Open bite:
Ass.Prof.Dr.Zaid AlDewachi
Introduction:
Open bite is a malocclusion that occurs in the vertical plane,
characterized by lack of vertical overlap between the maxillary and
Mandibular dentition. Open bites can occur in the anterior and the
posterior region and are called anterior open bite and posterior open
bite respectively.
Many potential etiologic factors are implicated as causes of open bite
including heredity, unfavorable growth patterns, digit-sucking habits,
tongue and orofacial muscle abnormal function, orofacial functional
matrices and their interaction with the skeletal components, imbalances
between jaw posture, occlusal and eruptive forces and head position. A
detailed understanding of its etiology and developmental process is thus
essential in its management.
Epidemiology
Openbites occur less frequently than deep bites. Severe deep bite
(overbite of 5 mm) is found in nearly 20% of children and 13% of adults,
while open bite (negative overbite >-2 mm) occurs in less than 1%.
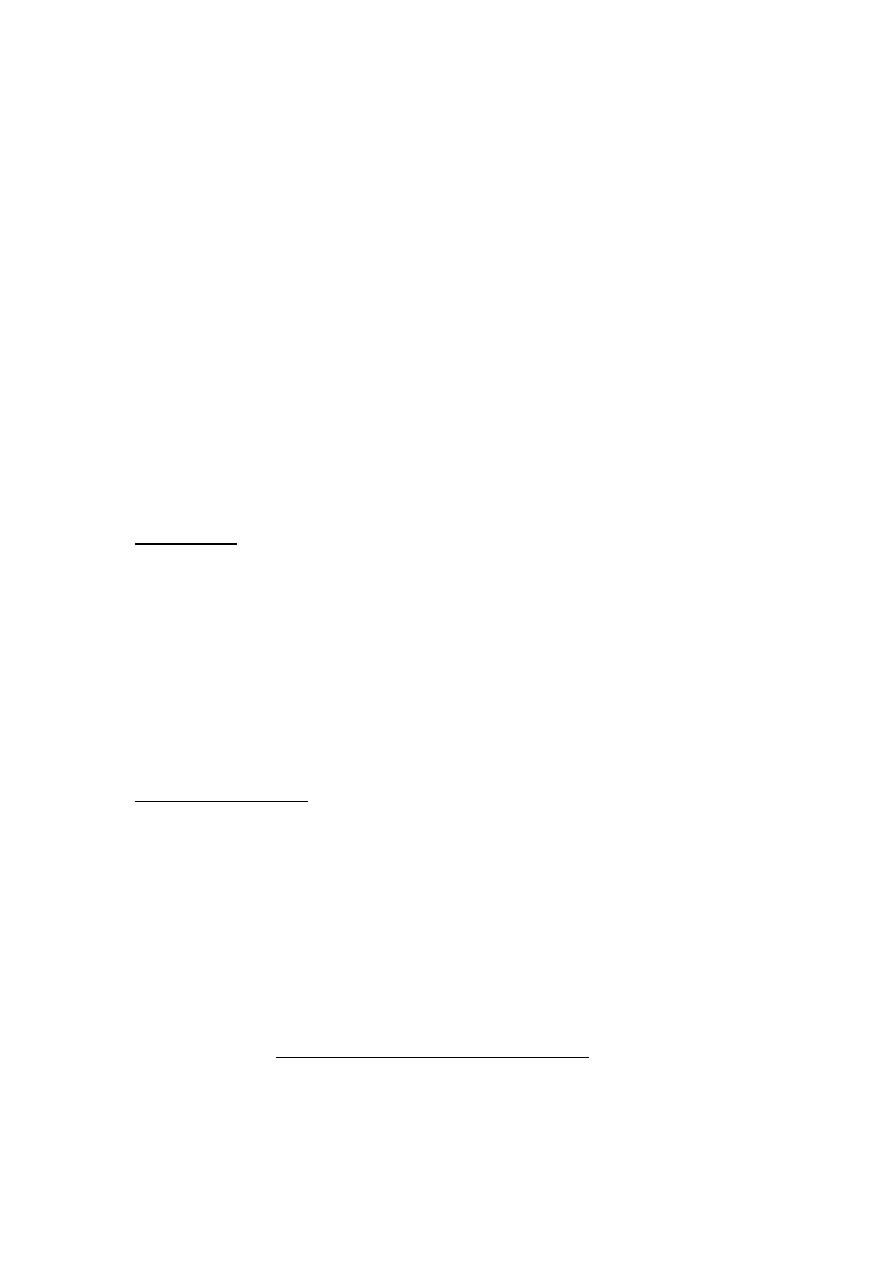
ANTERIOR OPEN BITE
In anterior openbite there is no vertical overlap between the upper and
lower anteriors. Anterior open bites are esthetically unattractive
particularly during speech when the tongue is pressed between the
teeth and lips. The anterior openbites particularly skeletal open bites are
called as “stigmata of malocclusion”
Causes
The etiology of anterior open bite is multifactorial. Anterior open bites
can occur due to variety of hereditary and non-hereditary factors. The
resultant openbite is an interaction between these factors.
