Coll. Medicine \3rd stage
ParasitologyAssist. Prof. Dr. Amal KH. KH.
Lec.6
Class (4) : Sporozoa (Coccidia)
The locomotion of a mature organism is by body flexion, gliding, or undulation of longitudinal ridges. The genus Plasmodium that are the causes of malaria is the prototype of this class. The members of class sporozoa belong to two order and include :order : Haemosporida : include blood species
Plasmodium spp.
Babesia sp.
order : Eucoccida : include intestinal and tissue species
Toxoplasma gondii (tissue species)
Isospora belli
Cyclospora sp.
Cryptosporidium parvum
Sarcocystis sp.
Microsporidia sp.
Malaria :
There are four species normally infecting humans, namely, Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, and Plasmodium malariae. P. falciparum causes the most fulminate disease . almost the death of malaria are due to P. falciparum . P. falciparum is the most dangerous of the 4 species. It causes a high level of parasitemia with parasite density exceeding 250,000-300,000 /ml of blood. Nearly 30-40% of RBCs may be infected. In contrast to other species, it invades erythrocytes of all ages (old and young).
Morphology :
There are various morphological forms of malarial parasites . out of the these are occur in human and the other in mosquitoes:Morphological forms seen in human :
1. forms in liver:
Sporozoites :these forms are slender, banana shaped and are infective forms for humans from mosquitoes.
Merozoites : are the end- product of schizogony the merozoites . the merozoites come out from liver and enter RBC to initiate the erythrocytic shcizogony . it is very difficult to demonstrates these form in liver because very few hepatic are affected.
2- forms in RBC :
Trophozoites : young trophozoites called ring forms . they have a vacuole in the centre . at a later they are called amoeboid forms .
Schizonts : this form occur inside RBC after asexual multiplication by dividing of nucleus without cytoplasm and this called immature schizont , after this ,cytoplasm condensed around each daughter nucleus to became mature schizont , each newly formed nucleus along with the surrounding cytoplasm covered with a cell membrane . these newly formed morphological forms are merozoites .
Merozoites . the number of merozoites varies from 8 to 32 depending on the species of plasmodium. Merozoites infects other RBC to repeat schizogony .
Gametocytes : there are two types of gametocytes formed by gametogony inside RBC and include female gametocytes or macogametes and male gametocytes or microgametes.
Morphological forms seen in mosquitoes :
Macrogametes : the female gametocytes mature in the mid – gut of mosquito to develop into female gamete . one gametocyte develop to one gamete .Microgametes : one microgametocyte produced 6 to 8 male gametes be a process of exflagellation in the mid-gut of mosquitoes.
Ookinete : a male gamete fertilize female gamete to form a diploid zygote (syngamy) . the zygote quickly elongates to become a motile ookinete .
Oocyst : ookinete penetrates the gut wall and comes to lie on the haemocoel side of gut , where it develop into oocyst .
Sporozoites: meiosis (nuclear reduction division) in the oocyst results in development of haploid forms called sporozoites . sporozoites break out of the oocyst into the haemocoel . they reach the salivary gland of the mosquitoes to become infective form to human .
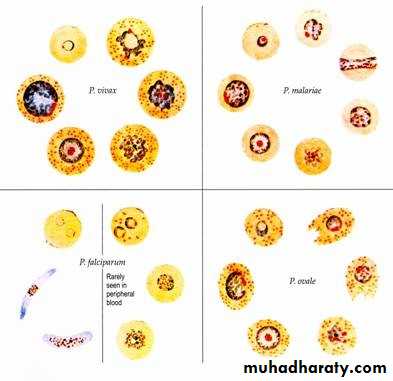
Plasmodium falciparum :
Plasmodium falciparum demonstrates no selectivity in host erythrocytes, i.e. it invades young and old RBCs cells. The infected red blood cells also do not enlarge and become distorted.
Multiple merozoites can infect a single erythrocyte, and show multiple infections of cells with small ring forms.
The trophozoite is often seen in the host cells at the very edge or periphery of cell membrane at accole position.
Occasionally, reddish granules known as Maurer’s dots are observed
Mature (large) trophozoite stages and schizonts are rarely seen in blood films, because their forms are sequestered in deep capillaries, liver and spleen.
Peripheral blood smears characteristically contain only young ring forms and occasionally crescent shaped gametocytes.
Plasmodium vivax:
P.vivax is selective in that it invades only young immature erythrocytes. Infections of P. vivax have the following characteristics:
Infected red blood cells are usually enlarged and contain numerous pink granules or schuffner’s dots.
The trophozoite is ring-shaped but amoeboid in appearance.
More mature trophozoites and erythrocytic schizonts containing up to 24 merozoites are present.
