Dental trauma
A pulpectomy involves complete pulp tissue removal from the crown and root and
is indicated when no vital tissue remains. It is also indicated when root maturation
is complete and the permanent restoration requires a post buildup. In the absence of
inflammatory root resorption, treatment is to obturate the canal with gutta-percha.
One of the greatest challenges facing the clinician is the treatment of a nonvital
immature permanent tooth with an open apex. Physiologic root maturation cannot
occur without the presence of vital pulp tissue, apical papilla stem cells,
odontoblasts, and Hertwig epithelial root sheath. Traditional treatment for these
cases was an apexification procedure wherein CaOH was carried to the root apex
to contact vital tissues directly. The CaOH stimulated the formation of a cementoid
barrier against which gutta-percha could subsequently be condensed. Multiple visits
over a period of 9 to 18 months were required, however, and the outcome was a
shortened root with thin walls. Additionally, long-term CaOH therapy has been
shown to weaken the tooth root and increase the likelihood of root fractures.
An alternative to the CaOH apexification technique for managing devitalized
immature incisors is the apical barrier technique using MTA. The material is
condensed into the apical area, and allowed to set. Gutta-percha is then condensed
against the MTA barrier at a subsequent appointment. Though overall treatment
time is greatly reduced, the shortened root and thin walls continue to place the tooth
at risk for subsequent cervical root fracture.
Regenerative Endodontics
An alternative to apexification of necrotic immature teeth termed
revascularization or “regenerative” endodontics. These procedures seek to
replace damaged dentin, root structures, and pulp cells with live tissues that
restore normal physiologic function. The concept is to thoroughly disinfect the
root canal system and then stimulate bleeding from the apical papilla to fill the
root chamber with a blood clot. A host of growth factors in the area then act on

dental stem cells, primarily from the apical papilla, to use the clot as a scaffold
and differentiate into healthy cells of the pulp-dentin complex that can
complete physiologic root maturation.
The technique is to first cleanse the canal by copious irrigation with sodium
hypochlorite or Ethylenediaminetetraacetic acid (EDTA). Owing to the
immature status of the root and thin radicular walls, instrumentation is kept to
a minimum and used mainly to agitate the irrigant. The irrigant is also
activated by placing an ultrasonic tip about 3 mm short of the working length
in the canal to facilitate better debridement of the pulp tissue remnants and to
minimize the substrate for microbial proliferation. The canal space is then
dried using sterile paper points. A triple antibiotic mix of 250 mg
ciprofloxacin, 250 mg metronidazole, and 150 mg clindamycin is prepared to a
creamy paste with propylene glycol as a vehicle. The antibiotic paste is
carefully placed into the root canal system using a Lentulo spiral up to the
cementoenamel junction (CEJ). The access cavity is sealed with a sterile
cotton pellet and glass ionomer cement.
The patient is scheduled for follow-up appointments after 3 to 4 weeks. At the
follow-up appointment, the area is anesthetized with local anesthetic
containing no epinephrine. The antibiotic paste is rinsed out, and a sterile
endodontic file is placed beyond the apex to initiate bleeding. A clot is allowed
to form as close to the CEJ as possible to facilitate root thickening at the tooth
cervix. MTA is then placed against the clot, and the tooth is temporarily sealed
with glass ionomer cement. The final restoration is placed at a subsequent
appointment. Root maturation should be apparent radiographically within
several months
5.
Without pulp exposure:
fragment removal with or without gingivectomy and restore.
With pulpal exposure and immature roots:
Perform a partial pulpotomy to preserve pulp vitality.
Pulp exposure with mature roots:
Perform endodontic treatment then restore with a postretained crown.
Orthodontic or surgical extrusion of apical fragment may be indicated to
expose the margins prior to permanent restoration.
Extraction with immediate or delayed implant-retained crown restoration or a
conventional bridge. Extraction is inevitable in crown root fractures with a
severe apical extension, the extreme being a vertical fracture
If the coronal fragment is stable and immobile (high apical root fracture), no
treatment is indicated. If the coronal fragment is mobile, reposition and
stabilize the fragment with rigid splinting of composite resin and wire or
orthodontic appliances for four weeks;
If the root fracture is near the cervical
area of the tooth, stabilization is beneficial for a longer period of time (up to 4
months).. Root canal therapy should not be initiated until clinical and
radiographic signs of necrosis or resorption are apparent. Even in those cases,
treatment can often be limited to the coronal fragment, because in most
instances the apical fragments maintain their vitality.