The following are some of the etiologic factors responsible for anterior
open bites:
1.
Heredity with genetic disposition Inherited factors such as
increased tongue size, and abnormal skeletal size and growth
pattern of the maxilla and mandible can also be responsible for
open bite malocclusion.
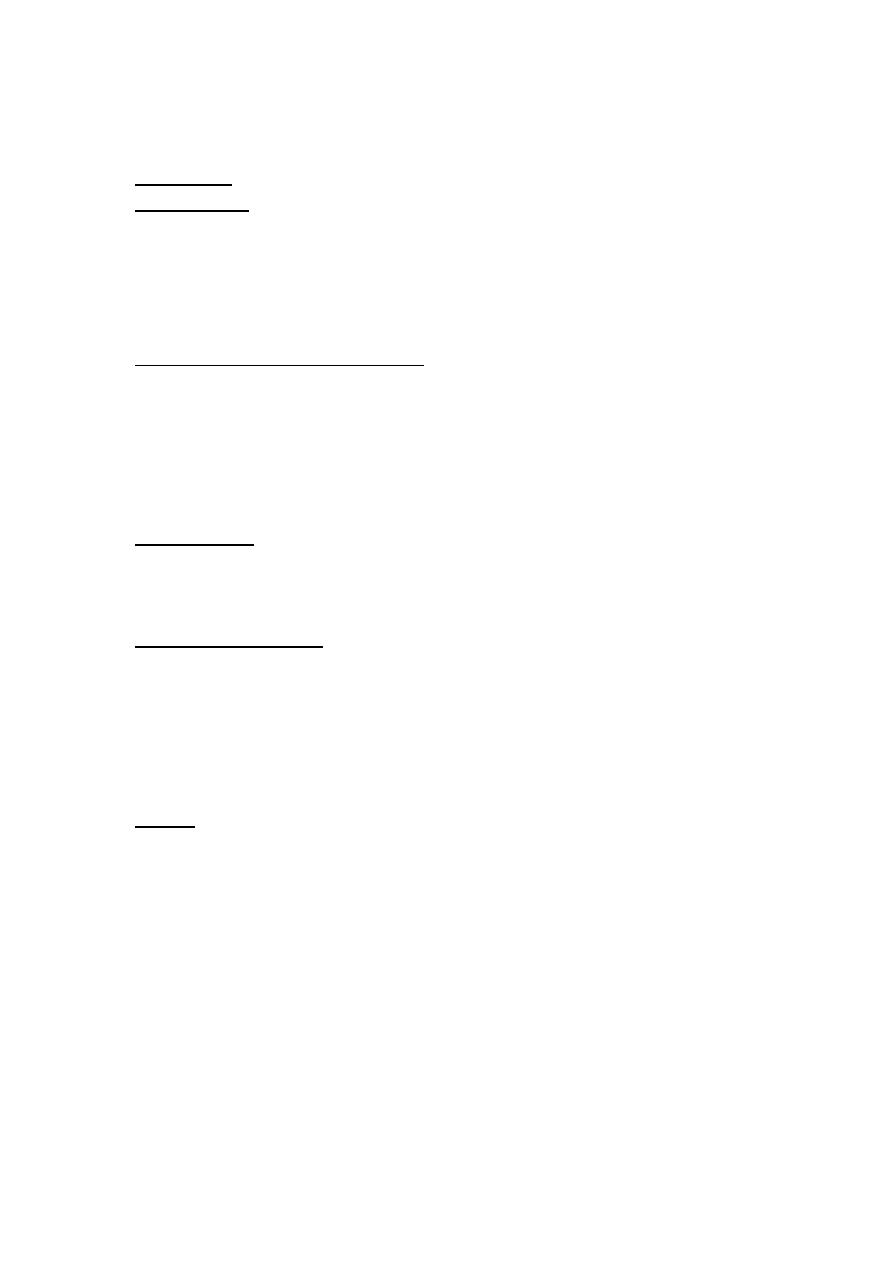
Habits
i. Prolonged thumb-sucking habit is one of the chief etiological factors of
open bite. The posture of thumb positioning, the intensity,and the
frequency of sucking, all have an influence on the nature and severity of
the open bite.
ii. Tongue thrusting is also implicated for some cases of open bite.
