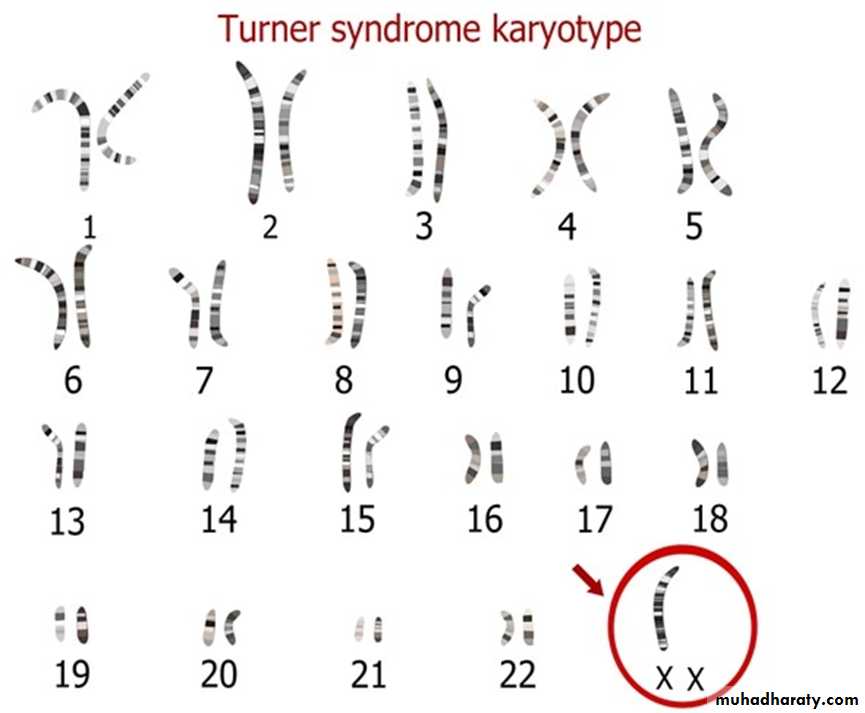
Turner syndrome
complete or partial absence of X chromosome (45x0)most common chromosomal abnormalities in females 1 in 2500 live female birth
clinical features: short stature, webbing of the neck and wide carrying angle. inverted widely spaced nipples, shield chest ,puffy hand and feet in baby due to lymphedema ,low hair line ,cubitus valgus ,short forth metacarpal .high arched palate ,micrognathia,defective dental development
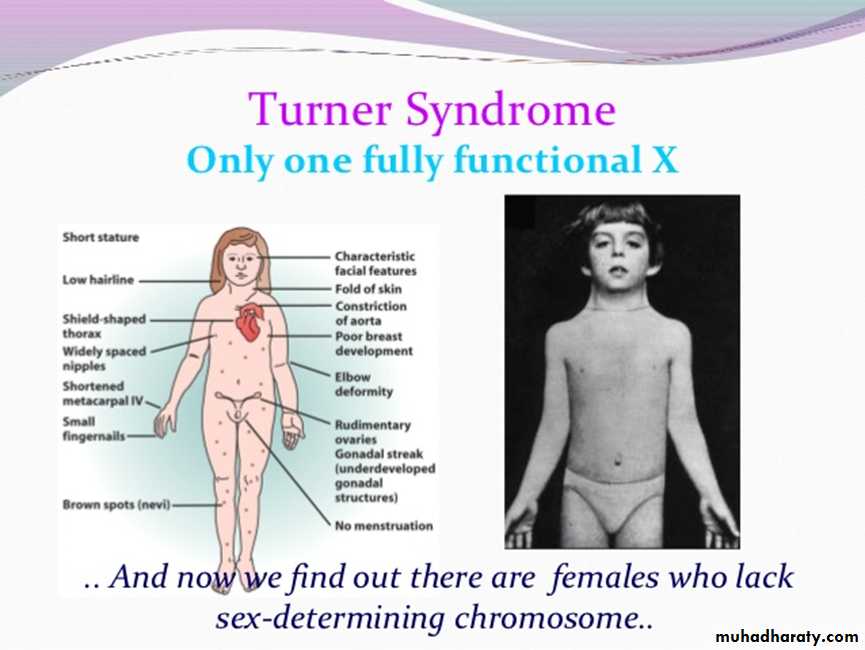
Normal intelligence
associated medical conditions: coarctation of the aorta, inflammatory bowel disease, sensorineural and conductive deafness, renal anomalies and endocrine dysfunctions such as autoimmune thyroid diseaseonly ovarian stroma present (streak gonads) do not function to produce estrogen or oocyte
diagnosis clinically short stature during childhood or during puberty (10%) due to delay puberty and absence of normal physical changes of puberty
treatment is focused on growth during childhood and on induction of puberty in adolescent
pregnancy is possible with ovum donation
47 XXX
Common Sexual development occurs normallyNormal or tall height
Academic performance is usually below average, there may be motor and speech delay and attention deficit
Premature ovarian failure and may present with secondary amenorrhea
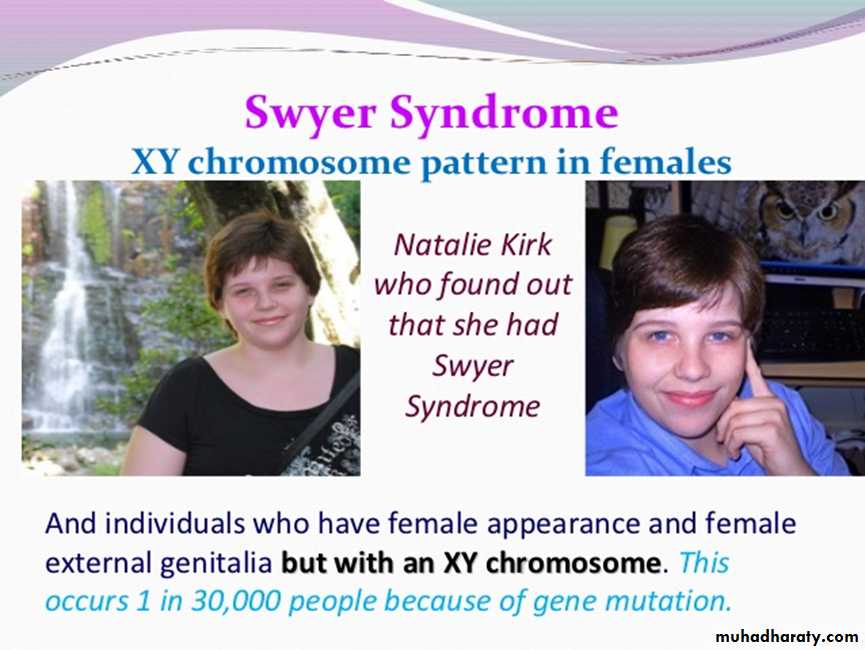
XY gonadal dysgenesis
XY gonadal dysgenesis
xy karyotype