Reposition any displaced segment and then splint the involved teeth with a
flexible splint for 4 weeks. Suture gingival laceration if present
3.
Monitor pulpal response until a definitive pulpal diagnosis can be made

4.
Extruded permanent teeth should be repositioned as soon as possible and
splinted for 2 to 3 weeks. It normally takes the PDL fibers this period of time
to reanastomose. Extruded permanent teeth with closed apices will undergo
pulpal necrosis; therefore root canal therapy should be initiated after the teeth
are splinted. Extruded teeth with open apices have a chance to revascularize
and maintain their vitality, so the decision to initiate therapy should be delayed
until clinical or radiographic signs indicate necrosis.
Alveolar bone fractures frequently occur in lateral luxation injuries and can
complicate their management. In the most severe cases, PDL and marginal
bone loss occur. Treatment is to reposition the teeth and alveolar fragments as
soon as possible. A splint should then be applied for 3 to 6 weeks, depending
on the degree of bone involvement. If the apices are closed, the pulps will
likely become necrotic. Again, teeth with open apices should be monitored
until signs of necrosis are evident.
Teeth with incomplete root formation:
Teeth with incomplete root formation:
If the crown remain visible and there is very wide immature apex (>2mm ) the
tooth may be allowed to re-erupt spontaneously . If no movement is noted