Tongue thrusting may develop as a complication of thumb sucking habit.
Sometimes tongue thrusting develops as a compensatory mechanism for
existing open-bite.
Skeletal:
a) An overgrowth or undergrowth of one or more alveolar segments, in
anterior openbites there is undergrowth of the anterior segment with
excessive growth posterior alveolar portion. In posterior openbites there
is undergrowth of the posterior alveolar segment.
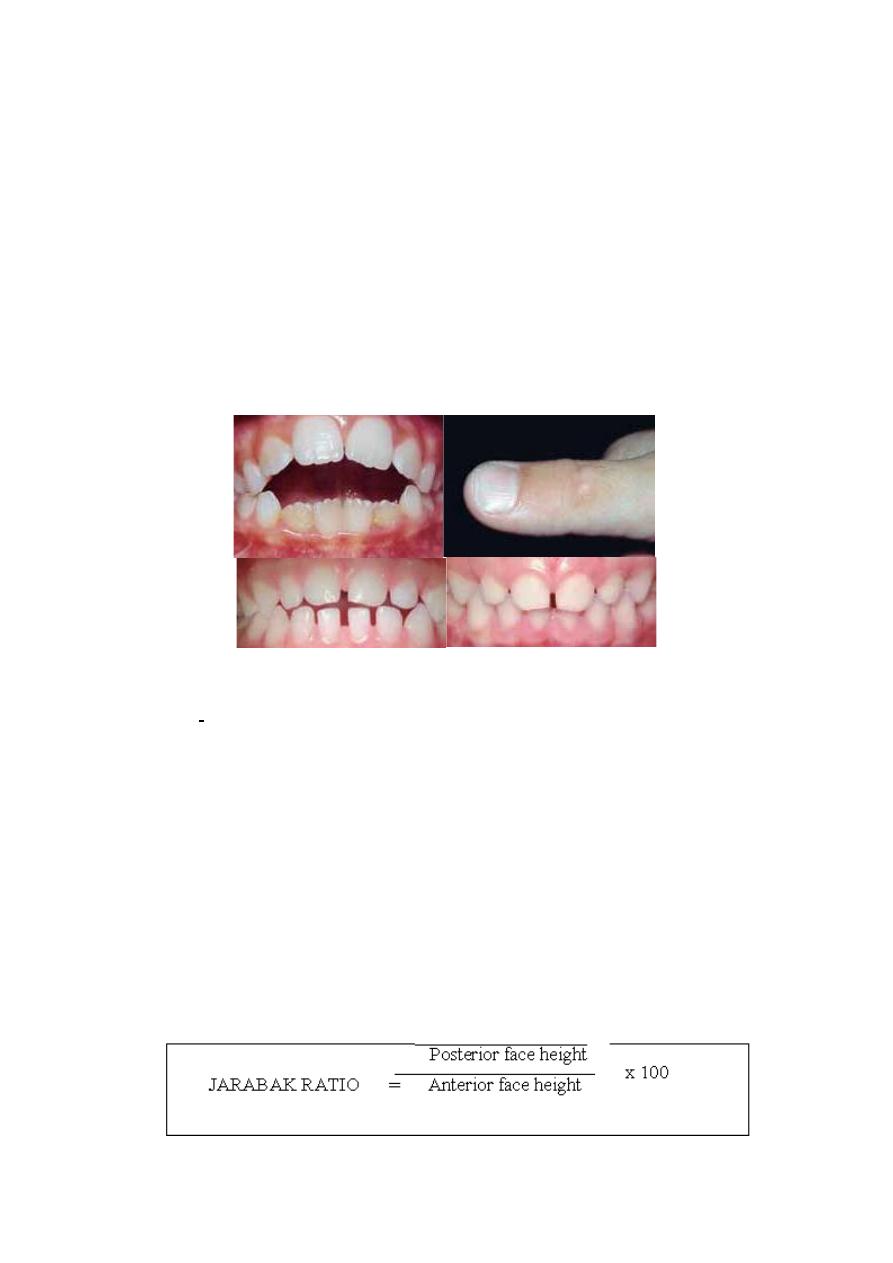
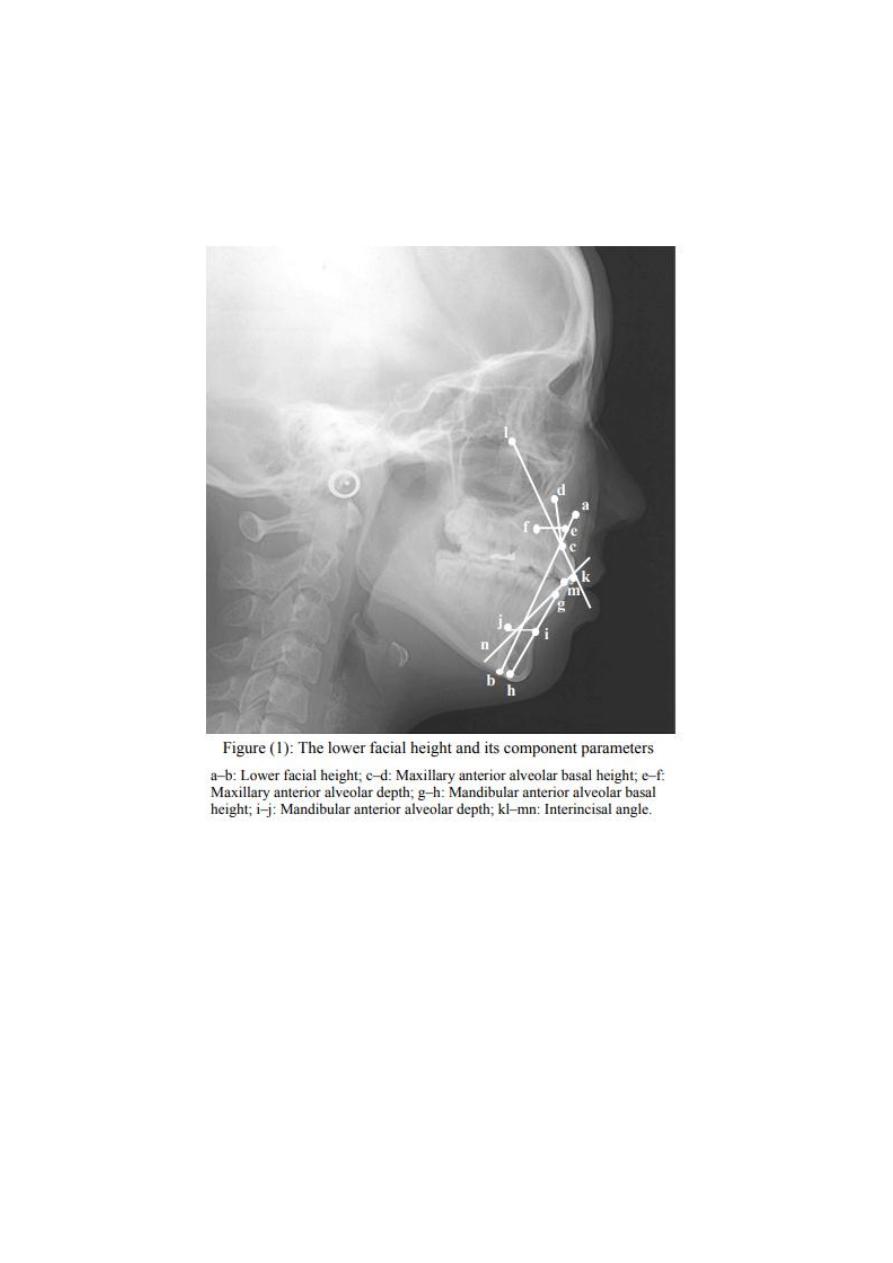
b) Increased anterior and decreased posterior facial height. The
posterior face height (Sella - Gonion) and anterior face height (Nasion –
Menton) are measured on lateral cephalogram with teeth in habitual
occlusion to estimate growth directions according to Recommendations
of JARABAK (1972), a ratio of less than 62 % Expresses vertical growth
pattern and open bite tendency whereas a ratio of more than 65%
increases the likelihood for horizontal vector and deep bite tendency.
c) Vertical growth pattern or backward rotation or clock wise rotation of
the of the lower jaw.
d) Anticlock wise rotation of the maxillary base.
e) Divergent jaw bases
f) Short ramus with long or short body and Increased gonial angle
(articulare—gonian – menton).