The gametocytes are round.
Plasmodium ovale:
P. ovale is similar to P. vivax in many respects, including its selectivity for young, pliable erythrocytes. As a consequence the classical characteristics include:• The host cell becomes enlarged and distorted, usually in an oval form.
• Schiffner’s dots appear as pale pink granules.
• The infected cell border is commonly fimbriated or ragged
• Mature schizonts contain about 10 merozoites.
Plasmodium malariae:
In contrast with P.vivax and P.ovale, P.malariae can infect only old erythrocytes with relatively rigid cell membranes. As a result, the parasite’s growth must conform to the size and shape of red blood cell. This requirement produces no red cell enlargement or distortion, but it results in distinctive shapes of the parasite seen in the host cell, “band and bar forms” as well as very compact dark staining forms. The schizont of P.malariae is usually composed of eight merozoites appearing in a rosette.
Mode of malaria transmission :
Man gets infection mainly by the bite of infected female Anopheles mosquito. However, infection may also be transmitted by:Transfusion malaria: malaria can be transmitted in blood . the infective forms are merozoites and RBC stages except the gametocytes.
Congenital malaria: also called transplacental malaria and occur through defect of placenta .the infection acquired during childbirth but the parasitemia are reduced in the infected newborn by passively transferred IgG from immune mother.
By the use of contaminated syringes particularly in drug addicts.
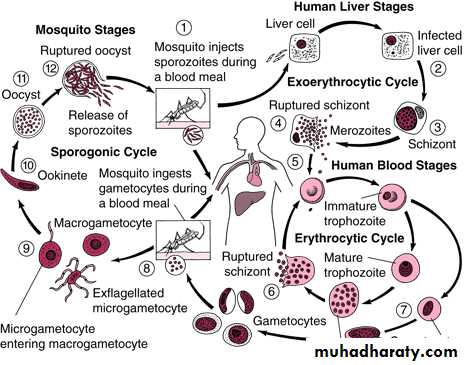
Life cycle
The life cycle of malaria is complex passed in two hosts (alternation of hosts) and has sexual and asexual stage (alternation of generations).Vertebrate host - man (intermediate host), where the asexual cycle takes place. The parasite multiplies by schizogony and there is formation of male and female gametocytes (gametogony).
Invertebrate host – female mosquito of genus Anopheles (definitive host) where the sexual cycle takes place. Union of male and female gametes ends in the formation of sporozoites (sporogony).
The life cycle passes in four stages:
Three in man:-
- Pre (exo )- erythrocytic schizogony.
Erythrocytic schizogony.
Gametogony.
One in mosquito – Sporogony.
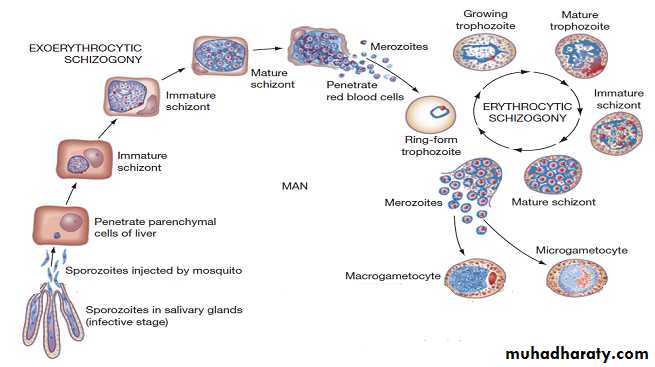
Introduction into humans - when an infective female Anopheles mosquito bites man, it inoculates saliva containing sporozoites (infective stage).
Pre- Erythrocytic schizogony - :
Sporozoites reach the blood stream and within 30 minutes enter the parenchymal cells of the liver, initiating a cycle of schizogony. Multiplication occurs in tissue, to form thousands of tiny merozoites from the schizont. Merozoites are then liberated on rupture of schizonts about 7th – 9th day of the bites and enter into the blood stream. These merozoites either invade the RBC’s or other parenchymal liver cells. In case of P. falciparum and possibly P. malariae, all merozoites invade RBC’s without re-invading liver cells. However, for P. vivax and P. ovale, some merozoites invade RBC’s and some re-invade liver cells initiating further Exo-erythrocytic schizogony,. Some of the merozoites remain dormant (hypnozoites) becoming active later on which is responsible for relapses.
Erythrocytic schizogony (blood phase) is completed in 48 hrs in P. vivax, P. ovale, and P. falciparum, and 72 hrs in P. malariae. The merozoites reinvade fresh RBC’s repeating the schizogonic cycles Erythrocytic merozoites do not reinvade the liver cells. So malaria transmitted by blood transfusion reproduces only erythrocytic cycle .