within 3 weeks, orthodontic repositioning using light forces should be
employed.
Teeth with complete root formation:
Mature permanent teeth intruded less than 3 mm should be allowed to
reemerge without intervention. If no movement is noted within 3 weeks they
should be
repositioned surgically
or
orthodontically before they
ankylose.Those teeth intruded beyond 7 mm should be repositioned surgically
Soft Tissue Trauma
The soft tissues are often involved during traumatic injuries to the orofacial
area and maybe bruised or lacerated by the impact of teeth against the tissue.
Usually application of pressure with gauze to the injured site should provide
adequate hemostasis. If hemostasis cannot be obtained or the laceration is so
severe the edges are not well opposed, sutures are recommended.
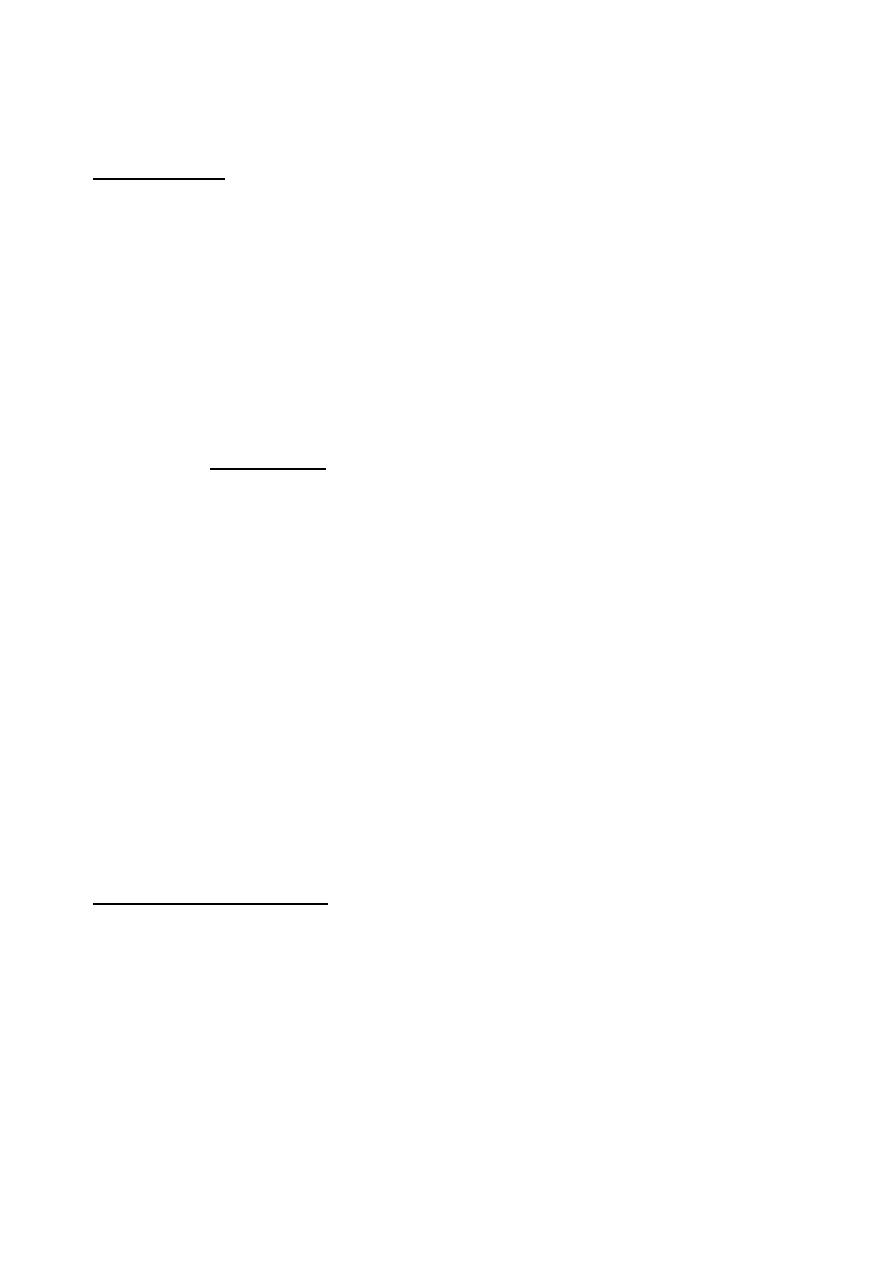
Lips often cushion the teeth during a fall, bearing the brunt of the injury and
resulting in bruises and lacerations. If a laceration is present, it should be
carefully examined to determine whether a foreign object such as a tooth
fragment or gravel has been introduced into the wound.
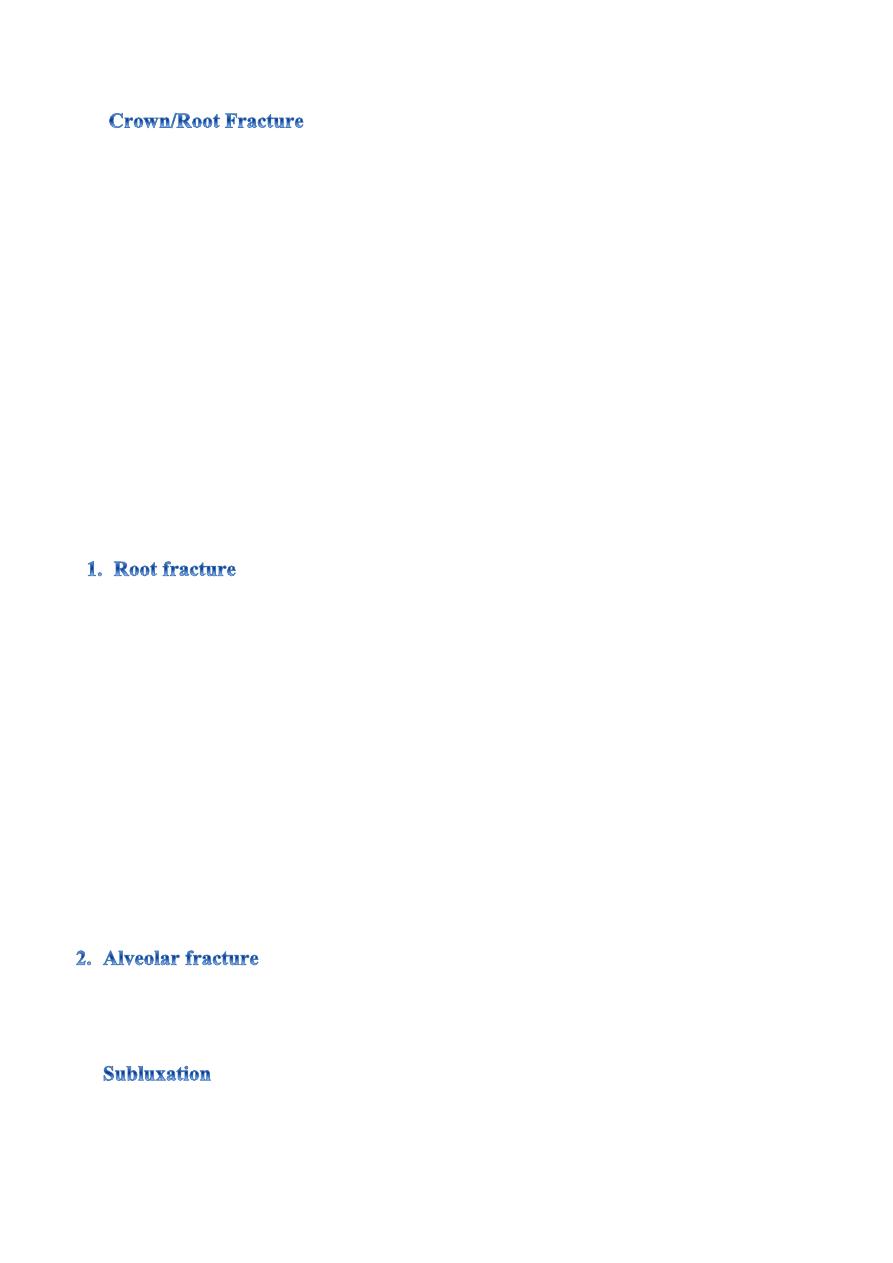
The maxillary labial frena may tear as a result of a fall. This type of injury is
common during falls experienced while learning to walk. However, such an
injury occurring in infants who do not walk or crawl is probably due to an
object being forced into the child’s mouth.