Dental
When there is only dental and dentoalveolar involvement, there is
predominance of environmental causes such as thumb or dummy
Sucking habits, mouth breathing, and tongue or lip thrusting in addition
to some local factors such as tooth ankylosis and eruption disturbances
that result from over eruption of the posterior teeth or under
Eruption of the anterior teeth, the periodontal breakdown of anterior
teeth may also give rise to anterior openbites with flaring of teeth.
Classification of anterior open bite
Anterior open bite can be classified as:
a. Skeletal anterior open bite
b. Dental anterior open bite (unilateral,bilateral )
Features of skeletal anterior open bite
a. The patient often has a long and narrow face with marked convex
profile. The esthetics is impaired. A patient with underlying skeletal class
III bases may have concave profile.
b. The patient may have a short upper lip with excessive maxillary incisor
exposure
c. Increase lower anterior facial height and decreased upper anterior
facial height
d. A steep mandibular plane angle (High angle). Thus the angle FMA is
increased and more than 30 degrees. There is clock wise rotation or
backward rotation of the mandible with increased lower anterior facial
height.
e. Small mandibular body and ramus
f. Divergent jaw bases as well as other horizontal cephalometric planes
g. There is upward rotation of maxillary jaw base (The ANS and PNS
plane gives maxillary jaw base).
Features of dental anterior open bite
Dental anterior open bites do not present with the skeletal
complications mentioned above. The following are the features of dental
open bite:
a. Proclined upper anterior teeth.
b. The upper and lower anteriors fail to overlap each other resulting in a
mild open bite.
c. The patient may have a narrow maxillary arch due to lowered tongue
posture due to a habit.
d. There may be spacing between the upper and lower anteriors
Other features
Speech defects can be found with lisping of voice. There may be
associated upper respiratory infections. Lispisng associated with anterior
openbite and spacings.
Diagnosis:
Diagnosis should include a thorough case history pointing to critical
examination towards the presence of any etiological factors like habits.
Hereditary content if present should be noted. The cephalometric
analysis will differentiate a dental from a skeletal component
Treatment of anterior open bite
The diagnosis and treatment of this malocclusion are still controversial.