absence of SRY gene in 10% but most cases the cause is unknown
complete gonadal dysgenesis (Swyer syndrome) the gonad remains as a streak gonad and does not produce any hormones
uterus, vagina and fallopian tubes develop normally due to absence of AMH (so Mullerian structures do not regress)
no virilization of the fetus and phenotype female due to absence of testosterone
failure of spontaneous puberty due to non-function gonad
the dysgenetic gonad has a high risk of malignancy so should be removed when the diagnosis is made
diagnosis: karyotype, laparoscopic biopsy of the gonad
puberty is induced by estrogen
pregnancy is reported with oocyte donation
Mixed gonadal dysgenesis
Is more complex, the karyotype may be 46 xx, mosaicism xx/xy is present in 20%
Both functioning ovarian and testicular tissue can be present (ovatesticular DSD
Anatomical finding vary according to functional gonad: virilize baby and ambiguous or normal male genitalia. mullerian structure are absent on one side of functioning testes, but unicornute uterus may be present if there is an ovary
46XY DSD
complete androgen insensitivity syndrome (CAIS) occurs in individuals where virilesation of external genitalia does not occur due to partial or complete inability of androgen receptor to respond to androgen stimulationin the fetus with CAIS testes form normally due to the action of SRYgen ,the testes secrete AMH leading to regression of Mullerian ducts .