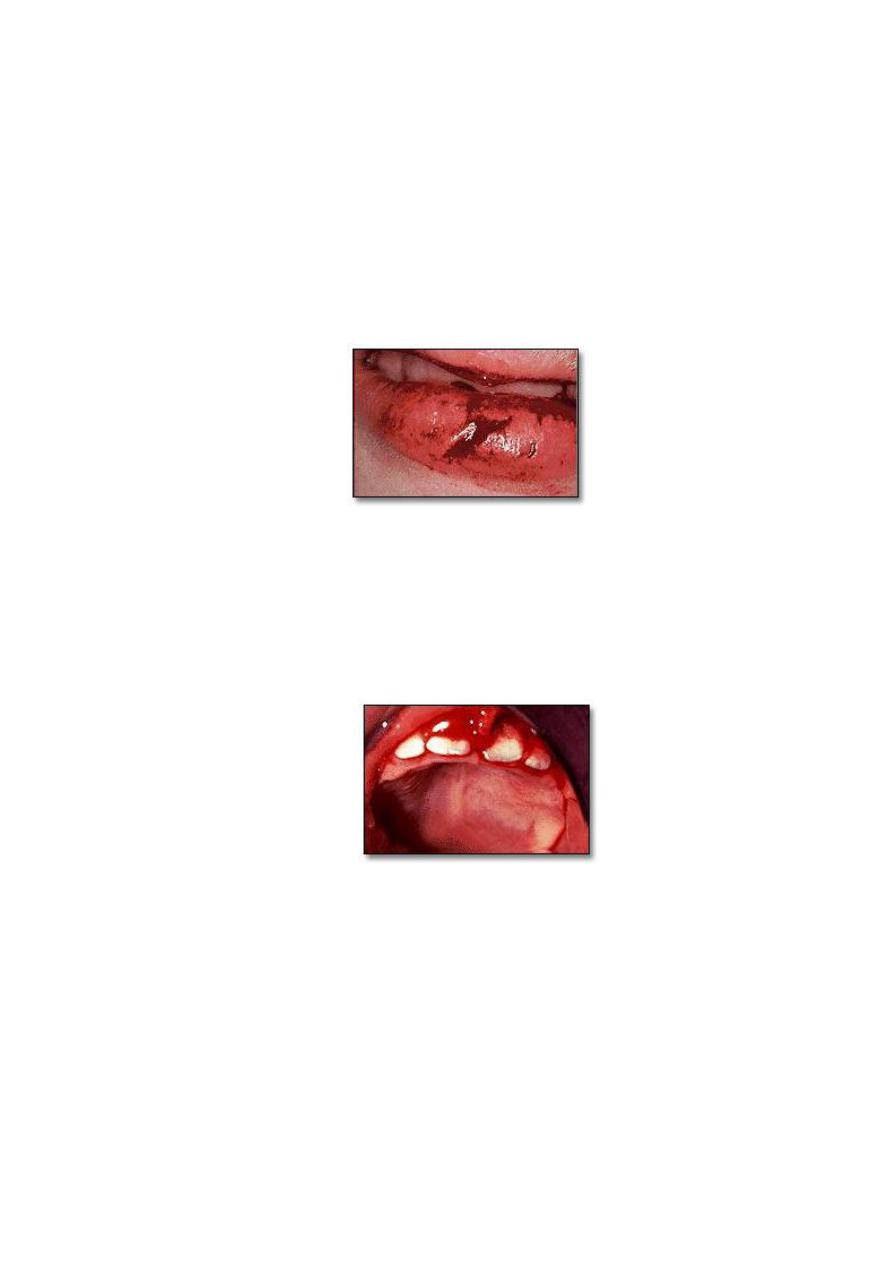
Trauma to the tongue can result in laceration or puncture. Careful examination
of the injury is important since the necessity for suturing is dependent on the
extent of injury.