Many authors agree that the clinician should be able to distinguish an
open bite of dental and dentoalveolar origin from a skeletal open bite so
that treatment is directed towards the cause of the problem.
Anterior open bite in the primary dentition is the most frequent
malocclusion associated with persistent digit and pacifier sucking
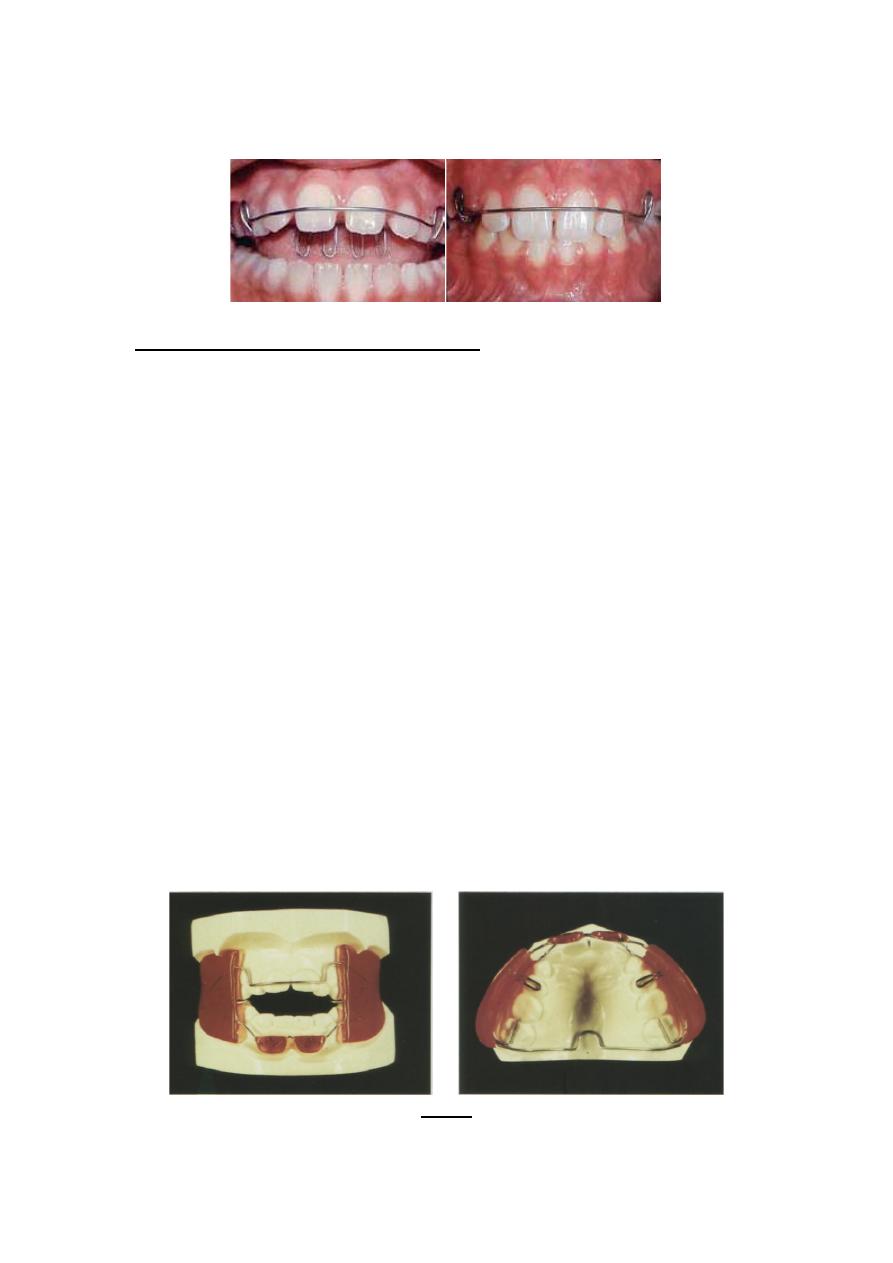
Removal of the etiology of Open bites that have been diagnosed as a
result of habits such as thumb sucking or tongue thrusting, require Their
interception using passive habit breaking appliances. The habit breaker
can be either a removable or a fixed type of crib. Persistence of the
cause will offer a severe limitation in the corrective procedures. Thus, to
allow normal development of the anterior dentoalveolar region, the
palatal crib may be an excellent treatment option, since it prevents
thumb or dummy sucking and avoids tongue thrusting.
The presence of abnormal nasopharyngeal pathology should be ruled
out after referring the patient to an otolaryngist. The control of those
Factors should be given due importance before rushing to correct the
existing open-bite.
Myofunctional and orthopedic therapy:
The open-bites can be intercepted by growth modulation. The aim is to
achieve counterclockwise mandibular rotation for closure of an open
bite, especially if there is remaining growth of the mandibular ramus, in
order to control the increase in anterior face height and achieve
improved occlusal outcomes and a balanced profile. Treatment
approach is directed at vertical control of facial growth and/or ‘real’ or
relative intrusion of the posterior teeth
The maxillary posterior segment can be intruded by an occipital
headgear which rotates the maxilla in clock wise direction thereby
closing the open bite. The Skeletal anterior open bites can be treated
during growth using functional appliances such as F.R-IV or a modified
activator. These appliances incorporate bite blocks interposed between
the posterior teeth, that have an intrusive action on the upper and lower
posterior teeth. Patients exhibiting a downward and backward rotation
of the mandible with increased vertical growth, benefit from therapy
Using a vertical pull head gear with chin cup if treated during the mixed
dentition period. Vertical chin cup inhibits the vertical growth in the
Mandibular posterior dento-alveolar region, It decreases mandibular
plane angle and helps in closure of gonial angle indicating anterior
rotation of the mandible.