Gametogony :
Some merozoites that invade RBC’s develop into sexual stages (male and female gametocytes). These undergo no further development until taken by the mosquito.
Sporogony (extrinsic cycle in mosquito) :
When a female Anopheles mosquito vector bites an infected person, it sucks blood containing the different stages of malaria parasite. All stages other than gametocytes are digested in the stomach. The microgametocyte undergoes ex-flagellation. The nucleus divides by reduction division into 6-8 pieces, which migrate to the periphery. At the same, time 6-8 thin filaments of cytoplasm are thrust out, in each passes a piece of chromatin. These filaments, the microgametes, are actively motile and separate from the gametocyte. The macrogametocyte by reduction division becomes a macrogamete. Fertilization occurs by entry of a micro gamete into the macro gamete forming a zygote. The zygote changes into a worm like form, the ookinete, which penetrates the wall of the stomach to develop into a spherical oocyst between the epithelium and basement membrane. The oocystes increase in size. Thousands of sporozoites develop inside the oocysts. Oocysts rupture and sporozoites are liberated in the body cavity and migrate everywhere particularly to the salivary glands. Now the mosquito is infective. The sporogonous cycle in the mosquito takes 8-12 days depending on temperature .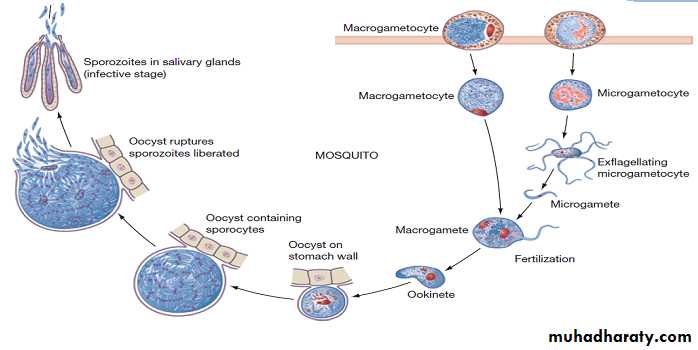
Recurrence of malaria :
This occur in malaria either from reinfection or due to certain events related to the life cycle of parasite . two type of recurrence are known in malaria :malaria recrudescence : in which the erythrocytic form of parasite may evade the host immunity and survive for months even after the clinical illness has subsided . the number of these forms may increase later leading to reappearance of clinical symptoms and signs within a year or two . this situation occur in P.falciparum.
malaria relapse :In case of P.vivax and P.ovale some sporozoites enter the hepatocytes and become dormant (resting) known as hypnozoite. After a period of time, up to two years, hypnozoites are reactivated to become secondary exo-erythrocytic schizonts and release merozoites that infect RBCs producing malaria relapse.
Pathology and clinical features of malaria :
All the pathology associated with malaria caused by asexual multiplication of plasmodia in bloodstream (erythrocytic schizogony ) . There are certain people, who are resistant to malaria infection, including those with:
Duffy antigen blood group negative (esp. for vivax).
Sickle cell traits.
Thalassemia.
Glucose-6-phosphate-dehydrogenase deficiency.
After an incubation period of 12 days for P.falciparum, 13-17 days for P.vivax, and P. ovale, and 28-30 days for P. malariae, patient will develop typical picture of malaria that consists of: Febrile paroxysm, Anaemia, Splenomegaly and jaundice .
Febrile paroxysm:
It generally begins in the early afternoon and comprises of 3 stages;cold stage : 15-60 min, the patient experiences intense cold and shivering.
hot stage : lasting for 2-6 hours, when the patient feels intense hot. Patient develops high fever (40-41 C), severe headache, nausea, and vomiting.
sweating stage.: fever ends by a crisis of profuse sweating.
Periodic fever (Febrile paroxysm ) in malaria is characteristic . it is related to life cycle of parasite . usually the erythrocytic schizogony is synchronous ; this means that schizogony begins and ends at the same time in all infected RBC in a particular cycle. Thus , at the end of each erythrocytic cycle all the infected RBC rupture at the same time . this releases toxic waste by –products along with merozoites . macrophages engulf merozoites (some merozoites escape from macrophages to repeat the erythrocytic schizogony ) . the macrophage release interleukin -1 which is act on thermo-regulatory centre situated in brain , to set it at higher temperature (41 Cْ or higher ) . the normal body temperature of 37 is now considered low by the thermo- regulatory centre . the patient at this stage feels cold. The thermo- regulatory activates temperature raising mechanism in the form of shivering . the mascular constructions leads to rise in the body temperature upto the set mark in the thermo- regulatory centre (41 Cْ or higher ). The feeling of coldness, attending with shivering is called chill . the consequent raising of body temperature is fever.