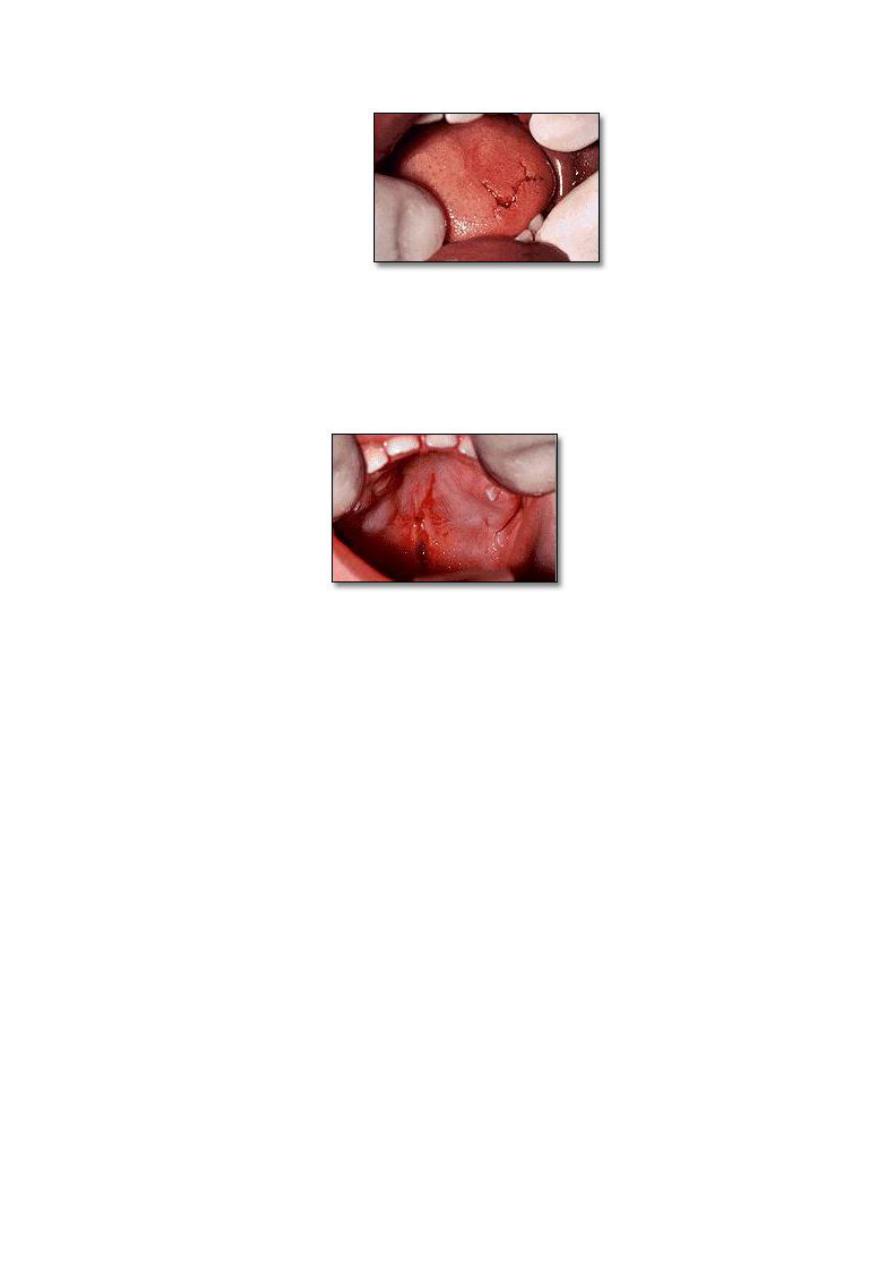
Impalement of the soft palate is commonly found in the child who falls while
holding an object in the mouth, i.e., a stick, pencil or pen, straw or toothbrush.
Most impalement injuries heal spontaneously and do not require treatment,
however the area should be thoroughly explored for foreign body objects and a
prophylactic antibiotic should be prescribed to avoid infection complications.