(FR-4)
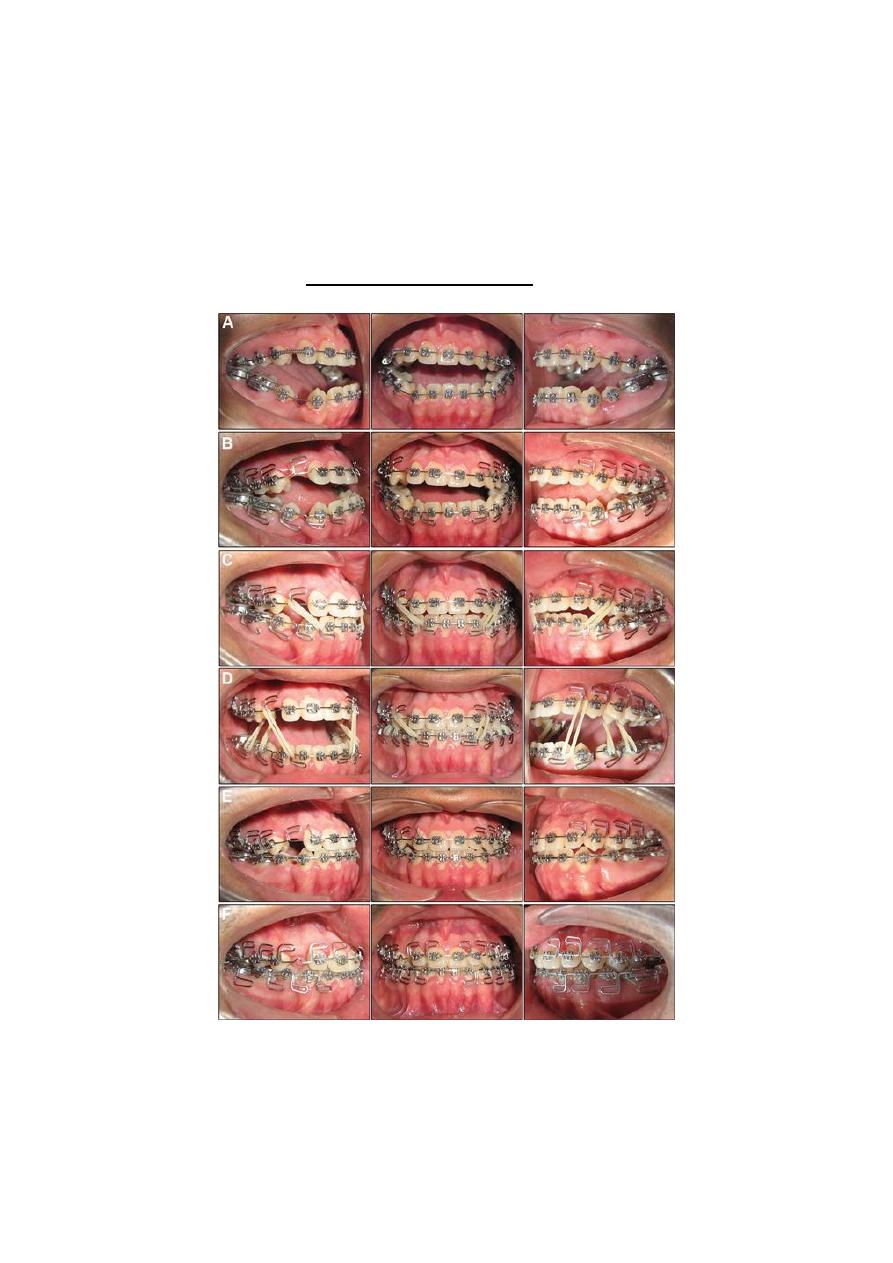
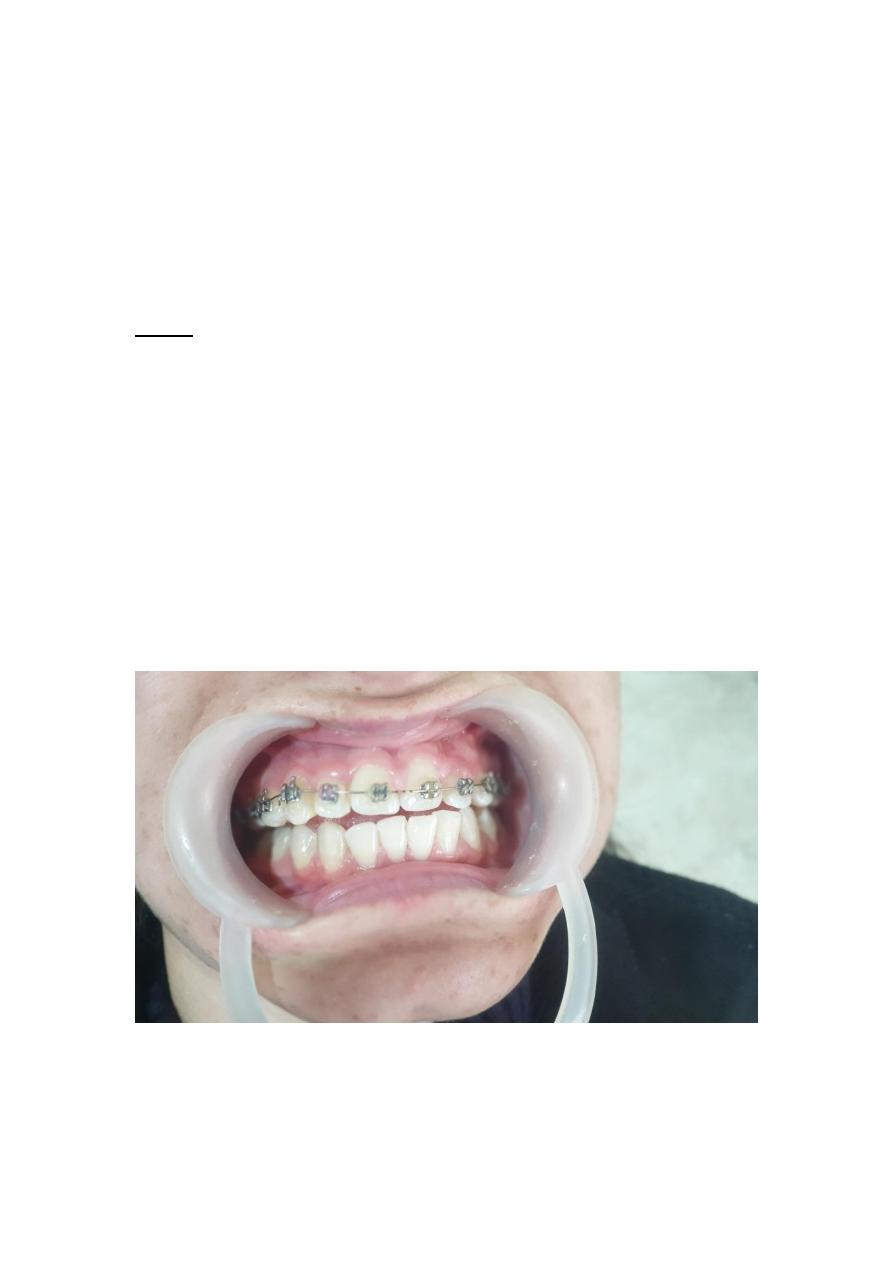
Orthodontic corrective therapy:
Mild to moderate dental open bites can be successfully managed using
fixed mechanical appliances in conjunction with box elastics. This form
of elastic application consists of elastic that is stretched to extend
between the upper and lower anteriors. This brings about extrusion of
the upper and lower anteriors. This form of therapy may not give
Favorable results in severe skeletal open bites.

Surgical correction:
Skeletal open bites in adults are best treated by surgical procedures
involving the maxilla and the mandible. This includes step down of
maxilla and setup of mandible. The surgical treatment depends upon the
other factors like anteriorposterior relationship of maxilla and mandible
Retention:-
The persistence of the etiological agents is the main cause of relapse in
open bite cases. Second factor the continous growth at the molar region
to a little extent and the intrusive effect of etiological factors on the
incisors is cited to be another reason for relapse. Use of open bite type
Of activator or bionator with posterior bite blocks is indicated for long
term retention. High pull head gear with standard retainer may also be
used but is not practically possible.
(Bite Block)
II. POSTERIOR OPEN BITE
Posterior open bite is a condition characterized by lack of contact
