Transverse problems
Posterior cross bite
The term “cross bite” means an abnormal labio lingual, edge to edge or
bucco lingual relationship of the antagonist teeth.
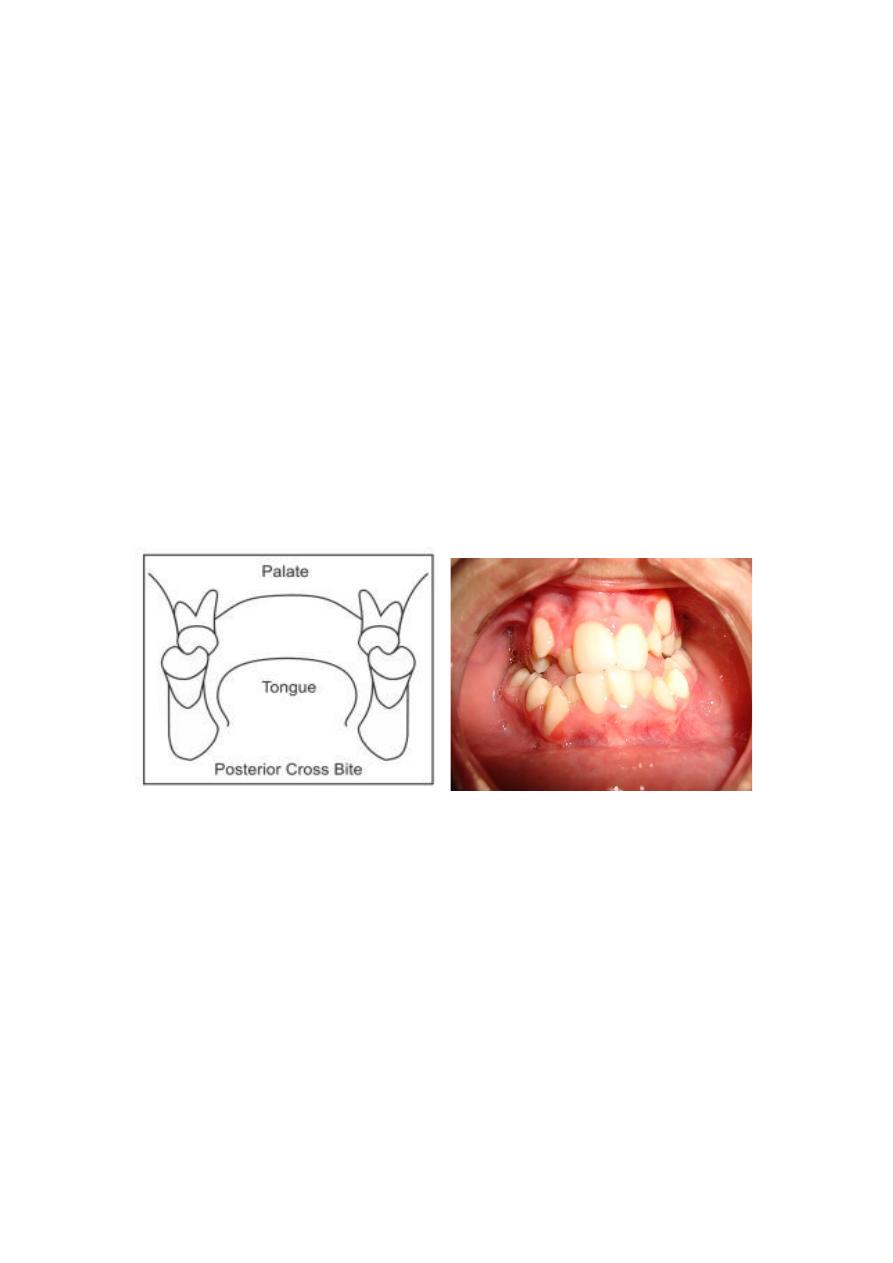
Posterior cross bite(fig.11) is defined as inadequate transversal
relationship of maxillary and mandibular teeth, i.e., the buccal cusps of the
maxillary teeth are in contact with the central fossae of the mandibular
teeth. This malocclusion does not show spontaneous correction, and should
be treated with maxillary expansion as early as possible. The displacement
of a tooth palatally in the maxilla or buccally in the mandible may result in
a localized crossbite and is usually a reflection of crowding.
Posterior crossbite is one of the most prevalent malocclusions in the
primary and early mixed dentition. It is reported to occur between 8% and
22%. It is defined as any abnormal buccal-lingual relation between
opposing molars, premolars or both in centric occlusion.
Fig.11 posterior cross bite.
Classification
Based on the location of the etiologic factors, posterior crossbite can be
a result of dental or skeletal abnormalities, a combination of the two or can
be functional:
1. Dental crossbite is caused by improperly inclined or malpositioned
teeth. Dental cross bites are generally single tooth or sometimes-
segmental cross bites. These usually result from
a. arch length discrepancy
b. abnormal path of eruption.
These are usually not accompanied by any threat to general health of
the patient, the problems arising due to such cross bites are periodontal or
esthetic in nature.

2. Skeletal posterior crossbite is defined as a discrepancy between the
width of the maxilla and the mandible. In general, the more teeth
occlude in crossbite, the greater skeletal component involved.
Bilateral crossbite is mostly a consequence of maxillary skeletal
deficiency.
Skeletal cross bite: include those cross bites, which are primarily due
to mal-positioning or malformation of the jaws. These can be:
a. inherited (e.g. Cross bites seen in patients with Class III skeletal
pattern).
b. congenital (e.g. cleft lip and palate cases).
c. arising due to trauma at the time of birth (e.g. unilateral ankylosis of
the TMJ) or later in life.