CAIS woman do not have a uterus
female external genitalia due to failure of viliralazation because inability of androgen receptor to respond to testosterone
testes present at some point in their line of descend from abdomen
during puberty :normal breast development(circulating testosterone is peripherally converted to estrogen
Minimal axillary and pubic hair
Primary amenorrhea
Sometime Inguinal hernia in young girl (testes in inguinal canal)
46XY DSD
infertilegonadectomy is recommended because risk of malignancy
long term hormonal replacement therapy
vaginal dilator or surgical vaginal reconstruction surgery for penetrative intercourse
In partial androgen insensitivity limited virilization and the diagnosis at birth with ambiguous genitalia
5-Alpha-reductase deficiency
XY karyotypenormal function testes produce both testosterone and AMH
the fetus unable to convert testosterone to dihydrotestosterone in the peripheral tissue and cannot virilize normally
Presentation: ambiguous genitalia at birth or increase virilization at puberty due to large increase of testosterone with the onset of puberty
assigned female sex of rearing
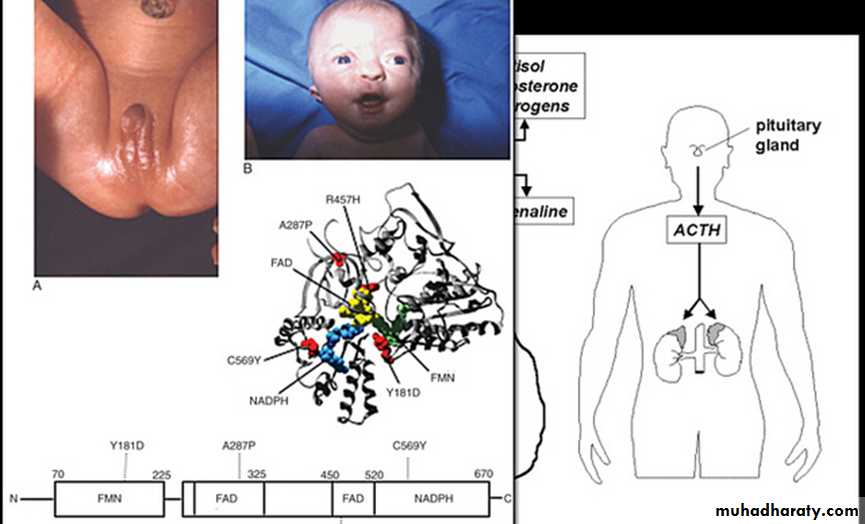
Congenital adrenal hyperplasia
it is due to an enzyme deficiency in the corticosteroid production pathway in the adrenal gland with over 90%being deficiency in 21-hydroxylase ,which convert progesterone to deoxycorticosterone ,and 17-hydroxyprogestrone to deoxycortisoladrenal hyperplasia as response to reduce level of cortisol
increase progesterone production, this lead to increase androgen precursor and then elevated testosterone.
raised androgen levels in female fetus will lead to virilization of external genitalia: the clitoris is enlarged and the labia are fused and scrotal in appearance ,the upper vagina join to the urethra and open as one common channel onto perineum
two third of children with 21 OH CAH will have salt losing variety ,which also affect the ability to produce aldosterone which is life threatening condition
life long steroid replacement such as hydrocortisone along with fludrocortisone for salt loser
surgical correction of external genitalia (feminizing genital surgery

Q 1
A mother bring her 15th year old daughter complaining of primary amenorrhea past medical history negative apart from inflammatory bowel disease and on examination short stature with micrognathiawhat is the professional diagnosis
what are other clinical features that support our diagnosishow do you investigate this patient
Is surgery help this girlA worried mother ask you about the future of her daughter regarding menstruation and possibility of marriage and pregnancy
Q2
you are obstetrician on call 30-year-old female with negative past medical history gave birth to a baby with ambiguous genitalia the female was surprised and become depressed so decide to go home and and come back later for investigation .Do you agree ?
how to investigate the fetus
give three possible differential diagnosis to this infant