between the posteriors when the teeth are in centric occlusion. It mostly
occurs in a segment of the posterior teeth.
Causes of posterior open bite
There are two possible causes of posterior open bite:
1. Mechanical interference with eruption, either before or after the
tooth emerges from the alveolar bone, or
2. Failure of the eruptive mechanism of the tooth so that the expected
amount of eruption does not occur.
Mechanical interference with eruption may be caused by ankylosis of
the tooth to the alveolar bone, which can occur spontaneously or as a
result of trauma, or by obstacles in the path of the erupting tooth.
Examples of such obstructions prior to emergence are supernumerary
teeth and non - resorbing deciduous tooth roots or alveolar bone.
After the tooth emerges from the bone, pressure form soft tissues
interposed (cheek, tongue, finger) can be obstacles to eruption
Ankylosed teeth are usually in infraocclussion and are said to be
submerged. The most commonly submerged tooth is retained lower
decidous second molar.
Treatment
The primary aim of treatment should be to remove the cause. Lateral
tongue spikes are a valuable aid in control of lateral tongue thrust. Once
the habit is intercepted, a spontaneous improvement often follows. The
posteriors can be forcefully extruded.
In cases of posterior open bite due to infraocclusion of ankylosed teeth,
it is best treated by crowns on posteriors to restore normal occlusal
Level.