Skeletal crossbite can result from one of the following
maxillomandibular combinations:
• Narrow maxilla, normal mandible.
• Normal maxilla, wide mandible.
• Narrow maxilla, wide mandible.
Skeletal cross bites are capable of causing appreciable damage to a
person's health and personality as the appearance may be compromised to
a larger extent
3. Functional cross bites These cross bites are usually caused due to the
presence of occlusal interferences during the act of bringing the jaws
into occlusion. These can be caused by the early loss of deciduous
teeth, decayed teeth or ectopically erupting teeth. If not corrected
early, these can ultimately lead to skeletal cross bites.
Posterior cross bites may be further classified according to the existence
of the cross bite on one side or both sides of the arch as:
• Unilateral cross bite.
• Bilateral cross bite.
Treatment of crossbite
Cross bites-anterior or posterior should be corrected as soon as they are
detected. Some authors believe that the same should be treated during the
deciduous dentition. However, it may be better to treat them as the
permanent teeth begin to erupt into the oral cavity. The child may be too
young and uncooperative at the deciduous dentition stage. Moreover, it is
easier to bring about changes in the mixed dentition stage.
Appliances used
Fixed or fixed-removable appliances used for maxillary expansion to treat
a posterior crossbite fall into 2 basic categories:
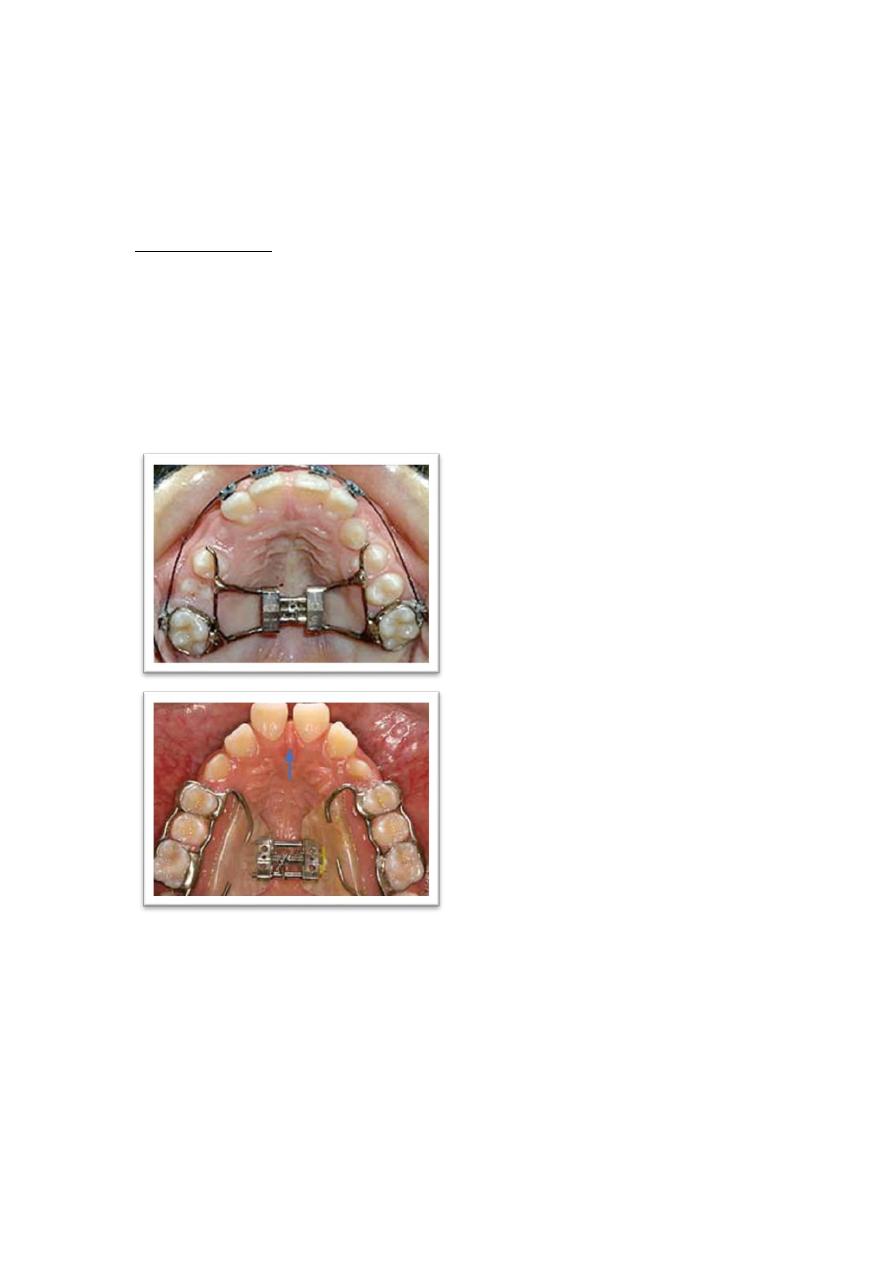
1. Those causing midpalatal suture separation such as Hass- and Hyrax-
type rapid palatal expansion appliances which are employed to
achieve crossbite correction via separation of the midpalatal suture.
(fig.12 and 13)
(fig.12) Hyrax-type expander (fig.13) Hass-type expander
2. Those that usually do not cause midpalatal suture separation. Quad
helices, screw appliances, and Coffin spring achieve expansion via
dental-alveolar movement.

(fig.14) Quad-helix screw-appliance Coffin spring
Scissor bite
Occasionally the upper dental base is very much wider than the lower
and there may be a lingual crossbite or scissor bite. This is usually
unilateral but rarely, in severe cases, it may be bilateral.
Fig.12 scissor bite.