Subsequently , the IL-1 level in blood falls . the thermo-regulatory centre is reset at the normal body temperature of that individual . now, the patient feel hot , severe headache, nausea, and vomiting . the thermo- regulatory centre activates temperature reducing mechanism . patients sweats profusely , leading to a drop in his body temperature bringing it back to normal . the patient feel s tired and generally sleep at the end of this episode.. this episode consisting of chill – fever – sweating is typical of malaria fever.
These paroxysms usually reappear periodically (generally every 48 hours) as the cycle of infection, replication, and cell lyses progresses , so it is tertian in the case of :
Plasmodium falciparum.(malignant tertian malaria)
Plasmodium vivax (benign tertian malaria)
Plasmodium ovale (benign tertian malaria)
While paroxysms usually reappear periodically (generally every 48 hours) as the cycle of infection, replication, and cell lyses progresses every 72 hours in the case of Plasmodium malariae (quatrain malaria )
Anaemia after few paroxysms, anemia of microcytic or normocytic hypochromic type develops as a result of:
Mechanical destruction of parasitized RBCs.
Reduced erythropoiesis in the bone marrow.
Lysis and phagocytosis of uninfected RBCs.
In a small number of patients with malignant tertian malaria there is autoimmune destruction of RBCs.
Consumption of more than 70% of haemoglobin in RBCs by the parasite.
Failure of the liver to convert liberated iron.
Splenomegaly: After few paroxysms, spleen gets enlarged and becomes palpable. Splenomegaly is due to massive proliferation of macrophages which phagocytize both parasitized and non-parasitized RBCs.
Jaundice : can also occur due to rupture of RBCs.
Clinical features :
Plasmodium falciparum :Sever malaria (malignant ) is caused by P. falciparum may be fatal , hence it is called pernicious malaria . Of all the four Plasmodia, P. falciparum has the shortest incubation period, which ranges from 7 to 10 days. After the early flu-like symptoms, P.falciparum rapidly produces daily (quotidian) chills and fever as well as severe nausea, vomiting , diarrhea and bleeding from gum, nose and GIT . The periodicity of the attacks then becomes tertian (48 hours), and fulminating disease develops which is include :
Involvement of the brain (cerebral malaria) is most often seen in P.falciparum infection. Capillary plugging from an adhesion of infected red blood cells with each other and endothelial linings of capillaries causes hypoxic injury to the brain that can result in coma and death.
Kidney damage is also associated with P.falciparum malaria, resulting in an illness called “black water” fever (dark red to blackish urine). Intravascular hemolysis with rapid destruction of red blood cells produces a marked hemoglobinuria and can result in acute renal failure, tubular necrosis, nephrotic syndrome, and death.
Liver involvement is characterized by abdominal pain, vomiting of bile, hypoglycemia , hepatosplenomegally, severe diarrhea, and rapid dehydration.
Hypotension \ shock : also called Algid Malaria resembles surgical shock with cold clammy skin, peripheral circulatory failure and profound shock.
Pregnant women have an increased risk of abortion, stillbirth, premature delivery and of low birth weight of their infants.
Treatment:
Plasmodium falciparum:Because chloroquine – resistant stains of P.falciparum are present in many parts of the world, infection of P.falciparum may be treated with other agents including mefloquine, quinine, guanidine, pyrimethamine – sulfadoxine, and deoxycycline.
Plasmodium vivax and Plasmodium ovale:
Chloroquine is the drug of choice for the suppression and therapeutic treatment of P.vivax, followed by premaquine for radical cure from relapse and elimination of gamatocytes.
The treatment regimen with P. ovale, including the use of primaquine to prevent relapse from latent liver stages is similar to that used for P.vivax infection.
Plasmodium malariae :
Treatment is similar to that for P.vivax and P.ovale.
Diagnosis :
Clinical picture is highly suggestive, esp. the characteristic paroxysm.
Ab detection can detect past (not active) infections.
Rapid Diagnostic tests (RDTS) are based on detection of Ag derived from lysed blood cells using immunochromatographic methods.
Molecular diagnostic techniques can complement other tests, esp. in species identification like PCR
Microscopic identification of parasite (stages) in blood film is the method most frequently used to demonstrate an active infection through thick and thin smear stained with geimsa , Leishman and wright ُ s Romanowsky stain (contains azure dyes and eosin). as follow :
Stages in thick smears :
Control & Prevention :
Spraying insecticides.Spraying larvicides in breeding sites.
Using biological larvicides .
Wearing long sleeve clothing and trousers to avoid bites.
Using bed nets.
Early diagnosis and prompt treatment of patients.